Signs of bone sarcomas
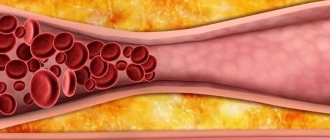
Diagnosing bone sarcomas at the initial stage of development is extremely difficult. Specialists and patients often mistake dull pain in the joints for inflammatory processes or the consequences of injuries, and are in no hurry to conduct a thorough diagnosis. As the tumor grows, the tissue above it becomes swollen, with a pronounced vascular network.
The joint becomes inactive, contracture develops and a pronounced limitation of physical activity occurs; patients often take a forced position of the body. The tumor itself, when palpated, can be painful and inactive. The local temperature of the pathological focus is often elevated. The pain tends to get worse at night.
Among young patients, the following are common: osteoscarcoma, Ewing's sarcoma, and malignant fibrous histiocytoma. At a more mature age, the following types of bone sarcomas are diagnosed: chondrosarcoma, malignant fibrous histiocytoma, fibrosarcoma. As a rule, such neoplasms metastasize to the lungs, bones and liver.
Methods for diagnosing bone sarcomas:
- X-ray examination;
- tumor puncture with morphological examination of tissues;
- computer, magnetic resonance imaging;
- positron emission tomography scintigraphy.
Features of treatment of bone sarcomas
With the development of modern medicine, significant breakthroughs have been achieved in the treatment of sarcomas. Today, many patients have access to organ-preserving surgical treatment methods, as well as combined methods, including radiation therapy and chemotherapy drugs (cytostatics). Many bone tumors are sensitive to cytostatics and are treated quite successfully with their use. If you seek medical help in a timely manner and carry out effective treatment, the prognosis is generally favorable.
Psychological aspects in the treatment of osteosarcoma
Most cases of osteosarcoma occur during adolescence, the most sensitive period of a person's life.
All this leaves a deep imprint on the patient’s life, including the ability to attend school, engage in sports, work and other activities. The first year of treatment is a particularly difficult period.
Help from family members, friends, medical personnel and psychologists can have a positive impact on a person with osteosarcoma.
Conversations with patients who have already undergone treatment for the same disease may also be useful.
Osteosarcoma
Osteosarcoma is a malignant neoplasm that affects the human skeletal system and rapidly develops with the formation of multiple metastases. The tumor occurs mainly among young people. Sarcoma originates mainly in the metaphysis - the section of long tubular bones adjacent to the epiphyseal plate. The tendency to early metastasis makes this disease extremely malignant and dangerous.
The majority of patients with osteosarcoma are young men under 25-30 years of age. A surge in the disease is observed during puberty and accelerated skeletal growth. The tubular bones of the lower extremities are affected several times more often than the upper ones. As a rule, the pathological focus covers the femur, humerus or tibia.
What parents need to pay attention to
Early symptoms:
Pain
The first significant symptom is increasing pain in the affected limb. After some time, the pain becomes unbearable, depriving sleep, it can appear both during exercise and at rest and is not relieved by conventional analgesics.
Swelling
The affected part of the bone increases in volume, the soft tissues above it become swollen, and phlebectasias (a network of small dilated veins) appear on the skin.
Impaired function of the affected limb. Restricted mobility in a nearby joint
When osteogenic sarcoma is localized in the bones of the lower extremities, movements in the joints become difficult, and lameness develops over time. A late symptom of this disease may include a pathological fracture in the area of the primary lesion.
The main problem of late diagnosis of osteogenic sarcoma is due to the fact that for a long time local pain is associated with a previous injury to the limb. But at the same time, the severity and duration of pain symptoms are not compared with the extent of the injury.
Unfortunately, pain in the extremities in children and adolescents often goes unnoticed or underestimated and is associated primarily with “growing pains,” as a result of which the child receives long-term analgesic therapy without effect.
The duration of the pain syndrome, its pronounced nature, not correlated with previous traumatic changes, is always a reason for an expanded diagnostic search.
