Published: 10/22/2021 15:15:00 Updated: 10/25/2021
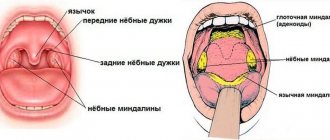
Sore throat is a disease of an infectious nature, manifested by acute inflammation of the lymphoid tissue of the pharynx. Most often the process affects the palatine tonsils, but other structures of the lymphadenoid pharyngeal ring can also be affected - the lingual and pharyngeal tonsils, lateral ridges or granules of the posterior pharyngeal wall.
The pathology in question is characterized by symptoms of intoxication, increased general temperature, sore throat that worsens during swallowing, enlarged and painful cervical lymph nodes. The palatine tonsils and arches are swollen, enlarged, bright red, and may have a white or dirty yellow coating.
Treatment of sore throat includes local treatment with antiseptics, painkillers and anti-inflammatory drugs, antibiotic therapy and detoxification measures. If complications develop or the process becomes chronic, surgical intervention may be required.
Causes of sore throat
Most often, inflammation is caused by the activity of beta-hemolytic streptococcus group A. Among the possible causative agents of the disease are also adenovirus, staphylococci, pneumococci, parainfluenza virus, mycoplasma, chlamydia, rhinovirus, respiratory syncytial virus, spirochete, Epstein-Barr virus, diphtheria bacillus, enterovirus Coxsackie B, fungi.
The risk of developing a sore throat increases when exposed to the following factors:
- general or local hypothermia;
- weakened immunity due to acute respiratory infections;
- fungal diseases;
- chronic pathologies of the nasopharynx, difficulty in nasal breathing, purulent processes and inflammation in the paranasal sinuses;
- caries;
- systematic exposure to irritating substances on the body, work in a smoky or dusty room;
- increased air dryness;
- regular drinking of alcohol, smoking;
- acute and chronic intoxication;
- poor nutrition, lack of vitamins in the diet.
Prevention measures
Is strep throat contagious to others? Yes, with tonsillitis the main route of transmission of infection is airborne. Infection occurs from a sick person or a carrier of pathogenic bacteria. Therefore, to prevent infection, it is necessary:
- reduce contact with a sick person to a minimum;
- use personal utensils (a person with a sore throat is given a separate cup, plate, fork and spoon).
Prevention measures also include general principles of addressing risk factors:
- promptly treat acute respiratory infections, the first sign of which is a runny nose;
- visit the dentist regularly to detect and treat caries in a timely manner;
- give up passive and active smoking.
Types and symptoms of sore throat
Depending on the cause, angina may be primary if the site of inflammation is initially localized in the tonsils.
A secondary or symptomatic type of pathology is considered a manifestation of another disease - infectious mononucleosis, diphtheria, scarlet fever, tularemia, typhoid fever, leukemia, alimentary-toxic aleukia, agranulocytosis. Inflammatory damage to the palatine tonsils is called tonsillitis, and to the nasopharyngeal tonsils - adenoiditis. There is also tonsillitis of the lingual tonsil, lateral ridges of the pharynx and laryngeal tonsillitis.
Based on the depth and nature of inflammation of the lymphoid tissue, the following forms of the disease are distinguished:
- catarrhal;
- lacunar;
- follicular;
- ulcerative-membranous;
- necrotic;
- combined.
Characteristic manifestations of any form of angina are general symptoms of intoxication, including increased body temperature, weakness, decreased appetite, headache, as well as enlarged and painful regional lymph nodes.
The incubation period depends on the type of pathogen and the state of immunity, ranging from several hours to a week or more. Other signs of angina, such as sore throat and external changes in the tonsils, may have varying severity depending on the form of the disease.
Catarrhal
The inflammatory process primarily involves the mucous membrane of the tonsils.
The disease begins acutely. The temperature during catarrhal tonsillitis rises within 37.1-38.0 °C, symptoms of intoxication and sore throat during swallowing are moderate. Characterized by enlargement of the lymph nodes located in front of the sternocleidomastoid muscle at the level of the angle of the lower jaw. The palatine tonsils are moderately swollen, their mucosa, as well as the surface of the palatine arches and the soft palate, are brightly hyperemic. The duration of the disease is 2-3 days, after which recovery occurs or a transition to a more severe form occurs.
