fibular
and the tibia are the long bones of the lower leg. The fibula is small and located on the outside of the lower leg. The tibia is a bone located on the inside of the lower leg.
The fibula and tibia meet at the knee and ankle joints. Two bones help stabilize and support the ankle and foot.
A fracture of the fibula occurs when a fall from a height or any blow to the outer surface of the lower leg. Even a sprained ankle can lead to a fracture of the fibula. A fracture of the fibula can occur at any point.
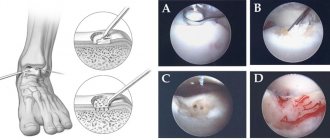
Photo: Medscape Reference
Types of Fibula Fracture
Types of fibula fracture include:
- Lateral malleolar fibular fracture - occurs when the fibula breaks at the ankle joint;
- Fracture of the proximal head of the fibula - localized at the upper end of the fibula in the area of the knee joint;
- Avulsion fracture - a fracture in which the tendon tears off part of the bone from the side of its attachment;
- Stress fractures occur as a result of repetitive trauma while running or walking;
- Fibula fractures are common in athletes, especially those who participate in running, jumping, soccer, and basketball.
fibula
This bone is also located in the lower leg, long and thin, it has two “heads”, upper and lower, the latter is part of the ankle, it stabilizes the ankle joint. Connects to the tibia via an interosseous membrane. The structure is similar to the tibia, but there are important differences. The body of the fibula is slightly twisted and curved initially, but it has a fairly simple structure. It is thin and not as strong as the tibia, but their “tandem” makes the tibia resistant to external injuries.
The fibula has edges:
- Front;
- Rear;
- Medial.
With the help of the thicker distal end, the bone forms the ankle.
Diagnosis of fibula fracture
People with a leg injury should see a doctor for a diagnosis. During the diagnostic process the following is carried out:
- Physical examination
- the doctor will look for any noticeable deformities; - X-ray
- used to detect a fracture or displacement of a bone; - Magnetic resonance imaging
(
MRI
) - provides a more detailed scan and can produce detailed pictures of internal bones and soft tissues; - Computed tomography
(
CT
) and other tests may be performed to make an accurate diagnosis and assess the severity of a fibular fracture.
Where is the fibula located?
The fibula is located at the bottom of the human skeleton, more precisely in the lower leg.
Bone restriction:
- At the top is the knee joint;
- Below is the ankle.
There are large and strong ligaments between the tibia and fibula. There is a hole on the back side of this bone; it exists so that vessels and nerves enter it; they pass through the canal into the bone and interact with the rest of the canals of the human skeleton.
The main function of the fibula is the ability of the foot to rotate in different directions relative to the lower leg.
This function is the most important, but because of this possibility, it is at great risk of being broken. Although the bone is small and thin, it should not be underestimated; it is very important for the skeleton, for its stability and ability to move.
Open fracture of the fibula (compound fracture)
In an open fracture, part of the bone passes through the skin and comes out. Open fractures are often the result of severe trauma or a direct blow, such as a fall or auto accident. This type of fracture is often accompanied by additional injuries. Some injuries can be potentially life-threatening.
Open fibula fractures should be treated immediately. Patients are given antibiotics to prevent infection. The wound is thoroughly cleaned and internal fixation with a plate and screws is used to stabilize the fracture. A bone graft is used to speed up healing.
Description of BBK
The largest component of the tibia is called the tibia, its anatomy has one feature. Its second, but separate half is adjacent to the LBC. This is the fibula. The tibia and fibula are attached to the femur and patella. At the bottom they form the ankle and adjoin the talus.
The anterior edge of the tibia looks like a pointed ridge. It is lumpy on top. There is a small connecting cartilage between the shin bones. The surface of the tibia is convex and can even be felt through the skin. The lateral part is concave, the posterior part is flat, with the soleus muscle. Below is the nutrient opening.
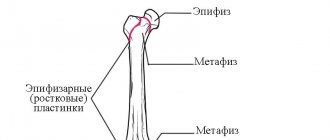
The proximal epiphysis is slightly expanded. Its sides are called condyles. Outside the lateral one there is a flat articular surface. At the top of the proximal epiphysis there is a small elevation with two tubercles. The distal epiphysis is quadrangular. On the lateral surface there is a fibular notch. Posterior to the epiphysis is the ankle groove.
Read also…. Bee saved: scam or not? Instructions for use, composition, reviews
Closed fracture (simple fracture)
With a closed fracture, the skin remains intact. The goal of treating closed fractures is to realign the bone fragments, control pain, allow time for the fracture to heal, prevent complications, and restore normal function of the leg. Ice is used to relieve pain and reduce swelling. The leg should be in an elevated position.
If surgery is not required, a brace or cast is used, and crutches are recommended when walking. After fusion, it is necessary to strengthen the weakened joints with the help of physical therapy.
Location
The shin is where the tibia bone is located. It consists of two parts and is located at the bottom of the leg. The tibia (TT) is located medially. It is long, has a 3-sided body and two epiphyses. The upper end of the tibia is involved in the formation of the knee joint. The tibia is the strongest bone in the human skeleton. The tibia can withstand a maximum load of up to 1650 kilograms.
Contents of the article: Description and fractures of the ankle joint Pain in the lower leg Fracture of the ankle joint Treatment of injuries
The fibula (FIB) is less massive and is located laterally. It is long and tubular, attached to the big one and limits the ankle. Fractures and injuries to the spinal cord are rare.
Prevention of recurrent fibula fracture
To prevent future fibula fractures, athletes should wear appropriate safety equipment.
