Treatment under the compulsory medical insurance policy is possible!
Submit your application
Follow the news, subscribe to our social networks
Details
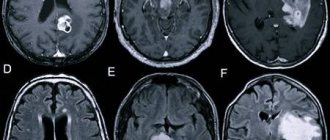
The main cause of cerebrovascular accidents is atherosclerosis of the carotid arteries. Atherosclerotic plaques cause narrowing of the carotid arteries, which is an obstacle to normal blood circulation in the brain. Gradually, a complete blockage of the carotid artery develops, which is called occlusion. Impaired patency of the carotid artery is the main cause of ischemic stroke in the modern world. The risk of developing a stroke if the carotid artery is narrowed symptomatically by 70% or more is about 15% per year.
Many people die or become disabled from stroke every year, although modern vascular surgery can prevent it in most patients. Only regular diagnosis and trust in doctors will significantly reduce the risk of stroke. It is much easier to treat atherosclerosis of the carotid artery than ischemic stroke and its consequences.
Anatomy
Topography of the right carotid arteries and their branches (the lobe of the right ear is pulled upward by a thread): 1 - angular artery;
2 — infraorbital artery; 3 - deep temporal arteries; 4 - buccal artery; 5 - maxillary artery; 6 - inferior alveolar artery; 7 - facial artery; 8 - submental artery; 9 - submandibular gland; 10 - masticatory muscle (cut off); 11—stylohyoid muscle (cut off); 12 - posterior belly of the digastric muscle (cut off); 13 - lingual artery; 14 - superior thyroid artery; 15 - thyroid gland; 16 - common carotid artery; 17 - brachiocephalic trunk; 18 and 28 - sternocleidoid - mastoid muscle (cut off and turned away); 19 - subclavian artery; 20 - scapular-hyoid muscle; 21 - anterior scalene muscle; 22 - phrenic nerve; 23—vagus nerve; 24 - external carotid artery; 25 - internal carotid artery; 26 - hypoglossal nerve; 27 - occipital artery; 29 - posterior auricular artery; 30 - superficial temporal artery; 3 1—transverse artery of the face (cut off); 3 2—middle temporal artery; 33 - parietal branch of the superficial temporal artery; 34 - frontal branch of the superficial temporal artery; 35 - temporal muscle (cut off and turned away); 36 - supraorbital artery; 37 - supratrochlear artery; 38 - dorsal artery of the nose. The right common carotid artery (a. carotis communis dext.) arises from the brachiocephalic trunk (truncus brachiocephalicus) at the level of the right sternoclavicular joint; left common carotid artery (a. carotis communis sin.) - from the aortic arch (see), it is 20-25 mm longer than the right one. General S. a. exit the thoracic cavity through the upper thoracic opening and are directed upward in the fascial perivascular sheaths on the sides of the trachea and esophagus, and then to the larynx and pharynx. More lateral are the internal jugular vein, a chain of deep cervical lymph nodes, between the vessels and behind is the vagus nerve, in front is the upper root of the cervical loop. The scapulohyoid muscle crosses the common S. a. in the middle third (color fig.). Posteriorly, at the level of the lower edge of the cricoid cartilage, on the transverse process of the VI cervical vertebra there is a carotid tubercle (Chassegnac’s tubercle), and the general S. a is pressed against it. for the purpose of temporarily stopping bleeding when she is wounded. At the level of the upper edge of the thyroid cartilage, general S. a. are divided into external and internal S. a. Before division, common S. a. they don't give away branches.
External S. a. in the proximal part it is covered by the sternocleidomastoid muscle, then it is located in the carotid triangle and is covered by the subcutaneous muscle of the neck. Before the artery enters the retromandibular fossa, it is crossed in front by the hypoglossal nerve, the stylohyoid muscle and the posterior belly of the digastric muscle. Deeper lie the superior laryngeal nerve with the styloglossus and stylopharyngeal muscles, which separate the external S. a. from internal. Above the muscles attached to the styloid process, the artery penetrates into the thickness of the parotid gland. Medial to the neck of the articular process of the mandible, it divides into terminal branches - the superficial temporal artery and the maxillary artery.