Viral sore throat occurs with symptoms of ARVI - runny nose, cough. When infected with Coxsackie enterovirus, blistering rashes are observed on the mucous membrane of the palate and tonsils.
Lacunar and follicular
The clinical course of both lacunar and purulent tonsillitis is severe.
Characterized by fever from 38.0 to 40.0 °C, severe intoxication syndrome: headache, general weakness, aches in joints and muscles, pain in the projection of the heart, chills, sleep and appetite disturbances. The pain in the throat during swallowing is sharp, often radiating to the ear. Severe inflammatory changes lead to dysphonia - the voice takes on a nasal tone. Swelling of the tonsils may be accompanied by difficulty breathing and temporary hearing loss. When a child has a sore throat, there may be increased salivation, drowsiness, vomiting, convulsions, and abnormal bowel movements. In the first 2-4 days, the symptoms increase rapidly, and then disappear just as quickly. In the lacunar form of the disease, in addition to swelling and pronounced redness of the mucous membrane, white, irregularly shaped overlays with a yellowish tint appear on the tonsils, which can be easily removed with tweezers. In the case of follicular tonsillitis, suppuration of the follicles occurs; individual pinpoint yellowish formations of regular shape, no larger than a pinhead, appear through the epithelium. The tongue is dry, covered with a white coating. On the 4-5th day, the surface of the lacuna begins to clear, and the purulent blisters gradually disappear.
Necrotic
The most severe form of the disease. A pronounced intoxication syndrome is characterized by persistent fever, impaired consciousness, and repeated vomiting that does not bring relief. Dirty yellow spots with a greenish tint, ulcers and ulcers appear on the surface of the tonsils.
Ulcerative-membranous
Simanovsky-Plaut-Vincent angina is caused by a spirochete and a spindle-shaped rod that constantly live in the oral cavity.
With exhaustion, a pronounced decrease in immunity or hypovitaminosis, opportunistic microorganisms can become active, causing inflammation. The difference between ulcerative membranous tonsillitis and other forms is the one-sidedness of the process. An ulcer with a gray-yellow coating on the surface appears on the tonsil mucosa. Characterized by a putrid odor from the mouth, moderate sore throat and enlarged regional lymph nodes on the same side as the inflammation. Symptoms of intoxication may be absent or mild. The duration of the disease is from 7 to 12 days. After cleansing of plaque, the ulcerative defect heals without scar formation. Extensive ulcerations can lead to bleeding, damage to the periosteum, and perforation of the palate.
Stages of disease development
The disease progresses rapidly. This is especially true in children and adults with a weakened immune response. Symptoms depend on the current state of the body, age, concomitant diseases and the stage of infectious tissue damage.
Signs of the development of the disease at different stages from the moment of infection:
- 2-3 days.
This stage is characterized by the maximum severity of the symptomatic picture. The patient's tonsils increase significantly in size and white or yellowish ulcers appear on their surface. The inflammatory process covers the entire surface of the tonsils. The patient notes deterioration in health, weakness, loss of appetite and signs of fever, including an increase in body temperature to 39-40 ° C. The patient also experiences excruciating pain in the throat, which gets worse when swallowing. - Day 4
The ulcers that form on the tonsils begin to spontaneously open, releasing the contents (pus). In their place, lacunae are formed - characteristic depressions. If at this stage the patient follows the doctor’s recommendations, the lacunae quickly close. - 5-6 day
. At this stage, patients feel a noticeable improvement in their condition - body temperature normalizes, headaches go away, strength and appetite are restored. - 7-10 day
. The last pathological sign – sore throat – recedes. The size of the lymph nodes located under the lower jaw also decreases. The patient ceases to feel pain and discomfort in this area.
Competent and timely therapy allows you to avoid serious complications.
Complications of sore throat
During the disease, the infection can spread to neighboring organs, causing otitis media, lymphadenitis, sinusitis, and peritonsillitis. Among the local purulent complications of tonsillitis, one can note the formation of an abscess or phlegmon in the inflamed tissues. Their occurrence is accompanied by a new wave of fever, increasing sore throat, problems with swallowing and breathing. In the case where the pathology is caused by streptococcus, 3-4 weeks after clinical recovery, glomerulonephritis, reactive arthritis or rheumatic carditis may develop due to subsequent autoimmune processes.
