Why does the infringement occur?
The causes of strangulated hernia are associated with a sharp or persistent increase in intra-abdominal pressure. This condition develops under the influence of external or internal factors:
- excessive physical activity;
- lifting heavy loads;
- chronic constipation;
- hacking cough;
- intestinal atony;
- weakened abdominal wall muscles;
- abdominal injuries;
- sudden weight loss;
- abdominal surgeries.
Internal organs caught in the hernial orifice are unable to correct themselves. Due to the overly stimulated tone of the muscles that form the hernial orifice, their size decreases, the organs become pinched, and signs of strangulation of the hernia appear.
With a hernia of the Spigelian line and other elastic strangulations, necrosis develops in the strangulated tissues within a few hours, and the risks of peritonitis and intestinal obstruction increase.
Complications
The presence of a hernia in a person significantly reduces the quality of life and ability to work. However, the need to eliminate a hernia is, first of all, dictated by the risk of possible complications.
The most dangerous complication is strangulated hernia.
In this case, any organ of the abdominal cavity (most often intestinal loops) gets into the hernial sac, which cannot be set back. The blood supply to the strangulated organ is disrupted and it begins to die (dead).
Symptoms of a strangulated hernia: the occurrence of sharp pain, tension of the hernial protrusion, which ceases to be reduced, later this is accompanied by nausea, repeated vomiting, retention of stool and gases. A strangulated hernia is a serious complication and is an indication for emergency surgery. Then we are talking about saving the patient’s life, and not about performing abdominal wall plastic surgery. The mortality rate from strangulated hernia is very high and ranges from 4.3% to 10%. Over the past 50 years, this indicator has not improved. Only timely planned repair of a hernia can prevent the development of complications.
Types of pathology
According to pathogenesis in surgery, the following types of strangulated hernias :
- elastic – associated with persistent spasm of the muscles of the anterior abdominal wall;
- fecal - develops as a result of a sharp overflow of the adductor part of the intestine located in the hernial sac.
Depending on which organ is pinched in the hernial orifice, there are pathologies with: pinching of the mesentery, parts of the intestine, omentum or stomach. With an inguinal hernia, the bladder, uterine appendages (in women), and spermatic cords (in men) may be compressed.
Special types of infringement include:
- Retrograde - at least three intestinal loops enter the hernial sac, two of which are in good condition, and necrosis develops in the third.
- Parietal - partial compression of the intestine in the area opposite the mesenteric edge.
Primary infringement is most often provoked by a single spasm of the abdominal wall muscles. Secondary develops as a complication of a previously diagnosed hernial formation.
Umbilical hernia in adults - symptoms and treatment
Treatment of umbilical hernia in adults is only surgical. Even an uncomplicated hernia is an indication for surgery [9]. It is impossible to cure a hernia with bandages; as a rule, they are used after surgery as part of rehabilitation.
Goals of surgical treatment:
- Return the contents of the hernial sac to the abdominal cavity or remove it if the areas of the strangulated organs are no longer viable.
- Restore the integrity of the abdominal wall in the area of the hernia defect, including using mesh prostheses. Such prostheses help to further strengthen the abdominal wall in the scar area. Connective tissue cells grow into the cells of the mesh and due to this, a dense scar “shell” is formed in the scar area, which prevents recurrence of the hernia.
The operation can be performed either open or laparoscopic. Both methods are equally effective, but after laparoscopy the pain syndrome is less pronounced and the patient’s rehabilitation is faster [1][9].
For small hernial protrusions (up to 1–2 cm), open surgery is often performed with local anesthesia. The surgeon makes an incision in the projection of the umbilical ring, places the organs and tissues from the hernial sac into the abdominal cavity and sutures the tissue to restore the integrity of the abdominal wall. Additionally, the weak area is strengthened with a mesh endoprosthesis. The mesh implant can be located preperitoneally (above the peritoneum), retromuscularly (behind the rectus abdominis muscles), supraponeurotically (between the aponeurosis and subcutaneous fatty tissue), or otherwise. The installation location depends on the technique. With open surgery with local anesthesia, the rehabilitation period is 1–2 weeks.