The anterior branches of the external S. a. are the superior thyroid artery (a. thyroidea sup.), from which the superior laryngeal artery (a. laryngea sup.) departs, the lingual artery (a. lingualis) and the facial artery (a. facialis), sometimes having a common origin with the lingual artery. Posterior branches of S. a. - the sternocleidomastoid artery (a. sternocleidomastoidea), which supplies blood to the muscle of the same name, the occipital artery (a. occipitalis) and the posterior auricular artery (a. auricularis post.). The medial branch is the ascending pharyngeal artery (a. pharyngea ascendens), the terminal superficial temporal artery (a. temporalis superficialis) and the maxillary artery (a. maxillaris).
Thus, external S. a. vascularizes the scalp, facial and masticatory muscles, salivary glands, oral cavity, nose and middle ear, tongue, teeth, partially dura mater, pharynx, larynx, thyroid gland.
Internal S. a. (a. carotis int.) starts from the bifurcation of the common carotid artery at the level of the upper edge of the thyroid cartilage and rises to the base of the skull. In the neck area, internal S. a. is part of the neurovascular bundle together with the internal jugular vein (v. jugularis int.) and the vagus nerve (n. vagus). The artery is encircled medially by the superior laryngeal nerve, in front - by the facial vein, the posterior belly of the digastric muscle, and the hypoglossal nerve, from which the upper root of the cervical loop departs. At the very beginning, internal S. a. lies outward from the external S. a., but soon passes to the medial side and, heading vertically, is located between the pharynx and the muscles attached to the styloid process. Next, the artery bends around the glossopharyngeal nerve.
In the cranial cavity internal S. a. passes through the carotid canal, where it is accompanied by nerve and venous plexuses (plexus caroticus int. et plexus venosus caroticus int.). According to the course of the carotid canal, the internal S. a. makes the first bend forward and inward, then in the carotid sulcus the second bend is upward. At the level of the sella turcica, the artery bends anteriorly. Near the optic canal, the internal S. a. forms a fourth bend upward and posteriorly. In this place it lies in the cavernous sinus. After passing through the dura mater, the artery is located in the subarachnoid space on the lower surface of the brain.
Conditionally internal S. a. divided into four parts: cervical (pars cervicalis), stony (pars petrosa), cavernous (pars cavernosa) and cerebral (pars cerebralis). The first branches extending from the inner S. a. in the carotid canal are the carotid-tympanic branches (rr. caroti-cotympanici), which pass in the tubules of the same name in the pyramid of the temporal bone and supply blood to the mucous membrane of the tympanic cavity.
In the cavernous sinus, the artery gives off a number of small branches that vascularize its walls, the trigeminal ganglion and the initial parts of the branches of the trigeminal nerve. At the exit from the cavernous sinus, the ophthalmic artery (a. ophthalmica), posterior communicating artery (a. communicans post.), anterior villous artery (a. choroidea ant.), middle cerebral artery (a. cerebri med.) depart from the internal carotid artery. and anterior cerebral artery (a. cerebri ant.).
Internal S. a. vascularizes the brain and its dura mater (see Cerebral circulation), the eyeball with its auxiliary apparatus, the skin and muscles of the forehead.
Internal S. a. has anastomoses with the external S. a. through the dorsal nasal artery (a. dorsalis nasi) - a branch of the ophthalmic artery (a. ophthalmica), the angular artery (a. angularis) - a branch of the facial artery (a. facialis), the frontal branch (r. frontalis) - a branch of the superficial temporal artery ( a. temporalis superficialis), as well as with the main artery (a. bаsilaris), formed from two vertebral arteries (aa. vertebrales). These anastomoses are of great importance for the blood supply to the brain when the internal carotid artery is turned off (see Brain, blood supply).
Innervation of the general S. a. and its branches are carried out by postganglionic fibers extending from the upper and middle cervical nodes of the sympathetic trunk and forming a plexus around the vessels - plexus caroticus communis, plexus caroticus ext., plexus caroticus int. The middle cardiac nerve departs from the middle cervical node of the sympathetic trunk, which participates in the innervation of the general S. a.
Pathology
The pathology is caused by malformations of S. a., damage and a number of diseases, in which the wall of the arteries is affected.