Sources
- Gauvin CA., Klyachman L., Grewal PK., Germana SS., Singh A., Rashba EJ. Electrical Storm in a Case of Bilateral Pheochromocytomas. // Am J Case Rep - 2021 - Vol22 - NNULL - p.e929507; PMID:33764957
- Behaeghe O., Geurde B., Jourdan JL., Bodson C., Seydel B., Lacremans D. A case of a borderline adrenal oncocytoma in a 62-year old female. // Acta Chir Belg - 2021 - Vol - NNULL - p.1-4; PMID:33554753
- Diatroptov ME., Diatroptova MA., Kosyreva AM. Effect of Surgical Removal of Testicles and Adrenal Glands on Ultradian Rhythms of Body Temperature in Male Wistar Rats under Conditions of Constant Illumination. // Bull Exp Biol Med - 2021 - Vol169 - N5 - p.691-694; PMID:32986204
- Samsel R., Cichocki A., Roszkowska-Purska K., Papierska L., Koalasińska-Ćwikła A., Karpeta E., Ostrowski T., Nowak K. Adrenal metastases — long-term results of surgical treatment, single-centre experience . // Contemp Oncol (Pozn) - 2021 - Vol24 - N1 - p.29-33; PMID:32514235
- Tanaka T., Aoyagi C., Mukai K., Nishimoto K., Kodama S., Yanase T. Extension of Survival in Bilaterally Adrenalectomized Mice by Implantation of SF-1/Ad4BP-Induced Steroidogenic Cells. // Endocrinology - 2021 - Vol161 - N3 - p.; PMID:31950150
- Hueston CM., Deak T. Corticosterone and progesterone differentially regulate HPA axis and neuroimmune responses to stress in male rats. // Stress - 2021 - Vol23 - N4 - p.368-385; PMID:31591928
- Dzalilova DS., Diatroptova MA., Mkhitarov VA., Diatroptov ME. Infradian Rhythms of Resistance to a Dissociative Anesthetic in Wistar Male Rats under Normal Conditions and After Surgical Removal of the Adrenal Glands and Testes. // Bull Exp Biol Med - 2021 - Vol166 - N3 - p.413-416; PMID:30617706
- Dworzyńska A., Paduszyńska K., Pomorski L. Autogenous transplants of adrenal fragments in an animal model. // Pol Przegl Chir - 2021 - Vol90 - N4 - p.22-28; PMID:30220673
- Jopek K., Tyczewska M., Celichowski P., Malendowicz LK., Rucinski M. Transcriptome Profile in Unilateral Adrenalectomy-Induced Compensatory Adrenal Growth in the Rat. // Int J Mol Sci - 2021 - Vol19 - N4 - p.; PMID:29642441
- Zhao Y., Guo H., Zhao Y., Shi B. Secreting ectopic adrenal adenoma: A rare condition to be aware of. // Ann Endocrinol (Paris) - 2021 - Vol79 - N2 - p.75-81; PMID:29525561
Diagnosis of sore throat
At the patient’s initial visit, the doctor collects complaints and anamnesis, specifying the duration and circumstances of the onset of symptoms, and the nature of the pain.
This is followed by a general examination of the patient, a visual assessment of the mucous membranes of the mouth and throat, and palpation of regional lymph nodes. An endoscopic examination of the ENT organs – pharyngoscopy – is mandatory. It allows you to examine the tonsils in detail and thus determine the form of the disease. For angina, the following tests are prescribed:
- Clinical blood test. Inflammation is indicated by neutrophilic leukocytosis with a shift to the left and accelerated ESR.
- General urine analysis. It is possible that protein may appear in the biomaterial.
- Rapid test from the tonsils using diagnostic strips to detect group A beta-hemolytic streptococcus.
- Bacteriological examination of a smear for beta-hemolytic streptococcus and diphtheria. Material is collected from the surface of the palatine tonsils and the posterior wall of the oropharynx before using local antiseptic drugs and taking antibiotics.