Laparoscopic surgery is considered a minimally invasive surgical procedure. It is performed using a video camera and special tools. The surgeon sees the surgical field on the monitor and controls all his actions during the operation. With laparoscopy, the period of hospital stay is reduced to 2–3 days.
For large hernias, most often only open surgery under endotracheal (general) anesthesia is possible. The surgeon makes a long incision in the abdomen, isolates the hernial sac, places the organs and tissues from the hernial sac into the abdominal cavity, removes the excess walls of the hernial sac and then sutures the tissues. If the hernial orifice is more than 2 cm, a mesh prosthesis is always installed. After such an operation, the patient remains in the department from 1–2 days to a week.
When operating on a strangulated hernia, the surgeon first carefully examines the contents of the hernial sac and determines its viability. If the contents of a strangulated hernia are reduced into the abdominal cavity before the doctor makes an incision, then it is necessary to examine the contents of the abdomen, find the strangulated organs and assess their condition. If the intestinal wall becomes necrotic or perforated (ruptured), the affected part of the organ is removed. After this, the surgeon sutures the hernial orifice. A mesh implant is not placed due to the high risk of wound suppuration and mesh rejection. It can be installed later, when the inflammation subsides or the hernia appears again.
When the contents of the hernia are suppurated (phlegmon of the hernial sac), an incision in the abdomen is usually made not above the hernia, but a little further. After this, the contents of the sac are isolated: the strangulated intestine is excised, the area of the hernial orifice is sutured from the side of the abdominal wall. At the next stage, the surgeon removes the hernial sac with its contents or opens the hernia and washes the cavity of pus and dead tissue. A mesh implant is not installed for this complication. It can be installed later, when the inflammation subsides or the hernia appears again.
If the strangulated hernia has repaired itself before the patient is taken to the operating room, it is necessary to monitor the patient for 24 hours to make sure that there is no necrosis of the strangulated organs and peritonitis. If the patient feels well and there are no signs of peritonitis, it is recommended to undergo elective surgery to remove the hernia.
Rehabilitation after hernia removal
In order for the patient to recover after surgery as quickly as possible, it is recommended that he:
- do not lift weights exceeding 5 kg in the first 5–6 weeks after surgery;
- gradually increase physical activity: 14 days after surgery, swimming, light jogging, walking, Nordic walking, cardio training without straining are allowed;
- treat concomitant diseases, especially diabetes mellitus and chronic obstructive pulmonary disease;
- wear a postoperative bandage for two months;
- control weight.
Possible complications of operations
Complications can arise with any operation on the abdominal organs; this is due to the technique of execution [1][9]. Such complications include:
- Injury to the intestinal wall during surgery. If such a complication occurs, the intestinal defect must be immediately sutured.
- Bleeding in the postoperative period with the development of a hematoma of the surgical wound or inside the abdomen. It may be associated not only with a violation of the surgical technique, but also with a violation of the patient’s coagulation system, for example, with hemophilia. This complication does not always require a second operation: if there are no signs of ongoing bleeding (increasing hematoma, increasing pallor and general weakness, bleeding from the wound), you can evacuate the hematoma or perform a puncture of the abdominal cavity. If bleeding continues, the blood vessel is sutured or cauterized.
- Seroma of a postoperative wound. This is an accumulation of serous fluid at the site of the removed hernial sac. It manifests itself as swelling and compaction in the wound area. If a seroma develops, the surgeon evacuates the fluid in the dressing room; repeated surgery is not required.
- Suppuration of a postoperative wound. It manifests itself as redness in the wound area, throbbing pain in the wound, as well as an increase in body temperature. If suppuration occurs, it is necessary to remove pus from the wound and prescribe antibiotic therapy. It is often necessary to remove the mesh implant.