To reduce the risk of fracture, you must:
- Wear suitable shoes;
- Follow a diet rich in calcium products, such as milk, yogurt, cheese;
- Do exercises to strengthen your bones;
- A fibula fracture usually resolves without further problems, but complications may occur:
- Degenerative or traumatic arthritis;
- Abnormal deformities or dysfunction of the ankle joint;
- Constant pain;
- Damage to the nerve and blood vessels around the ankle joint;
- Chronic swelling of the limb.
Most fibular fractures do not have any serious complications. Within a few weeks to several months, most patients recover completely and can continue their normal activities.
Cyst
When the tibia hurts, this may mean the appearance of a cyst. This is a disease when a thickening appears in half of the tissue. Cysts are a manifestation of the dystrophic process.
Read also…. Electrophoresis with Lidase: for what conditions is it indicated, the cost of the procedure and patient reviews about it
The thickening is based on poor circulation and the active activity of lysosomal enzymes, which lead to a decrease in collagen and other beneficial substances and proteins. A cyst refers to neoplasms that can be either benign or malignant.
They are discovered when the tibia bone in the leg begins to ache . The cyst can be aneurysmal or solitary. It develops over a long period of time. A solitary cyst is most often found in young men. An aneurysmal neoplasm appears suddenly. Typically, such a cyst appears after an injury or bone fracture.
Degrees of ligament damage
Different degrees of damage produce both differences in the clinical picture and require different treatment tactics. Highlight:
- First degree- This is a partial rupture of the surface fibers. Pain occurs at the site of deformation, and swelling is possible.
- The second is damage to most ligamentous fibers. The pain is more widespread, swelling of the joint increases quickly, may be associated with hemarthrosis, and a hematoma occurs on the lateral surface of the joint.
- The third is a complete break. In addition to the above symptoms, joint dysfunction and instability appear.
Osteosynthesis using pins (rods)
This type of surgical treatment is also called intraosseous or intramedullary. In this case, the pins are inserted into the internal cavity of the bone (marrow cavity) of long tubular bones, namely their long part - the diaphysis. It provides strong fixation of fragments.
Intraosseous osteosynthesis is performed using open, closed and semi-open methods.
With open intramedullary osteosynthesis, open reposition of the fragments is performed and a pin is inserted intraosseously. With closed intramedullary osteosynthesis, bone fragments are reduced, and then, under X-ray television control, without exposing the fracture area, a pin is inserted through a hole in the proximal or distal fragment into the medullary canal. With semi-open intramedullary osteosynthesis, the fixator is also introduced outside the fracture zone, but due to the fact that completely closed reduction is impossible due to the comminuted nature of the fracture or interposition of soft tissues, a small incision is made above the fracture area and the fragments are reduced. The advantage of intramedullary osteosynthesis with pins is its minimal trauma and the ability to load a broken limb within a few days after surgical treatment. Non-locking pins, which are rounded rods, are used. They are inserted into the medullary cavity and jammed there. This technique is possible for transverse fractures of the femur, tibia and humerus, which have a bone marrow cavity of a sufficiently large diameter. If more durable fixation of fragments is necessary, drilling of the spinal cavity using special drills is used. The drilled spinal canal should be 1 mm narrower than the diameter of the pin in order for it to be firmly jammed. To increase the fixation strength, special locking pins are used, which are equipped with holes at the upper and lower ends. Screws are inserted through these holes and pass through the bone. This type of osteosynthesis is called blocked intramedullary osteosynthesis (BIOS). Today, there are many different types of pins for each long tubular bone (femur, tibia, humerus, radius, ulna, fibula), and there are pins for osteosynthesis of certain parts of bones (for example, for the proximal and distal parts of the femur).
Using locking screws, a strong fixation of the pin is achieved in the areas of the bone above and below the fracture. Fixed fragments will not be able to shift along their length or rotate around their axis. Such pins can also be used for fractures near the end portion of long bones and even for comminuted fractures. For these cases, pins of a special design are made. In addition, the locking pins can be narrower than the medullary canal, which does not require drilling out the medullary canal and helps preserve intraosseous blood circulation.
In most cases, blocked intramedullary osteosynthesis (BIOS) is so stable that patients are allowed dosed loads on the damaged limb the very next day after surgery. Moreover, such a load stimulates the formation of callus and fracture healing. BIOS is the method of choice for fractures of the diaphysis of long tubular bones, especially the femur and tibia, since on the one hand it least disrupts the blood supply to the bone, and on the other hand it optimally accepts the axial load and allows you to reduce the time of using a cane and crutches.
Causes of injury
Let us first consider the mechanism of injury to the medial collateral ligament. As already mentioned, she gets injured quite often. The situation in which this occurs is a blow just below the knee from the outside of the shin. In this case, the leg is usually in an extended position and is more susceptible to injury (happens more often in football players). Otherwise, this can happen during falls, when the lower leg is fixed, and the body moves relative to it to the side with torsion on the leg (injuries of skiers and snowboarders). When the external collateral ligamentous fibers are torn, on the contrary, the blow should fall on the inner surface of the lower leg, and also excessive extension of the knee or internal rotation of the body on the supporting leg should occur.
Pain in the lower leg and its bones
Pain in the lower leg can have various causes. For example, from excessive training, when the tibia begins to ache after running. It can become more fragile if there is a lack of calcium, magnesium and other essential elements in the body. They are often washed out when a person uses diuretics.
When the tibia hurts in the front, this may be a consequence of joint disease or excessive stress that the legs unexpectedly felt after a long period of stagnation. The causes of negative sensations can be inflammatory processes or an infection that affects bone tissue. Very rarely, a malignant tumor may appear on the bone.