- If a patient is suspected of having infectious mononucleosis, a blood test is performed to test for IgM antibodies or to identify the genetic material of the Epstein-Barr virus.
- As part of the diagnosis of herpetic sore throat, enterovirus RNA is determined in the blood and throat smear using the PCR method.
Diagnosis of complications of angina after clinical recovery includes the following laboratory and instrumental studies:
- Control general analysis of blood and urine.
- Rheumatic test. Determination of rheumatoid factor, C-reactive protein, antistreptolysin-O, seromucoid in the blood.
- ECG. The electrocardiogram may show signs of hypoxia and conduction disturbances.
Complications of GABHS-pharyngitis
In most cases, GABHS pharyngitis resolves without complications. Non-purulent complications include acute rheumatic fever, post-streptococcal glomerulonephritis, childhood autoimmune neuropsychiatric disorders associated with streptococcal infection. Purulent complications of streptococcal pharyngitis include necrotizing fasciitis and bacteremia.
The differential diagnosis of GABHS pharyngitis includes both infectious and non-infectious causes of pharyngitis.
The main viral diseases manifested by acute pharyngitis:
- infectious mononucleosis - Epstein-Barr virus (EBV) and cytomegalovirus. More common in adolescents and characterized by fever, severe pharyngitis (which lasts longer than GABHS pharyngitis), anterior and posterior cervical or diffuse lymphadenopathy. Periorbital edema, mild hepatomegaly, and splenomegaly may be present. Patients prescribed ampicillin, amoxicillin (sometimes other antibiotics) may develop a characteristic rash;
- primary HIV infection —may cause an acute retroviral syndrome (similar to infectious mononucleosis) in sexually active adolescents or rarely in sexually abused children. Clinical signs of primary HIV infection include severe cervical or generalized lymphadenopathy and complaints of fever, weight loss;
- herpes simplex virus - pharyngitis caused by the herpes simplex virus, manifested by blistering rashes on the mucous membrane, lips;
- influenza - characterized by fever, cough, headache and myalgia, which occur during seasonal epidemics;
- other viral diseases - enteroviruses, adenoviruses, rhinoviruses, coronaviruses, respiratory syncytial virus, parainfluenza viruses.
The main bacterial causes of pharyngitis:
- streptococci of groups C and G - there is still a debate about the role of these bacteria in the etiology of acute pharyngitis;
- n eisseria gonorrhoeae (gonorrhea) is a relatively rare cause of pharyngitis. Most cases are asymptomatic or symptoms are nonspecific (eg, pharyngeal congestion, swelling or exudate in the tonsil lacunae);
- f usobacterium necrophorum (Lemierre's syndrome) is the cause of most cases of purulent thrombophlebitis of the jugular vein. Clinical signs include strep throat, high fever (39°C), respiratory symptoms, unilateral neck swelling or pain;
- diphtheria - rare in developed countries, but important to consider in patients from endemic areas. Unlike GABHS pharyngitis, which has an acute onset, the onset of diphtheria symptoms usually occurs gradually. A distinctive feature of diphtheria is the formation of a gray filmy coating that adheres tightly to the mucous membrane of the nose and throat, the removal of which leads to bleeding;
- others - tularemia (Francisella tularensis), Arcanobacterium haemolyticum, Mycoplasma pneumoniae.
Non-infectious causes of pharyngitis are diagnosed based on medical history. This may be irritation or dryness of the pharynx, a foreign body (for example, a fish bone), chemical exposure, radiating pain due to dental abscess, acute otitis media.
Treatment of sore throat
Depending on the severity of the patient’s condition, treatment of angina occurs under the supervision of a doctor at home or in a hospital.
Bed rest is mandatory, a gentle dairy-vegetable diet enriched with vitamins, and plenty of warm drinks are recommended. For bacterial sore throat, broad-spectrum antibiotics are prescribed. If the disease is caused by streptococcus, penicillin drugs are used. In case of severe intoxication syndrome, intravenous infusion of glucose-saline solutions is performed. Non-steroidal anti-inflammatory drugs are used as antipyretics and pain relievers.