- Chronic pain syndrome . It manifests itself in the fact that the patient has been bothered by pain in the area of the postoperative wound for a long time (more than two months). The cause of the complication is damage to the nerve structures during surgery. Chronic pain syndrome requires an integrated approach. Sometimes it is necessary to perform a second operation to free the nerve from the compressing tissue or remove the mesh implant [6].
- Displacement of the mesh implant. The endoprosthesis may move if the mesh fixing material (suture material or clips of various modifications) comes off. In this case, the implant moves to the lower corner of the wound and folds, which often leads to recurrence of the hernia and the need for repeated surgery.
- Recurrence of hernia. It occurs for various reasons: due to the characteristics of the patient’s connective tissue, suppuration of the implant, wound healing by secondary intention, or violation of the surgical technique. In case of relapse, the hernia is removed using a different method, i.e. if a relapse occurs after open surgical treatment, then it is recommended to perform a repeat operation using the laparoscopic method and vice versa.
Treatment of umbilical hernia in pregnant women
There are no generally accepted clinical recommendations for the treatment of hernias in pregnant women, but three key points can be identified:
- strangulated hernias in pregnant women require emergency surgical treatment;
- asymptomatic hernias up to 3 cm are recommended to be operated on after childbirth or in the second trimester of pregnancy;
- preference is given to the laparoscopic method, but the decision on the volume of intervention should be made with the participation of an experienced obstetrician-gynecologist [14].
Strangulated hernia: symptoms of the disease
❗ What signs can be used to judge a developing pathology:
- sharp pain at the location of the hernial formation;
- muscle tension in the protrusion area;
- inability to straighten a pinched organ;
- absence of cough impulse transmission.
The clinic of a strangulated hernia is characterized by a general deterioration in the patient’s well-being. The skin becomes pale, the heartbeat quickens, and vomiting occurs. With the development of intestinal obstruction, vomiting becomes fecal in nature and becomes constant.
With prolonged strangulation, signs of painful shock appear - decreased blood pressure and tachycardia. At the site of the hernial protrusion, phlegmon forms - a purulent inflammatory process without clear boundaries of the lesion. If a strangulated umbilical hernia or other protrusion is not eliminated in time, the outcome is diffuse peritonitis.
Strangulated inguinal hernia
Dear Konstantin Viktorovich! I would like to express my immense gratitude to you and the entire team of the Swiss University Clinic for returning me to normal life - without pain, without anxiety and fear, with full confidence that now everything will be GOOD!
It so happened that I received treatment at this clinic twice. Over the past six months, I have consulted several gastroenterologists. But it didn’t get any easier: the pain somewhere in the stomach area intensified, no medications or diets helped. Finally, a diagnosis was made - cholelithiasis. They suggested trying to dissolve the stones using medications (ursosan). They warned me that I would have to drink them for a long time, several months. For almost three months, I went to the pharmacy more often than to the store for bread: a lot of medications were prescribed, I had to take handfuls of pills! But instead of relief, a severe pain attack began. The pain made it dark in my eyes, and I was ready for surgery, and for anything - if only someone would help!
Using the Internet, the sons found information about Professor K.V. Puchkov. as the best specialist in this field and immediately contacted his clinic. And despite the huge busyness that day: operations and consultations were planned, he did not refuse to see me (for which special thanks to him!). From just communicating with him, from his calm confidence, the panic immediately decreased, and I realized that this person would definitely help me. A short time later, after all the necessary examinations, I was already lying under IVs in a comfortable room under constant supervision by very attentive and sensitive doctors and nurses. As Konstantin Viktorovich explained, I had acute cholecystopancreatitis (against the background of cholelithiasis, the pancreas also became inflamed). It was impossible to operate at this moment. Three days later I was discharged home without pain for further rehabilitation.
