Types and classification
Symptoms of agnosia vary significantly depending on the damaged area of the cerebral cortex. Most often, one type of perception is affected, but the disease can affect several systems simultaneously. There are several main types of agnosia:
- visual (visual);
- auditory;
- olfactory - impaired perception of smells;
- tactile - change in response to touch;
- taste;
- other specific varieties.
Specialists at the Clinical Brain Institute have extensive experience working with patients with agnosia. It is important to promptly determine the type of disorder and begin maintenance therapy. In addition, the first signs of the disease may indicate serious pathologies of nervous activity.
Visual agnosia
This type of agnosia is characterized by a violation of the perception of information that enters the brain through the visual analyzer. Its symptoms may differ for each patient, depending on the type and location of the damage. So, we can distinguish several specific varieties:
- object-based (develops when the left occipital lobe is damaged) - the patient sees objects well, but has difficulty recognizing them;
- prozolagnosia (damage to the lower occipital region on the right) - inability to recognize even familiar faces;
- color (damage in the left occipital region) - difficulty identifying colors and shades, as well as determining their relationship with certain objects;
- weakness of optical representations (symmetrical damage to the occipital-parietal lobe) - inability to determine the color, shape and size of objects, imagine and describe them;
- simultaneous (pathology of the occipital region) - the patient can concentrate on only one object;
- Balint's syndrome (damage to the occipito-parietal region) - inability to direct the gaze and focus on objects that are in different directions, as well as difficulty identifying objects at near and far distances.
With visual agnosia, the normal functioning of the other sense organs is maintained, and no eye diseases are detected. After rehabilitation at the Clinical Institute of the Brain, the patient adapts to everyday life and can compensate for visual disorders using other analyzer systems.
Optical and optical-spatial agnosias
Patients experience impaired ability to determine the distance between objects and navigate in space. In this category, several specific types of agnosia can be distinguished:
- Depth agnosia (damage to the middle part of the occipital-parietal lobe) - difficulty determining the distance to objects, especially those located in the anterior direction from the patient;
- impaired stereoscopic vision (pathology in the left hemisphere) - inability to recreate a three-dimensional image;
- unilateral (damage to the opposite parietal region) - one half of the space falls out of the field of vision;
- Topographical orientation disorder (parietal and occipital regions) - difficulty finding familiar objects, including home address and objects in one’s own home.
Memory and attention are preserved in optical-spatial agnosia. The patient will need help with everyday life and with new tasks, but proper rehabilitation will allow him to experience minimal discomfort in everyday life.
Auditory agnosia
With this type of agnosia, the functions of the auditory analyzer are preserved. The patient may experience various auditory perception disorders, including:
- simple - decreased ability to characterize and identify familiar sounds;
- auditory-speech - impaired speech recognition, recognition of simple and familiar words;
- tonal - lack of understanding of voice timbre, emotional coloring and other aspects.
All types of auditory agnosia develop when the temporal lobe of the brain is damaged. If the patient is unable to recognize speech, he experiences difficulties in everyday life, while his memory, attention, and the functions of the visual and other analyzers compensate for the impairment.
Somatoagnosia
Somatoagnosia is a disorder in which the patient is unable to identify and recognize parts of his own body. These are complex perception disorders associated with damage to various parts of the right hemisphere of the brain. There are two main types of somatoagnosia:
- Anosognosia is a condition in which the patient denies the presence of an illness. This may be ignoring paralysis of limbs, blindness, or speech disorders.
- Autotopagnosia is a disorder of the ability to recognize individual parts of the body. The patient experiences difficulty when asked to point to an arm, leg, or face; in some cases, there is a feeling of a change in the size of parts of the body. This group also includes somatic allosthesia, in which the patient experiences a feeling of an increase in the number of limbs.
Signs of somatoagnosia may occur in attacks. Thus, in some patients they are harbingers of an epileptic attack, and with proper treatment they are practically invisible and do not cause inconvenience in everyday life. However, they can persist permanently.
Impaired awareness of space and time
This type is considered the rarest and is associated with damage to the occipital lobe of the cerebral cortex. The patient has difficulty determining the passage of time, as well as the speed of movement of any objects. Separately, there is akinetopsia - impaired ability to identify moving objects.