For sore throat, gargling with alkaline and water-salt solutions and irrigating the pharynx with painkillers and antiseptics are recommended. The use of drugs in the form of a spray for the treatment of sore throat is possible only in adults and children over 3 years of age. With the development of purulent complications of the disease, hospitalization of the patient followed by surgical intervention is required.
Author:
Pugonina Tatyana Alekseevna, Therapist
Treatment of acute tonsillopharyngitis
Antibiotic therapy is recommended for any patient with symptomatic pharyngitis or tonsillopharyngitis who has a positive rapid antigen or culture test for group A streptococcus.
Empirical treatment is generally not recommended because there is significant overlap between the clinical features of GABHS pharyngitis and nonstreptococcal pharyngitis. Short delays in therapy (eg, while awaiting culture results) do not increase the incidence of complications, including acute rheumatic fever. However, it is unknown whether such treatment delays affect the incidence of other complications (eg, development of peritonsillar abscess).
If clinical suspicion for GABHS pharyngitis is high and test results cannot be obtained quickly, it is advisable to initiate antibiotic treatment while awaiting test results. If the diagnosis is not confirmed, antibiotics should be stopped.
Antibiotic treatment is not recommended for asymptomatic chronic GABHS carriers or for GABHS carriers with signs of acute viral pharyngitis.
Antibacterial therapy
The drug of choice for the treatment of GABHS pharyngitis is penicillin antibiotics. Penicillin is the only antibiotic that has been studied and shown to reduce the incidence of acute rheumatic fever. For complete eradication of GABHS, the duration of the course of antibacterial therapy is 10 days.
Amoxicillin is more preferable for young children. It can be given once daily using an extended-release form (suspension). In several randomized trials, amoxicillin suspension at a standard dose (once daily) was found to be as effective as penicillin taken orally.
In case of allergy to penicillins or poor tolerance, preference is given to cephalosporin antibiotics, lincosamides (clindamycin) and macrolides - the choice of drug depends on the type of allergic reaction to penicillin.
Studies that combined data from more than 5000 adults and children showed no clinically significant difference between cephalosporins, macrolides, or clindamycin compared with penicillin or amoxicillin in the resolution of GABHS tonsillitis symptoms. But no studies have assessed the use of alternatives to penicillin for the prevention of acute rheumatic fever. Thus, penicillin remains the drug of choice whenever possible.
Tetracyclines, sulfonamides and fluoroquinolones should not be used to treat streptococcal pharyngitis due to high resistance and high side effect profile.
Nonsteroidal anti-inflammatory drugs (ibuprofen) or acetaminophen (paracetamol) may be used to relieve fever and pain.
How is acute tonsillopharyngitis treated at the Rassvet clinic?
When diagnosing a sore throat, we always pay attention not only to the pharyngoscopy picture, but also to the presence of signs of a viral infection. This means we do not perform streptococcus tests on all patients with acute pharyngitis.
If there are signs of GABHS pharyngitis, we must perform a rapid test; if indicated, we take material for testing only for GABHS. Confirmation of streptococcal infection helps prevent unnecessary prescription of antibiotics for viral pharyngitis.
We do not prescribe throat swabs for flora. Streptococcal infection is one of the few causes of tonsillopharyngitis for which treatment with antibiotics is recommended. To this day, the need for antibacterial therapy for most other pathogens remains controversial. Other bacterial infections that strictly require treatment include diphtheria and gonorrhea.
We do not order an ASLO test on the first day of illness (ASLO - antistreptalizin-O, antibodies produced in response to the toxin of group A beta-hemolytic streptococcus). ASLO increases only 10-20 days after the onset of streptococcal infection. There is also no point in monitoring it every week, since this marker begins to decrease 3-5 weeks after the illness, but its levels can be higher than normal for up to a year.
We understand that the main goal of antibiotic therapy for streptococcal pharyngitis is to prevent complications. Treatment with antibiotics has been shown to reduce the severity of symptoms and speed recovery in patients with streptococcal pharyngitis, but even without antibiotic therapy, in most cases, symptoms resolve within three to five days.
We do not treat any plaque in the throat with antibiotics, since their presence does not equal streptococcal tonsillitis, nor vice versa.