The sigmoid colon is the terminal section of the colon that continues into the rectum. In oncology, malignant neoplasms of this location are called cancer of the rectosigmoid junction. Together with colon cancer, they are collectively called colorectal cancer.
- Risk group
- Symptoms
- Staging and classification of sigmoid colon cancer
- Metastasis
- Diagnosis of sigmoid colon cancer
- Treatment
- Chemotherapy treatment of sigmoid colon cancer
- Prognosis for sigmoid colon cancer
In the vast majority of cases, a malignant tumor of the sigmoid colon is represented by adenocarcinoma. It accounts for 90-95% of all detected malignant neoplasms. The remaining tumors are represented by the following options:
- Signet ring cell.
- Small cell.
- Squamous.
- Medullary.
- Undifferentiated.
Risk group
Currently, several risk factors have been identified, the presence of which increases the likelihood of developing malignant tumors in the sigmoid colon. These include:
Nutritional Features
The following dietary habits increase the likelihood of developing colorectal cancer:
- Excessive consumption of animal fats and red meat.
- Insufficient content of plant fiber in the diet.
- Regular alcohol consumption.
- Excessive nutrition.
It has been proven that colorectal cancer is diagnosed much less often in vegetarians than in people with a standard diet. For some time it was even considered that meat is the main carcinogen for the intestines and leads to the formation of malignant tumors. The modern theory is based on the fact that plant fibers, which are rich in the diet of vegetarians, cleanse the intestines and do not allow its contents to stagnate. This reduces the contact of the intestinal epithelium with carcinogens and prevents its malignant transformation.
The second risk factor is the presence of polyps . In the vast majority of cases, intestinal cancer develops as a result of malignancy of adenomatous polyps. Moreover, the longer it exists and the larger its size, the more likely its malignant degeneration.
Heredity . The role of hereditary predisposition has been proven in relation to two syndromes: familial adenomatous polyposis (FAP) and Lynch syndrome - hereditary non-polyposis colon cancer. Hereditary cancer accounts for 5-7% of cases of malignant tumors of this localization.
Other risk factors:
- Inflammatory diseases of the large intestine - ulcerative colitis, Crohn's disease.
- History of breast and ovarian cancer.
- Immunodeficiency diseases.
Symptoms
The insidiousness of malignant tumors of the sigmoid colon is that in the initial stages there are no signs of the disease. The clinical picture unfolds when the process enters stages 3-4.
In this case, general and local symptoms are distinguished. Common symptoms include weight loss, chronic fatigue, increased fatigue, pallor and pasty skin (against the background of chronic iron deficiency anemia).
Local symptoms include:
- Abdominal pain. Pain can have various causes, from impaired intestinal motility to tumor growth into adjacent tissues and organs.
- Impaired stool regularity. Patients are bothered by chronic constipation, which is replaced by foul-smelling diarrhea. This occurs due to the fact that feces accumulate above the tumor site, which, in turn, leads to increased fermentation and putrefaction processes, the intestinal contents liquefy, and constipation is replaced by diarrhea. Due to inflammation of the intestinal wall and injury to the tumor, there may be streaks of blood in the stool. When the intestinal lumen is obstructed (blocked) by a tumor, intestinal obstruction develops, which is accompanied by cramping pain, bloating, increased symptoms of intoxication, nausea and vomiting. This condition requires emergency hospitalization in a surgical hospital for immediate medical care.
In addition, signs of sigmoid colon cancer may include:
- Increased gas formation.
- Nausea and bloating.
- Discharge of mucus, blood or pus from the anus.
Possible complications
Possible complications:
- bleeding due to inadequate hemostasis;
- failure of postoperative wound sutures or anastomosis;
- infectious complications (life-threatening conditions such as peritonitis and sepsis may develop);
- dynamic intestinal obstruction (intestinal paresis);
- adhesive disease;
- postoperative hernia.
A sigmoidectomy is a major surgical procedure. However, if the operation is performed correctly by qualified surgeons and the patient follows all recommendations, it is possible to achieve a good quality of life for the patient after resection.
Staging and classification of sigmoid colon cancer
Based on the type of tumor growth, exophytic and endophytic cancer are distinguished. Exophytic tumors grow into the intestinal lumen and have the appearance of a nodular formation or growth. If they grow excessively, they can obstruct the intestinal lumen, causing intestinal obstruction.
The endophytic, or infiltrative form of cancer is characterized by the fact that it grows in the thickness of the intestinal wall. The tumor can circularly cover the intestinal wall, narrowing its lumen, which also causes intestinal obstruction.
