Carcinoid is a slow-growing tumor that develops from cells of the neuroendocrine system, mainly in the gastrointestinal tract (cecum, stomach, small intestine, colon, rectum) or lungs. It produces a hormone (serotonin) that causes symptoms such as diarrhea or facial flushing (carcinoid syndrome).
In 50-60% of cases, carcinoids are located in the appendix area. The tumor is usually benign. Only when the size is more than one centimeter does the carcinoid become malignant. In order not to miss the moment of tumor growth, it is recommended to undergo detailed diagnostics in our clinic in Germany.
Symptoms of carcinoid tumor of the appendix
Increased serotonin production due to carcinoid causes a decrease in tryptophan and leads to niacin deficiency (pellagra), dermatitis, dementia and diarrhea.
Serotonin is a neurohormone of the nervous system. Especially when metastases form, the so-called carcinoid syndrome occurs, which is expressed by rapid redness of the facial skin and accompanying manifestations:
- rapid heartbeat;
- sweating;
- breathing problems;
- cramping pain in the abdomen;
- diarrhea.
Diagnosis of the disease
Most carcinoid tumors of the appendix are discovered incidentally during surgery performed for other reasons. To diagnose carcinoid, a blood test is performed to determine the level of free hormones. When hormones break down, increased concentrations of certain substances are formed, for which a urine test is performed.
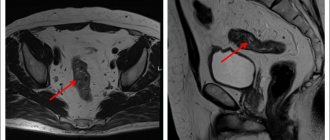
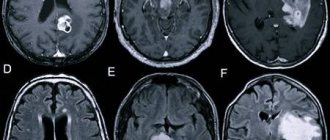
To determine the exact position and size of a neuroendocrine tumor of the appendix, imaging methods are used:
- Computed tomography (CT)
- Magnetic resonance imaging (MRI)
- PET-CT
- Ultrasound examination
- Somatostatin receptor scintigraphy
- X-ray
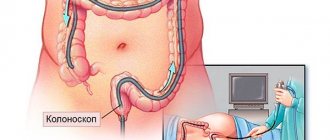
- in some cases, colonoscopy.
To confirm the diagnosis, a tumor biopsy is performed.
Treatment
Surgical treatment The main treatment method for NET is surgery. Possible options for surgical intervention are determined by the location of the tumor, the presence or absence of metastases and complications of the tumor process. However, symptom control during surgical treatment is not always achieved !
Non-drug treatment Monitoring the manifestations of carcinoid syndrome: avoiding stress, alcohol, following a diet.
Drug treatment
Biotherapy:
- synthetic analogues of somatostatin: solution for injection Octreotide and lyophilisate for the preparation of a suspension for intramuscular administration of prolonged action Octreotide-depot.
- interferon-?, prolonged form of INF-? (PEG-interferon).
Chemotherapy:
- monochemotherapy: streptozocin, doxirubicin, fluorouracil, dactinomycin, etoposide, cisplatin, dacarbazine.
- PCT: combinations of streptozocin, fluorouracil and doxirubicin, cisplatin with etoposide.
Combination chemotherapy:
biotherapy + chemotherapy.
Symptomatic therapy:
- antihypertensive drugs
- antihistamines
- diuretics
- bronchodilators
- antidiarrheal drugs.
Mechanism of action of OCTREOTIDE-DEPO
- The drug has a symptomatic effect, reducing the secretion of hormones and peptides excreted in VIPomas in 89%, in glucoganomas in 75%, in insulinomas in 65%.
- After using Octreotide depot for various NETs, diarrhea stops in 40-60% of patients.
- With VIPomas, Octreotide-depot completely stops diarrhea in 38% of cases, and in another 38% of patients it significantly reduces it.
- Improves general condition in 75-85% of cases.
- Octreotide depot controls hypoglycemia in insulinomas and necrolytic skin lesions in glucanomas, which significantly improves the quality of life of patients.
For carcinoid tumors, the use of Octreotide Depot can lead to a decrease in the severity of symptoms of the disease, primarily such as hot flashes and diarrhea. In many cases, clinical improvement is accompanied by a decrease in plasma serotonin concentrations and urinary 5-hydroxyindoleacetic acid excretion.
For tumors characterized by overproduction of vasoactive intestinal peptide (VIP), the use of Octreotide Depot leads in most patients to a reduction in severe secretory diarrhea, which is characteristic of this condition, which, in turn, leads to an improvement in the patient’s quality of life. At the same time, there is a decrease in concomitant electrolyte imbalances, for example, hypokalemia, which makes it possible to cancel enteral and parenteral administration of fluids and electrolytes. According to computed tomography data, in some patients the progression of the tumor slows down or stops, and even reduces its size, especially metastases to the liver. Clinical improvement is usually accompanied by a decrease (down to normal values) in the plasma concentration of vasoactive intestinal peptide (VIP).