Literature
- Balashova E. Yu., Kovyazina M. S. Neuropsychological diagnostics in questions and answers. — 2nd ed. - M.: Genesis, 2013. - 240 p. — ISBN 978-5-98563-270-5.
- Korsakova N.K., Moskovichiute L.I. Clinical neuropsychology. - 1988. - ISBN 5-211-00508-2.
- Luria A. R. Higher cortical functions of humans. - M.: Moscow University Publishing House, 1962.
- Neuropsychology: Reader, 3rd ed. / Ed. E. D. Chomskoy - St. Petersburg: Peter, 2010. - 992 p. — ISBN 978-5-498-07566-2.
- Polonskaya N.N. Life on the fragments of the visible world: Neuropsychological diagnostics of visual agnosia. - M.: Cogito-Center, 2014. - 88 p. — ISBN 978-5-89353-416-0.
- Simernitskaya E. G. The human brain and mental processes in ontogenesis. - M.: Moscow University Publishing House, 1985. - 188 p.
- Khomskaya E. D. Neuropsychology. — 4th ed. - St. Petersburg: Peter. — 496 p. — ISBN 5-469-00620-4.
Diagnostic methods
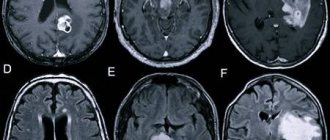
The Clinical Institute of the Brain has all the conditions for a full diagnosis of patients with agnosia. At the initial stage, it is important to determine exactly what difficulties the patient has with the perception of the environment. For this purpose, there are special tests, during which the patient is asked to describe objects, sounds, and point to parts of the body. After determining the type of disorder, it is important to conduct brain imaging using computed tomography or magnetic resonance imaging. This research method will detect neoplasms, heart attacks, vascular damage and other anomalies that can cause agnosia.
2. Reasons
Various areas of the brain, cortical and subcortical, are “responsible” for the processes of perception, analysis and synthesis, comprehension and use of sensory information, and there is no clear boundary or functional division between these structures. If one of these “blocks” is damaged, the work of adjacent ones may be disrupted, and vice versa: damage or functional failure can be compensated to one degree or another by other parts of the brain.
Finally, in some cases, the organic, pathomorphological cause of agnosia cannot be established at all.
The most common factors under the influence of which recognition disorders develop include:
- disorders of cerebrovascularization (blood supply to the brain), incl. ischemic and hemorrhagic strokes and other types of stroke (acute cerebrovascular accidents);
- degenerative-dystrophic and atrophic processes in brain tissue;
- tumor processes;
- traumatic brain injuries;
- some types of mental disorders.
Any dependence on age, gender, region or other additional factors has not been established.
Visit our Neurology page
Treatment of agnosia
Treatment tactics are selected individually. The Clinical Brain Institute employs specialists with extensive experience in treating various types of agnosia. Only some cases require surgery - when tumors, aneurysms, abscesses and other structures are found that need to be removed. In other cases, treatment consists of compensating for lost functions and adapting the patient. For this purpose:
- classes with a speech therapist - special exercises strengthen neural connections and improve perception;
- occupational therapy;
- course of therapy with a neuropsychologist.
Doctors at the Clinical Institute of the Brain insist on full rehabilitation. It can last up to 10 months or more, but qualified medical care will significantly affect the patient’s well-being. Despite the fact that some changes in the structure of the cerebral cortex may be irreversible, it is possible to improve the patient’s quality of life and adapt it in everyday life.
1.General information
Agnosia is a very broad topic, and modern medicine has not fully studied it (like many other aspects of brain functioning). This term refers to numerous types of recognition disorders, differing in etiology and localization of the lesion, clinical picture and prognosis.
It is known that the five basic senses, i.e. The modes of physical sensation in humans are vision, hearing, smell, touch and taste. Any of these channels for obtaining information about the outside world (or about the state of one’s own body) can be disrupted, distorted or turned off completely. Agnosia, which represents the last, extreme version of such a disorder, as well as their partial and distorted forms (paresthesia, illusions, paragnosia, etc.) are studied by several disciplines, primarily clinical: neurology, neurophysiology, psychiatry, neuro- and pathopsychology. There are no exact statistical data on the frequency of occurrence, and they are hardly possible at all, since agnosia is most often observed in the structure of more general psychoneurological disorders.