Rice. 1. Angiograms of the aortic arch and carotid arteries in various forms of pathology: a - pathological tortuosity of the right common carotid artery (indicated by an arrow); b — nonspecific arteritis (arrows indicate multiple narrowings of the right common carotid and right subclavian arteries); c — atherosclerosis (the arrow indicates a segmental narrowing in the area of bifurcation of the right common carotid artery).
Developmental defects
are rare and usually have a patol character. tortuosity and looping of S. a. The shape and degree of tortuosity of S. a. are different; patol is most often observed. tortuosity of general and internal S. a. (Fig. 1, a). In addition, there are various variations and anomalies of S. a. Thus, sometimes the carotid arteries have a common trunk (truncus bicaroticus), extending from the aortic arch. The brachiocephalic trunk may be absent, then the right common carotid and right subclavian arteries depart from the aortic arch independently. There are also topographic variants associated with anomalies in the development of the aortic arch (see).
In rare cases, from general S. a. the superior and inferior thyroid arteries (aa. thyroid eae sup. et, inf.), pharyngeal ascending artery (a. pharyngea ascendens), vertebral artery fa. vertebra-lis). External S. a. may begin directly from the aortic arch. In exceptional cases, it may be absent, while its branches arise from the artery of the same name passing on the other side, or from the common S. a. Number of branches of external S. a. may vary. Internal S. a. very rarely absent on one side; in this case, it is replaced by the branches of the vertebral artery.
In some cases, with malformations of S. a., accompanied by impaired blood supply to the brain, surgical treatment is indicated (see below).
Damage
are possible as a result of a gunshot wound to S. a., its trauma, for example, with a knife or during surgical interventions on the neck, and are accompanied by massive acute blood loss, thrombosis and the formation of a pulsating hematoma with the subsequent development of a false aneurysm (see).
During surgery for wounds of S. a. First, the proximal part is exposed, and then the distal part. Only after clamping the proximal and distal parts of the artery with atraumatic clamps is the wound area exposed, ligatures are applied above and below the site of injury, a lateral vascular suture or a patch is applied. In cases of the formation of a post-traumatic carotid-cavernous anastomosis, operations are performed to turn it off (see Arterio-sinus anastomosis, carotid-cavernous anastomosis).
Staged treatment of combat injuries to S. a. is carried out according to the same principles as for damage to other blood vessels (see Blood vessels, combat injuries. staged treatment).
Diseases
. Diseases leading to damage to the wall of the S. a. are various forms of nonspecific arteritis, atherosclerosis, fibromuscular dysplasia and, extremely rarely, syphilitic aortitis (see).
In patients with rheumatic heart disease with thrombosis of the left auricle or left ventricle of the heart in the presence of atrial fibrillation, as well as in patients with post-infarction large-focal cardiosclerosis, complicated by a cardiac aneurysm and atrial fibrillation, thromboembolism of S. a. may be observed, edges are sometimes accompanied by focal cerebral symptoms (see Thromboembolism).
Nonspecific arteritis (see Takayasu syndrome) occupies one of the central places among lesions of the brachiocephalic trunk (Fig. 1.6). According to B.V. Petrovsky, I.A. Belichenko, V.S. Krylov (1970), it occurs in 40% of patients with occlusive lesions of the branches of the aortic arch, and no more than 20% of them have damage to S. a . Non-specific arteritis is observed in women 3-4 times more often than in men; It usually occurs before the age of 30, but occurs in both childhood and old age. Its etiology is not fully understood. Nowadays, it is believed that nonspecific arteritis is a systemic disease of an allergic and autoallergic nature with a tendency to damage the walls of arterial vessels of the muscular-elastic type. Damage to all layers of the arterial wall results in productive panarteritis, thromboendovasculitis, disorganization and collapse of the elastic frame and complete obliteration of the vessel. Quite rarely the final stage of development of nonspecific arteritis S. a. is the formation of a true aneurysm as a result of destruction of the elastic membrane of the vessel against the background of arterial hypertension. The proximal part of the general S. a. is most often affected, and the internal and external S. a. remain passable. In patol. the process of nonspecific arteritis may also involve other arteries (see Arteritis, Giant cell arteritis).