And so on June 18, 2014, after a preliminary consultation with Konstantin Viktorovich, I underwent 2 operations at once (during the examination, an umbilical hernia was also discovered). For some reason I was very afraid of anesthesia. But anesthesiologist Ruslan Avelievich Vinogradov calculated everything in such a way that I didn’t even feel it! After the operation I came to my senses very quickly, there was no nausea, etc. There are only 4 punctures in the abdomen (the hernia was removed through a puncture in the navel, a mesh implant was inserted). I didn't expect everything to go so easily! When Konstantin Viktorovich arrived, I was already reading a book. ))) On the 3rd day I was discharged. It's only been 8 days and recovery is going very quickly.
In conclusion, I would like to once again thank Konstantin Viktorovich for everything. In addition to the fact that he has golden hands, he also has a big heart, the warmth and kindness of which is enough for all his patients without exception. Konstantin Viktorovich, I wish you health, strength, new successes and discoveries! Prosperity to your clinic, you have a wonderful professional team, excellent conditions. I will recommend you to my loved ones with full confidence in a successful outcome.
Diagnosis: Gallstone disease. Chronic calculous cholecystitis. Irreversible umbilical hernia. Operation performed: Laparoscopy, cholecystectomy. Umbilical allohernioplasty.
Larisa Drozhzhina [email protected]
Diagnostic measures
✅ Diagnosing a hernia infringement is not difficult. In most cases, an external examination is sufficient, during which you can detect a painful protrusion in the groin area or on the anterior abdominal wall. A clear sign of the disease is the absence of a cough impulse and symptoms of intestinal obstruction.
, abdominal ultrasound and radiographic examination are prescribed for differential diagnosis .
Hernia symptoms
- the presence of a protrusion in the groin or umbilical region, along the midline of the abdomen or in the area of a postoperative scar, which patients can independently detect (in the lying position the protrusion may completely disappear);
- nagging pain in the lower abdomen, in the navel area of varying intensity, especially during physical activity;
- abdominal pain, bloating, constipation associated with the presence of adhesions inside the hernial sac in large postoperative hernias.
How is a strangulated hernia treated?
⚠ Therapeutic tactics for strangulated hernia consist of emergency surgical intervention.
During the operation, the surgeon releases the compressed organs and examines the extent of their damage. If necrotic areas are found in the intestines, they must be removed immediately. The hernial opening is closed with special synthetic materials or the patient’s own tissues.
In case of a strangulated hernia of the white line of the abdomen and other parts of the abdominal wall, it is prohibited:
- adjust the protrusion independently;
- take laxatives;
- administer antispasmodics and analgesics.
Treatment of hernia of the anterior abdominal wall
The only treatment method is surgical. The operation is aimed at eliminating the hernia and closing the “weak” spot in the abdominal wall - hernioplasty
.
Two methods of surgical intervention are used:
- the traditional “open” method (an incision above the hernia), in which the defect is closed with its own tissues or a special mesh, the so-called “tension-free” type of plastic surgery.
- laparoscopic method - closing the defect with a special mesh through small incisions in the abdominal wall.
Treatment of strangulated hernia in our clinic
Specialists at the herniology center in Kaliningrad are ready to provide routine care to patients with hernias of the anterior abdominal wall. Emergency operations in case of strangulation are carried out in emergency hospitals in the city.
☝ We recommend that you seek routine help in a timely manner and not wait for serious complications such as strangulated hernias. In this case, the risks of complications will be minimal, and surgeons will do everything possible to get you back to your normal life as quickly as possible.
To find out the details of hernia treatment at the clinic for reconstructive surgery of the anterior abdominal wall, sign up for a consultation by phone: ☎ +7 (4012) 971-961.
Diagnosis of hernias
The diagnosis in most cases can be made based on a simple examination of the patient, when a protrusion is detected in typical places, increasing with physical activity. In unclear cases, the surgeon may use additional research methods.