Signs of progression
Like all malignant bone tumors, osteosarcoma is diagnosed quite late. Many people (and doctors too) mistake dull, sudden pain in the joints for signs of an inflammatory process (myositis) or echoes of an injury received several months ago. In fact, it is osteosarcoma that progresses, taking over more and more healthy bone tissue.
As the disease progresses, more noticeable signs of pathology begin to appear: - the appearance of a tumor and characteristic effusion in the joint; - increased pain; - pain of the pathological focus upon palpation; - decreased activity, lameness, restrictions in movement (joint contracture); - tumor growth into muscles; - formation of metastases, spread of malignant cells through the bloodstream to the lungs and brain; - swelling, redness of the tumor, the appearance of a pronounced vascular network on its surface.
If you seek medical help at the first pathological signs, undergo a routine x-ray examination, and be vigilant, then subsequent treatment will be more effective. Often, osteosarcoma is diagnosed in the later stages of development, when metastases are detected in many organs and tissues, but even in this case, well-chosen treatment can save a person’s life and health.
The most common locations
A malignant tumor primarily affects the bone tissue of long tubular bones. All other types of bones account for 20% of the damage. Osteosarcoma of the hip, i.e. femur, its distal end is the most common site of tumor formation. The disease occurs in flat bones, bones of the feet, hands, spine, and skull very rarely.
The area of the metaphysis of the bone is closer to the joint, this is where the neoplasm will be localized. But there are exceptions when, during the disease, the metaphysis remains unchanged, and it is the diaphysis that is affected. Also, doctors already know where exactly the metastases are located on a particular bone, for example, if the hip bone is affected, then the neoplasm should be looked for in the area of the distal end. With pain in the tibia, the internal condyle is affected, with pain in the humerus, where the roughness is located in the deltoid muscle.
Diagnostic methods
The initial stage of osteosarcoma has practically no symptoms. The patient may experience minor aching pain in the joint, but there are almost never external signs of the disease (swelling, redness, small dilated veins). The absence of pronounced symptoms misleads both patients and doctors themselves.
Often, when visiting hospitals and clinics, people with osteosarcomas begin to undergo anti-inflammatory therapy. Some of the prescribed techniques may not only be ineffective, but also dangerous. For example, warming physiotherapeutic procedures can accelerate the growth of tumor cells. The patient should be interested in the prescribed treatment and insist on a high-quality and more detailed diagnosis. Especially in cases where the doctor, due to lack of time or for some other reason, does not strive to get to the bottom of the truth and find the true cause of the patient’s poor health.
Common diagnostic methods used for osteosarcoma include the following:
- radiography: the most accessible diagnostic method for all malignant bone tumors;
- tissue biopsy, tumor histology;
- laboratory examination of blood parameters: in patients with osteosarcoma, some indicators are elevated (lactate dehydrogenase, alkaline phosphatase);
- computed tomography: allows you to detect metastases, but, as a rule, the smallest of them are never detected;
- skeletal scintigraphy;
- arteriography.
If questionable results of the study are obtained, it is recommended to carry out a number of additional diagnostic procedures. A thorough examination is necessary to select the correct treatment tactics and predict the outcome of the disease.
Osteosarcoma is a bone disease that is treated
May 12, 2021 2338 1
The insidiousness of the disease is that it comes quietly, and the first symptoms can easily be attributed to the consequences of a bruise or rheumatism. This is what usually happens: the tumor grows unnoticed, and when pain occurs, it is mistaken for something else. But to treat osteosarcoma, it is extremely important not to waste time. With modern medical capabilities, a patient with this disease in the early stages has a survival prognosis of 70-80%, and sometimes higher.
What is osteosarcoma?
Osteogenic sarcoma is a malignant tumor of bone tissue elements. It may contain chondroblasts and fibroblasts in varying volumes: the former are cartilage cells, and the latter produce collagen.
This is not “bone cancer,” as some write and say - people are just used to calling any dangerous tumors a scary three-letter word. But cancer, or carcinoma, grows from epithelial cells, and all sarcomas, including bone sarcomas, develop from different types of connective tissue.
The disease usually affects long tubular bones, while flat and short bones—those forming the ribs, shoulder blades, and sternum—happens much less frequently.