Atherosclerosis S. a. It occurs 4-5 times more often in men than in women. Wedge, manifestations of the disease caused by their stenosis or occlusions, develop, as a rule, in people aged 40-70 years. Morphol. the picture of atherosclerosis (see) is characterized by the deposition of lipids in the inner lining of the vessel, the formation of atherosclerotic plaques with their subsequent calcification and ulceration. With ulceration of an atherosclerotic plaque, arterial thrombosis and peripheral embolism with atheromatous masses are often observed. Due to the destruction of the elastic framework of the vessel, true aneurysms can develop. An important factor contributing to the development of true aneurysms of S. a. is the presence of arterial hypertension in the patient. Most often, with atherosclerosis, stenosis of the carotid arteries develops in the area of division of the general S. a. on the internal and external (Fig. 1, c), as well as in the extracranial parts of the internal S. a. Due to the systemic nature of the development of atherosclerosis, it is extremely rare that damage to only one S. is detected. More often, a bilateral process is observed, leading to occlusion, as well as the presence of atherosclerotic stenosis and occlusions in the aorta and main arteries of other organs.
There are more and more reports of the defeat of S. a. according to the type of fibromuscular dysplasia observed in women aged 20-40 years. Some researchers associate this disease with congenital dysplasia of smooth muscle cells of the artery wall, while others tend to consider this disease acquired. Morphologically, fibromuscular dysplasia reveals fibrosis of the muscular layer of the artery wall, areas of stenosis, alternating with areas of aneurysmal dilation. In some cases, either stenotic or aneurysmal forms of fibromuscular dysplasia are detected. Most often, fibromuscular dysplasia is observed in the extracranial parts of S. a., and there is often bilateral damage.
Stenosis of S. a. can also be caused by extravasal factors, among which the most common is a tumor of the carotid gland - chemodectoma (see Paraganglioma). It is extremely rare to observe extravasal compression of S. a. neck tumors and scar processes resulting from inflammation and trauma in this area.
A feature of stenotic lesions of the brachiocephalic trunk, and in particular S. a., is the discrepancy between the wedge, manifestations of impaired blood supply to the brain and the severity of the stenotic process in the arteries. This is due to the large compensatory capabilities of cerebral circulation, a feature of which is the presence of many collateral pathways (see Vascular collaterals). The critical degree of narrowing of the S. a., in which the phenomenon of insufficiency of blood supply to the brain may occur, is a decrease in its lumen by more than 75%. However, this degree of stenosis of S. a. and even its occlusion does not always lead to acute insufficiency of blood supply to the brain with a wedge, a picture of cerebrovascular accident (see). With S.'s lesions. There are four wedges, stages of cerebral ischemia: I - asymptomatic, II - transient, III - chronic. cerebral vascular insufficiency, IV - residual effects of cerebrovascular accident. Treatment of occlusive and stenotic lesions of S. a. depends on the stage of cerebral ischemia, which is important for determining indications for surgery (see below).
Treatment of carotid artery stenosis
The most common treatment for stenosis is artery stenting. Stenting is a surgical treatment method, therefore, like any other surgical intervention, it requires a highly qualified doctor in diagnosis, deciding on the need/possibility of surgery and direct insertion of the stent. A stent is a metal frame inserted directly into an artery. At the point of narrowing, it unfolds and expands the walls of the vessel as necessary. The stent remains in the artery. Only in the first days its presence can be inconvenient due to changes in blood flow, but over time the patient stops feeling it and returns to normal life without the risk of a stroke. But of course, the doctor will give certain recommendations for further lifestyle in order to prevent re-stenosis.
Our doctors understand the importance of high-quality patient management and postoperative monitoring, so by contacting us, you can count on an integrated approach to diagnosis, treatment and the postoperative period. To implement this approach, the neurology department of the Federal Scientific Research Center has a powerful diagnostic base and a strong team of specialists with extensive experience in the treatment of stenosis, who additionally undergo advanced training courses on a regular basis. The department closely cooperates with the cardiac surgery service and the department of vascular surgery, which is separated into a separate unit.
The advantage of our center is the provision of a full range of services to our patients in one place, starting with an initial consultation, which you can sign up for by phone or through a special form on the website.