Staging of the disease is carried out based on data on the extent of tumor spread:
- carcinoma in situ - malignant cells are found only in the superficial layer of the intestinal mucosa.
- Stage 1 - the tumor grows into the intestinal mucosa and reaches the submucosa and muscle layer.
- Stage 2 - cancer infiltrates the entire intestinal wall and can extend beyond its limits, but does not yet metastasize.
- Stage 3 - metastases appear in regional lymph nodes. The tumor can be of any size.
- Stage 4 - there are distant metastases, or the tumor spreads throughout the peritoneum (peritoneal carcinomatosis).
Metastasis
The following methods of metastasis are typical for malignant tumors of the sigmoid colon:
- Lymphogenic - through lymphatic vessels, malignant cells first reach regional lymph nodes, and then spread further to more distant groups. For example, the supraclavicular nodes may be affected.
- Hematogenous route - malignant cells spread through blood vessels. The liver and lungs are the first to be affected. If the patient has undifferentiated cancer, bone marrow metastases may occur.
- Implantation metastasis - when a tumor extends beyond the intestinal wall, nearby organs and tissues can be affected. In this way, multiple peritoneal metastases, or peritoneal carcinomatosis, are formed.
Kinds
There are more than ten types of malignant processes in the sigmoid colon. In 80% of cases, patients are diagnosed with adenocarcinoma. The level of its malignancy depends on the type. Highly differentiated oncology is considered less dangerous, and undifferentiated oncology is considered the most dangerous.
Remember: even when a cancer fits several specific categories and types, its further development can still be unpredictable - both negatively and positively.
Diagnosis of sigmoid colon cancer
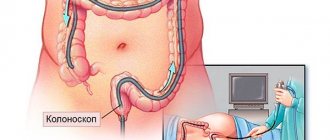
The most informative method for diagnosing sigmoid colon cancer is colonoscopy with biopsy. The procedure involves a complete examination of the entire surface of the colon using special endoscopic equipment.
A shortened version of colonoscopy is rectosigmoidoscopy, in which only the final stage of the large intestine is examined - the rectum and sigmoid colon.
Both diagnostic methods make it possible to detect a tumor of the sigmoid colon, assess its size, the likelihood of complications, and take a piece of tissue for subsequent histological examination. To obtain enough material to verify the tumor, a biopsy is performed from several points. The results obtained are necessary for treatment planning.
If it is impossible to perform a total colonoscopy at the diagnostic stage, it must be done within 3-6 months after the operation, since there is a risk of synchronous malignant neoplasms that are localized in areas inaccessible during rectosigmoidoscopy. If a total colonoscopy is not possible after surgery, CT colonography or irrigoscopy is performed.
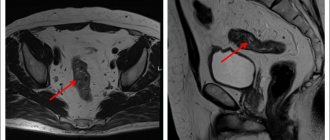
As part of the clarifying diagnosis, a CT scan of the abdominal cavity and chest is performed. This study will differentiate the stage of the disease and detect regional and/or distant metastases. CT can be partially replaced by ultrasound of the pelvic organs, abdominal cavity and retroperitoneal space.
1.General information
Thanks to active educational and preventive activities carried out by the World and national health organizations in developed countries, the population is gradually realizing the reality and individual significance of the danger posed by intestinal cancer. This danger is not at all exaggerated; rather, on the contrary: it is greatly underestimated due to inertia of thinking and a tendency to take an attitude (“What happens, cannot be avoided, but there is no time to run around and just get examined anyway”), due to distrust of doctors (who supposedly “just want to cut”); due to the abundance of all kinds of “advisers” on the Internet and the availability of over-the-counter pills, as well as other means, so to speak, fast medicine - which, by the way, are sometimes more dangerous than the disease itself.
Meanwhile, colorectal cancer occupies one of the leading positions in cancer statistics, and in the absence of adequate radical treatment is characterized by high mortality, along with such deadly types of pathology as heart disease and vascular accidents of the brain. Any adult living in the modern world is at risk - a world that is very comfortable, but which no longer has practically anything in common with the natural human environment.
The large intestine consists of several sections that differ in morphological and functional aspects.
The longest section is called the colon; in turn, it is divided into the ascending, transverse, descending and sigmoid colon; the latter is the transition to the final, distal section of the gastrointestinal tract - the rectum. The sigmoid colon has a characteristic curved shape (which is why it got its name) and serves as a compartment for the final thickening and formation of feces, which slow down somewhat when passing through the gastrointestinal tract. The anatomical and functional features of this section of the large intestine determine the increased (compared to other sections) likelihood and clinical uniqueness of tumor processes, benign or malignant neoplasms.
A must read! Help with treatment and hospitalization!