- Ultrasound of a hernia allows you to determine the size of the hernial orifice, distinguish small irreducible hernias from soft tissue benign tumors of the subcutaneous fatty tissue (for example, lipomas), and enlarged lymph nodes of the groin area. It is especially useful for inguinal hernias.
- Herniography is used in case of unclear pain in the groin area (to exclude an externally invisible inguinal or femoral hernia), perineum (to exclude a perineal hernia) and in case of an inguinal hernia, if there is doubt about the presence of a hernia on the opposite side.
- Computed tomography allows you to clearly determine the nature and size of the abdominal wall defect.
In recent years, due to the widespread introduction of new technologies and the latest scientific achievements and the use of modern plastic and suture materials, the quality of hernia repairs has significantly improved, and the number of relapses and postoperative complications has decreased.
An umbilical hernia is a pathological protrusion of abdominal organs through the umbilical ring, which can disappear or significantly decrease in size when the body is horizontal. This disease affects 6–10% of the population in adults and is more common in women.
Symptoms
The severity of symptoms of an umbilical hernia depends on many factors:
- its size;
- the presence of adhesions in the abdominal cavity;
- the presence or absence of strangulation of the hernial sac;
- general condition of the patient.
The very first symptom of a hernia is the appearance of a small protrusion in the navel area. There may not be any pain at first. At an early stage, you can even repair the hernia yourself, without a doctor. If adhesions appear, it will no longer be possible to straighten it. The duration of the process of adhesions formation varies from person to person, so some people have been accustomed for years to repair a hernia and move on without seeing a doctor, while for others, adhesions appear quite quickly.
Pain is not always present with an umbilical hernia in adults. It can appear during physical activity, coughing and standing in one place for a long time. Late stages may already be accompanied by nausea, vomiting, belching, constipation and difficulty urinating.
Treatment
The only treatment for umbilical hernia in adults is surgery. Surgery for an umbilical hernia may be postponed in uncomplicated forms of the disease in pregnant women or in cases of concomitant diseases aggravating the general condition of the patient (acute or aggravated chronic diseases, pulmonary or heart failure, etc.).
Causes of acute pain with a hernia in the lumbar region
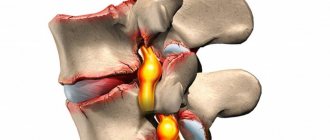
First of all: an intervertebral disc that has lost its shape is not a source of pain. The disc may even rupture entirely. Its outer, circular fibrous layers cease to hold the internal nucleus pulposus, which is under high pressure, and the contents of the disc fall out of its limits. This is how a hernia is formed from the protrusion. But the disc itself, just like any cartilage tissue in the body, is not capable of feeling pain. The cartilage formations are not innervated, since otherwise the nerves would have to be in constant motion, with the risk of getting caught between the discs. For the same reason, cartilage, as the boundaries of the skeleton, which has mobility, is also devoid of blood vessels.
Therefore, the source of pain is other structures:
- the first of them is the deep ligaments, which are constantly touched by the hernial protrusion;
- the second component is the nerve roots that enter and exit the spinal cord at the level of each segment, which have sensory and motor portions.
The nerve roots themselves also cannot perceive pain. But if they experience intense compression by a protrusion, or, especially, a hernia, this will lead to the development of aseptic inflammation.
This inflammation will be of the same nature as a callus on the heel, which has formed as a result of constant rubbing from shoes. Constant mechanical irritation of the nerve roots leads to edema, swelling, they begin to be compressed by the surrounding bone canals and ligaments, and the pain increases sharply with every movement and shock (especially with intraforaminal hernias) of such a swollen nerve root. That is why the pain is shooting and sharp;
- this pain also has a constant, aching component, which is largely due to the reaction of the surrounding muscles.
A muscle can respond to pain in only one known way. This is a reduction. If the pain is constant, then the muscle is in a state of constant spasm, and excessive contraction makes it impossible for blood to flow and remove harmful substances from the muscle that are formed as a result of its vital activity. First of all, it is lactic acid.