In case of glucagonomas, the use of Octreotide depot in most cases leads to a noticeable reduction in the necrotizing migratory rash that is characteristic of this condition. In patients suffering from diarrhea, Octreotide Depot causes its reduction, which is accompanied by an increase in body weight. When using Octreotide depot, a rapid decrease in plasma glucagon concentration is often observed, but with long-term treatment this effect does not persist. At the same time, symptomatic improvement remains stable for a long time.
For gastrinomas/Zollinger-Ellison syndrome, Octreotide depot, used as monotherapy or in combination with H2 receptor blockers and proton pump inhibitors, can reduce the formation of hydrochloric acid in the stomach and lead to clinical improvement, incl. and regarding diarrhea. It is also possible to reduce the severity of other symptoms, probably associated with the synthesis of peptides by the tumor, incl. tides In some cases, there is a decrease in plasma gastrin concentration.
In patients with insulinomas, Octreotide depot reduces the level of immunoreactive insulin in the blood. In patients with operable tumors, Octreotide depot can ensure the restoration and maintenance of normoglycemia in the preoperative period. In patients with inoperable benign and malignant tumors, glycemic control may improve without a simultaneous prolonged decrease in blood insulin levels.
In patients with rare tumors that overproduce growth hormone releasing factor (somatoliberinomas) , Octreotide Depot reduces the severity of symptoms of acromegaly. This appears to be due to suppression of the secretion of growth hormone releasing factor and growth hormone itself. In the future, it is possible to reduce the size of the pituitary gland, which was enlarged before treatment.
It was found that the use of Octreotide depot in doses of 30 mg and above has an antiproliferative effect associated with the direct cytotoxic effect of the drug on the tumor when interacting with somatostatin receptors, as well as with the inhibition of the formation of blood vessels feeding the tumor.
Dosage regimen
For endocrine tumors of the gastrointestinal tract and pancreas for patients in whom subcutaneous administration of Octreotide provides adequate control of the manifestations of the disease, the recommended initial dose of Octreotide depot is 20 mg every 4 weeks. Subcutaneous administration of Octreotide should be continued for another 2 weeks after the first administration of Octreotide depot. For patients who have not previously received subcutaneous Octreotide, it is recommended to begin treatment with subcutaneous administration of Octreotide at a dose of 0.1 mg 3 times a day. for a relatively short period of time (approximately 2 weeks) to assess its effectiveness and overall tolerability. Only after this is Octreotide depot prescribed according to the above scheme. In the case when therapy with Octreotide depot for 3 months. provides adequate control of clinical manifestations and biological markers of the disease, it is possible to reduce the dose of Octreotide depot to 10 mg, prescribed every 4 weeks. In cases where after 3 months. Treatment with Octreotide depot only achieved partial improvement; the dose of the drug can be increased to 30 mg every 4 weeks. During treatment with Octreotide Depot, on some days there may be an increase in clinical manifestations characteristic of endocrine tumors of the gastrointestinal tract and pancreas. In these cases, additional subcutaneous administration of Octreotide is recommended at the dose used before the start of treatment with Octreotide depot. This may occur mainly in the first 2 months. treatment.
Octreotide depot is a first-line drug for monotherapy or combination therapy of highly differentiated neuroendocrine tumors of the gastrointestinal tract and pancreas, effectively relieving hormonal syndromes by suppressing the hypersecretion of hormones by these tumors, increasing the quality of life and survival of patients.
Treatment of carcinoid tumor of the appendix in Germany
Treatment for carcinoid depends on several factors:
- its location;
- presence and extent of metastasis;
- general condition of the patient;
- stage of the disease.
The main directions of treatment for carcinoid tumor of the appendix are:
- Surgery – the most complete removal of a malignant tumor
- Radiation therapy
- Chemotherapy
- Targeted therapy
- Radioreceptor therapy
When metastases form, other forms of treatment are used, such as Octreotide or the radiopharmacone 131I-MIBG (meta-iodine-bencyl guanidine) to stop the growth of cancer cells, as well as embolization techniques.
INCIDENCE
- The incidence of neuroendocrine tumors of the gastrointestinal tract and pancreas is approximately 3-5 cases per 100,000 people per year.
- NETs of the gastrointestinal tract and pancreas can develop at any age, but more often after 50 years.
- When detected with glucagon, gastrin, VIP, and somatostatin, metastases to regional lymph nodes are detected in 60-80% of patients.
- The five-year survival rate for carcinoid cancer averages 50-67%. The best median survival rate occurs when the tumor is localized in the rectum (88%), bronchus (74%) and appendix (71%).
Clinical and pathogenetic characteristics of the main NETs
| Tumor type | Secreted hormones or amines | Clinical symptoms |
| Carcinoid | Serotonin | Carcinoid syndrome: hot flashes, diarrhea, bronchospasm, hypertension, heart damage. |
| Gastrinoma | Gastrin | Zollinger-Ellison syndrome, severe peptic ulcers |
| VIPoma | Vasointestinal polypeptide | Severe diarrhea (“pancreatic cholera”, Werner-Morrison syndrome) |
| Insulinoma | Insulin | Hypoglycemia |
| Glucagonoma | Glucagon | Diabetes, erythema migrans, irritation and redness of the tongue |
| Somatostatinoma | Somatostatin | Gallbladder dysfunction, cholelithiasis, impaired glucose tolerance |
CARCINOID
One of the most common tumors of the diffuse neuroendocrine system! The tumor secretes:
- serotonin
- bradykinin
- 5-hydroxytryptophan
- prostaglandins
- VIP
- histamine
This leads to the development of carcinoid syndrome.