The legs are most often affected - in four out of five cases the tumor affects the knee joint. After the femur and tibia, the most vulnerable are the humerus, fibula, elbow and pelvis. In some, more rare cases, the disease also affects other areas - the spine, jaw, and parts of the skull.
To understand how the disease occurs, let’s figure out what the hardest structures of our body are made of and what processes occur there.
How are bones formed?
Bone tissue is a hard, lime-impregnated substance that forms the basis of the skeleton, which provides us with support and support in this world, although the functions of bones are not limited to this.
Three types of cells are responsible for its growth and renewal:
Osteoblasts -
“young activists” who actively produce all sorts of important substances, including calcium salts and collagen.
They are found most often in growing tissue, but they also come to the rescue when you need to help bones heal after injury. Then these cells mature and become less active, turning into osteocytes
- “conservative citizens” who have found a place for themselves and are firmly established in it.
And osteoclasts are
a “cleaning company” that helps to promptly get rid of excess particles by dissolving them to make room for new ones.
What could go wrong?
One day - this can happen in any part of the human or animal body - among a group of healthy cells, one appears with altered DNA. Why its genetic code was broken, scientists do not have a single answer to this question. Such a particle behaves differently from others: it does not work for the common good, gradually displaces healthy “comrades”, takes away their food and multiplies vigorously. The accumulation of “egoists” grows and after some time they form a tumor that poses a threat to life.
A malignant cell has two features that make it so dangerous. Firstly, it is not susceptible to natural aging and dying - apoptosis, or programmed death, does not affect it. The pest will not die naturally, and will multiply its own kind until it is stopped. And the second insidious feature is that it is able to travel throughout the body and create islands of disease there - metastases, which are very difficult and not always successfully combated.
When such a process develops in bone tissue, it is called osteosarcoma.
It is generally accepted among experts that the disease is triggered by young cells at the moment of their “self-determination”: as if parsley was supposed to grow from seeds, but a weed also sprang up and displaces a useful plant from the garden bed.
How long does it take from cell mutation to disease?
Oncogenesis, or the process of the appearance and accumulation of malignant particles in the human body, takes time, and sometimes it lasts for years. One changed cell is not enough - the mutation needs to occur more than once, and finally lead to the appearance of such “heirs” that could afford to behave as independently and aggressively as possible in the body.
There are tumor diseases that take a long time to develop, starting as conditionally malignant. Violations make themselves known in advance, and regular preventive examinations are guaranteed to save the organ, health, and even life. This way you can monitor the condition of the mammary glands or cervix; Some types of skin cancer take a long time to mature - for example, basilioma.
The bone is another matter: here everything happens more unnoticed and faster. No one can predict the exact time for the development of the disease to one stage or another, but it is known that with osteosarcoma, on average, it takes 140 days for the number of malignant cells to double.
Osteosarcoma: how to recognize and treat? April 29, 20211214 1
Who can this happen to?
The “risk group” includes people from 5 to 25 years old, but twelve to sixteen year olds are most often affected.
The fact is that during this period the bones have not yet fully formed; they are undergoing an active growth process. Often in adolescents, the limbs look disproportionately long - because the process of change occurs too quickly and unevenly, the rest of the body does not keep up.
Until about the age of 25, our bone tissue continues to form. This occurs in the area of the so-called “growth zones” - cartilaginous plates located at both ends of the long bones, near the joints. Later, when growth ends, the tissue will turn from cartilage into bone, but while the cells are actively dividing, these areas are especially vulnerable. Therefore, osteosarcoma of the tibia and lower part of the femur are most common, and the area near the shoulder joint is also affected.
Children have other dangerous places: for example, in infants, a tumor can affect the bones of the skull.
Although older people are not included in the risk group, this possibility cannot be completely excluded: the disease can occur in anyone and in any part of the skeleton, and the risk increases in older people - when the body’s resistance as a whole has decreased, and health problems have accumulated.
What factors increase the risk of disease?