Treatment
The key treatment for malignant tumors of the sigmoid colon is radical surgical removal. In the early stages (stages 1-2), it is recommended to give preference to gentle, minimally invasive endoscopic operations. In other cases, resection of the sigmoid colon is indicated within healthy tissues, departing from the edge of the tumor by at least 5 cm. Also, tumor-affected tissues, in particular, regional lymph nodes, are removed en bloc. The radicality of the operation must be confirmed by urgent histological examination for the presence of tumor cells at the cutting edges.
Radical surgical treatment can be carried out in 1 or 2 stages. In a one-stage operation, the tumor is removed and the integrity of the intestine is restored through anastomosis.
If this is not possible, two-stage operations are performed. After the tumor is removed, the afferent part of the intestine is removed to the anterior abdominal wall (a colostomy is formed, through which bowel movements will be carried out), and several months after the end of treatment, reconstructive operations are performed and the colostomy is removed.
If radical excision of the tumor is not possible, perioperative chemotherapy is considered, which is designed to reduce the size of the tumor and make it resectable. If this does not happen, palliative operations are performed, and the patient's main treatment is chemotherapy.
If there are distant metastases, they are also recommended to be removed surgically. Preference is given to one-stage operations, when the primary lesion and metastases are removed during one operation. If the metastases are unresectable, chemotherapy is given and then the option of surgical removal is reconsidered.
Nutrition after surgery
After surgery on the sigmoid colon, patients at the Yusupov Hospital are provided with dietary nutrition. The chefs prepare dishes from quality ingredients. They contain a sufficient amount of vitamins and minerals. The menu includes kefir, yogurt, bifido products, fresh vegetables and fruits. All dishes are prepared using gentle technologies: steamed, boiled, baked in the oven or grilled. If indicated, the food is crushed. Patients eat regularly, in small portions.
During the rehabilitation process, the patient should follow certain rules:
- eat only fresh foods;
- products must contain a sufficient complex of vitamins and minerals;
- reduce meat consumption to a minimum;
- consume kefir, yogurt, and bifido products more often;
- eat more fresh vegetables and fruits;
- include cereal porridges and products made from wholemeal flour with bran in the menu;
- periodically include boiled or steamed sea fish in the menu;
- Take food in crushed form, chew thoroughly;
- do not overeat, eat small meals and regularly.
Chemotherapy treatment of sigmoid colon cancer
Chemotherapy for sigmoid colon cancer can be used as part of a combination treatment. In addition, it can be used as an independent method of therapy for unresectable tumors or when it is impossible to perform surgery due to general contraindications.
As part of combination treatment, adjuvant chemotherapy is performed. The feasibility of its use is determined based on the stage of the tumor and the results of an urgent intraoperative examination of the removed intestinal fragment for the presence of malignant cells.
As part of adjuvant chemotherapy, fluoropyrimidine therapy (5-fluorouracil, then 5 FU) is used together with 3rd generation platinum drugs (oxaliplatin). If the patient develops severe complications from two-component regimens, therapy is continued with fluoropyrimidines in monotherapy. The goal of adjuvant chemotherapy is to destroy remaining tumor cells and prevent relapses of the disease.
Independent chemotherapy is palliative in nature and is aimed at containing the tumor process, prolonging the patient’s life and improving its quality.
In addition to regimens with oxaliplatin and 5-FU, regimens with irinotecan are used. Treatment may be supplemented with targeted drugs. In the absence of BRAF and RAS mutations, cetuximab and panitumumab are used. Bevacizumab can be prescribed regardless of the presence of mutations, but it is effective only in conjunction with cytostatic therapy. Cetuximab and panitumumab can be used as 3rd line monotherapy.
Rehabilitation period
The rate of recovery after surgery depends on the volume of intervention performed and the general condition of the body. The rehabilitation period is also affected by the patient’s compliance with the medical and protective regime.
For the first day of the postoperative period, the patient is in the intensive care unit. Antibacterial, anti-inflammatory and analgesic drug therapy is carried out. Chemotherapy drugs may be administered according to indications.
Diet after resection:
- 12-24 hours after surgery, drinking water and unsweetened tea is allowed;
- It is necessary to expand the diet gradually. During the first week, the diet should consist only of liquid and pureed food;
- gradually you can include a small amount of solid foods in the menu;
- the patient will eat small portions 5-6 times a day;
- after a month, the patient can gradually return to his usual diet, but completely eliminate fatty, smoked, spicy and alcohol;
- with a properly selected diet there should be no digestive disorders.
To speed up rehabilitation, patients are recommended to engage in therapeutic physical education. The physiotherapist selects the volume and type of exercises individually for each patient.