Therefore, in the presence of an irritating factor, such as a protrusion or hernia, the muscle becomes denser and gradually falls into a state of constant, chronic spasm. Pain stimulates contraction, and constant contraction increases this pain. A vicious circle is formed.
Thus, in the pathogenesis of acute pain in the lower back with protrusion or hernia, several components can be distinguished: ligaments, swelling of the roots and muscle reaction, which forms aching pain that persists for a long time. How can we cope with this complex and multifaceted pain?
What does a hernia consist of?
All hernias, regardless of location and size, have a common structure and consist of the following components:
- A hernial orifice is a defect of the anterior abdominal wall, mainly in the aponeurosis. Through them, the internal organs leave the abdomen and end up under the skin. If the hernial orifice is wide, then through it the contents can freely return to the abdominal cavity.
- Hernial sac is a sheet of stretched peritoneum covering organs that extend beyond the abdominal cavity through the hernial orifice. The hernial sac is covered with several membranes, these also include subcutaneous tissue and skin.
- The contents of the hernial sac are the internal organs or their individual parts that extend beyond the abdominal cavity through the hernial orifice.
Examination methods for diagnosis
Diagnosing an inguinal hernia is not difficult. By collecting a detailed history of the disease and life, and an objective examination, a preliminary diagnosis is made.
To clarify, additional examination methods .
- Laboratory tests (general analysis and blood biochemistry, liver tests, coagulogram, general urinalysis) - prescribed to identify the degree of severity, in preoperative preparation to assess possible risks during surgery;
- Ultrasound of the abdominal organs, pelvis, inguinal canal, scrotum - allows you to visualize the contents of the hernial sac, differentiate an inguinal hernia from other diseases, clarify the type, assess the condition of the inguinal canal and the organs involved;
- Herniography - an X-ray examination with contrast is performed for an internal inguinal hernia, when there are complaints of pain in the groin area, but there is no obvious protrusion;
- Irrigoscopy – X-ray contrast examination of the colon to determine its location;
- Cystography is an X-ray examination of the bladder with the introduction of a contrast agent, prescribed for suspected sliding inguinal hernia involving the urinary system;
- Computed tomography - allows you to accurately localize the hernial orifice, determine the contents of the hernial sac, and is performed in doubtful cases to verify the diagnosis.
The doctor who has diagnosed an inguinal hernia will tell you what to do next and select safe treatment with minimal risk of relapse, taking into account individual characteristics.
Effective Treatments
Easily reducible hernia contents give the false belief that the inguinal hernia has resolved on its own.
There are no conservative treatment options . An elastic bandage prevents strangulation, slows down the rate of progression of an inguinal hernia, surgical treatment completely neutralizes the pathological process, and reduces the risk of relapse to a minimum.
Incarceration with signs of an “acute” abdomen is a direct indication for emergency surgical care. The operation is performed as quickly as possible with minimal examination and preoperative preparation. Planned treatment of an inguinal hernia, the symptoms of which do not cause concern for the patient’s life, is carried out after a full examination.
Hernioplasty is performed using open access and laparoscopic methods .
The operation using the Lichtenstein method is a classic version of open repair, the “gold ” standard , which is effective for hernias of any size and location. Does not require general anesthesia. The protrusion is reduced without opening the hernial sac, after which a special mesh is installed to strengthen the structures of the inguinal canal. With this treatment, the risk of relapse is less than 1%. But in the first days after the operation, pain may be expressed; in the long term, chronic abdominal pain is sometimes bothersome.
A less invasive way to eliminate an inguinal hernia are laparoscopic techniques: transabdominal preperitoneal repair (TAPP), total extraperitoneal repair (TEP).
Access is made through three small punctures in the abdominal wall, which ensures quick recovery and minimal cosmetic defects. The operation is performed under general anesthesia using an endoscopic unit. An ideal correction option for a bilateral process. The intensity of pain after surgery is significantly lower.