CARCINOID SYNDROME
Manifestations:
- hot flashes (63-94%). Sudden appearance of deep red or purple erythema of the upper torso, mainly the face and neck. Accompanied by an unpleasant sensation of warmth, lacrimation, itching, swelling of the face and conjunctivitis, salivation and sweating, a feeling of pulsation.
- diarrhea (68-84%)
- bronchospasm (3-19%)
- shortness of breath (3-19%)
- telangiectasia (25%)
- heart changes (11-53%)
- pellagra-like syndrome with hyperkeratosis and pigmentation (2-6%)
- heart damage - carcinoid cardiac syndrome (Hedinger syndrome) is detected in more than 50% of patients.
The syndrome is caused by the development of fibrous changes in the endo- and myocardium of the right heart with damage to the valves. Stenosis and insufficiency of the tricuspid valve and pulmonary valve are characteristic.
CARCINOID CRISIS
- It can occur spontaneously or be provoked by stress, alcohol, certain foods (for example, cheese), and injections of catecholamines.
- Initial attacks last 2-5 minutes, and later their duration can increase to several hours.
- Crises more often occur with daily excretion of 5-HIAA more than 200 mg and are provoked by stress, anesthesia, biopsy or surgery, chemotherapy, causing high mortality.
CLASSIFICATION OF NEO (WHO, 2002)
- Well-differentiated neuroendocrine tumor (benign).
- Well-differentiated neuroendocrine carcinoma (low-grade).
- Poorly differentiated neuroendocrine carcinoma (small cell).
- Mixed exocrine and endocrine carcinoma.
- Tumor-like lesion.
Characteristics of highly differentiated NETs
- low proliferative potential
- ability to secrete various biological substances
- low sensitivity to chemotherapy.
These include various carcinoids of the foregut, midgut and hindgut, pheochromocytoma, and medullary thyroid cancer.
Characteristics of low-grade NETs
- highly malignant tumors with high proliferative potential
- sensitive to chemotherapy and radiation therapy.
These include small cell cancer of the lung and other organs.
Characteristics of mixed exocrine and endocrine carcinomas
- these include various pancreatic tumors (except carcinoids)
- The sensitivity to chemotherapy of these tumors is moderate.
CLASSIFICATION OF CARCINOID TUMORS (WILLIAMS AND SANDLER, 1963)
- Upper (2-9%) (foregut): tumors of the respiratory tract, thymus, esophagus, stomach, duodenum, pancreas. Characterized by low secretion of serotonin, increased secretion of histamine and various hormones, an atypical course of carcinoid syndrome, frequent metastasis to the bones.
- Middle (75-87%) (midgut): tumors of the small intestine, appendix, cecum, ascending colon. Hypersecretion of serotonin and other vasoactive substances, carcinoid syndrome.
- Lower (1-8%) (hindgut): tumors of the transverse colon and descending colon, sigmoid and rectum. Carcinoid syndrome is not typical; liver metastasis is common.
Classification depending on the presence or absence of carcinoid syndrome
- Hormonally active tumors are characterized by hypersecretion of hormones. Clinical symptoms allow early diagnosis.
- Hormonally inactive tumors (no symptoms of hormone hypersecretion) – up to 50% of neuroendocrine tumors. Clinically manifested with a large tumor mass - at this stage the tumor metastasizes, and can also manifest itself as symptoms of intestinal compression.
LABORATORY DIAGNOSTICS
- Determination of the level of serotonin and its metabolites in urine. The most common test is to measure the excretion of 5-HIAA (5-hydroxyindoleacetic acid) in 24-hour urine. However, this analysis may give false positive results depending on the nature of the food consumed by patients (citrus fruits, bananas, pineapples, kiwi, nuts).
- Determination of the level of chromogranin A in the blood (an increase in the level of chromogranin A is observed in 87-99% of patients), the norm is less than 4.5 mmol/l. This plasma marker is the most reliable for NET.
- Determination of the level of excretion of neuron-specific enolase in the blood.
Where is the best place to treat appendix carcinoid?
Carcinoid tumor of the appendix belongs to neuroendocrine tumors, the treatment of which involves the interaction of doctors from different fields: surgeons, endocrinologists, radiologists, oncologists, which is successfully provided at the Nordwest Clinic. The treatment regimen for neuroendocrine tumors directly depends on their type and stage of development, and therefore accurate diagnosis of the disease is of particular importance. The diagnostic equipment of the Nordwest Clinic provides the most modern capabilities for determining and confirming all types and stages of cancer. When you contact us, you can be sure that the therapy will be tailored individually, taking into account the characteristics of the development of the disease.