In the current edition of the International Classification of Diseases (ICD-10, the adoption of ICD-11 is expected in 2021), the independent diagnosis “Agnosia” is placed under the heading of pathological phenomena that do not fall under any profile heading, but in reality this is extremely rare.
A must read! Help with treatment and hospitalization!
Diagnostic measures
Since agnosia is not an independent disease, but only one of the symptoms of neurological nosologies, the main task of diagnosis in this case is to identify the main cause of brain damage
It is also important to determine concomitant disorders of higher mental functions (apraxia, acalculia, etc.), which will suggest the localization of the pathological focus
Non-instrumental techniques
Non-instrumental diagnostics includes the following steps:
- collection of anamnesis of life and illness - is carried out to clarify the nature of the pathology, the presence of previous infections, injuries, vascular “catastrophes”, and the rate of increase in symptoms. Often the patient is not aware of his illness, so the neurologist has to interview the patient’s immediate environment;
- neurological examination - during a physical examination, the doctor can detect signs of focal brain damage (paresis, paralysis, hearing impairment, oculomotor disorders, etc.), intracranial hypertension, which indicate the underlying disease and the location of the pathological focus;
- consultation with an ophthalmologist - congestion in the area of the optic nerve head may indicate the presence of a space-occupying formation in the brain, parenchymal or intrathecal hemorrhage, etc.;
- consultation with a psychiatrist – consists of excluding mental disorders that could serve as the basis for the occurrence of “pseudoagnosia”;
- neuropsychological testing - includes a number of tests that can help determine the type of agnosia and accompanying disorders of higher mental functions.
Instrumental examination methods
Based on the data from the survey and physical examination, the neurologist determines subsequent instrumental diagnostics. Most often, it includes an electroencephalographic study, which allows us to exclude agnosia, such as the aura of an epileptic seizure, and neuroimaging examination methods.
CT and MRI of the brain are the most informative for any pathology of the central nervous system. They make it possible to identify: vascular (stroke, encephalopathy), degenerative brain diseases (Alzheimer’s disease), space-occupying formations (tumor, cyst, aneurysm, etc.), contusion of the brain substance, post-traumatic hematomas and other, diffuse or focal diseases that could lead to the development of agnosia.
Only a qualified specialist can identify the true causes of agnosia and develop adequate treatment and examination tactics.
Autotopagnosia
And this is the second type of disorder related to somatoagnosia. A person’s presence can be recognized by his ignoring half of his body. And many patients simply do not recognize some of its individual parts or incorrectly assess their position in space.
This type of pathology includes:
- Hemisomatoagnosia. A person ignores half of the body, but its functions are partially preserved. The patient simply does not use them. He may “forget” that he has a left arm, leg, etc.
- Somatoparagnosia. The patient perceives the affected part of the body as foreign. He may seriously believe that there is someone else next to him, and it is he who owns his second leg, arm, etc. In severe cases, people feel the “separateness” of the body, as if it were sawn into two parts.
- Somatic allosthesia. The patient feels an increase in the number of his limbs. He may think that he has two or three left hands, for example.
- Autotopagnosia of posture. A person is not able to determine exactly what position his body parts are in. He really doesn't know whether his hand is down or up, whether he's sitting or lying down.
- Disorientation. With this pathology, the patient does not know such concepts as “right” and “left”. This is usually caused by damage to the left parietal lobe.
- Finger agnosia. Specific pathology. If it is present, a person is not able to show on his hand the same finger that the doctor shows on his hand.
Apractoagnosia is also a disorder of this type. This is a special case. People with this disorder have difficulty performing spatially oriented movements. It is difficult for them to make the bed (they place the bedspread crosswise rather than lengthwise), find their way into a room or ward, get their foot in a pant leg, or put on a T-shirt with the right side.
As in any other case, when diagnosing somatoagnosia, neuropsychological methods, samples and tests are used.