Experts are trying to find the causes of the disease and suggest some risk factors, but find it difficult to establish a cause-and-effect relationship between them and osteosarcoma. Today we can speak with confidence only about the influence of radioactive exposure - and the effects of radiation can appear even after decades.
There are hypotheses about heredity, but there are no direct explanations of how it works and what the risks are. The appearance of bone sarcoma is also associated with Paget's disease, in which abnormally rapid tissue metabolism occurs - but this complication occurs in one patient out of a hundred. Children also suffer from a rare eye disease - retinoblastoma; in victims of it, osteosarcoma is diagnosed more often.
Some believe that multiple injuries lead to illness - but it is not obvious what is considered a cause and what is a consequence. Many doctors, on the contrary, say that the injury only draws attention to the problem: only after the affected bone was touched - for example, while playing sports - did the person begin to understand that something was wrong with him.
Types of disease
There are many of them, and they stand out according to different characteristics. For example, according to the shape shown by x-ray, osteosarcoma may look like a single tumor with unclear boundaries beyond which it extends; there may be an option when the formation fills the bone from the inside, replacing the previous contents. And there is also a mixed version - at the same time the membrane is destroyed and the internal space is filled with malignant cells.
The clinical course of the disease is rapid
or
slow
. The first is characterized by a high rate of division of malignant cells, increasing pain and impaired mobility of the limb. The second is less common: it is a gradual and imperceptible development without obvious signs and discomfort - such a tumor is more successfully treated if it can be recognized in a timely manner.
Ewing's sarcoma October 27, 2020856 81
The detected neoplasm may have a different location: sometimes it is limited to only one zone and does not affect other organs, but only nearby tissues; it happens that it has already metastasized, and islands of malignant cells are found far from the primary focus. And sometimes, at the time of diagnosis, the disease is already developing simultaneously in several bones.
Osteosarcoma comes in different grades of malignancy - low, moderate and high. To understand this, they study differentiation, that is, the determination of the structure of the changed cell: the more similar it is to its healthy “ancestors” and the easier it is to understand its origin, the less danger it poses.
Malignancy is indicated by the letter G and the corresponding digital value: G 1
— the cells are highly differentiated, that is, their structure is as close as possible to healthy ones, and this means a low degree of aggressiveness of the disease;
G 2
- moderate differentiation and degree;
G 3
- malignant cells are difficult to detect, have a strong difference from a healthy structure and, accordingly, a high level of malignancy;
G 4
- not detectable at all, the most aggressive.
Unfortunately, osteosarcomas with low and moderate grades are much less common than with high grades: mildly aggressive cases account for slightly more than 1% of all malignant bone diseases, while “malignant” variants account for 80-90%.
Sarcoma October 27, 20201139 55
But the names of some of the most common types were given based on the microscopic properties of the tumors.
Classical
occurs in 80% of all cases, and is divided into three types:
- Osteoblastic, or true, sarcoma is formed from bone tissue cells, and most often affects the areas of the legs, arms and pelvis;
- Chondroblastic mainly consists of cartilaginous plates;
- Fibroblastic
is when the tumor has few bone cells, but many structural components - for example, collagen.
All three species are characterized by a high level of danger and rapid growth.
Ewing's sarcoma —
named after the doctor who discovered this disease
-
it belongs to a separate species, but it is worth mentioning, since it is attributed to 10-15% of all bone tumor diagnoses, and it is also very aggressive. Usually destroys the bones of the legs and pelvis. This disease is sometimes called "Ewing's osteosarcoma."
Telangiectatic osteosarcoma is also considered highly dangerous.
- consists of many balls filled with blood, and externally separated from each other by partitions;
small cell
- it most often destroys the femur,
highly malignant superficial
,
secondary
and
extraskeletal
tumors. But they are not common and are rarely diagnosed.
Among non-aggressive species called low-grade central
and
paraosseous -
as already mentioned, they are also rare to meet.
There are tumors that occupy an intermediate stage between very dangerous and slightly aggressive: for example, periosteal
.
Sometimes malignant tumors in the bone appear as a result of another disease, and then this is called a “secondary lesion.” The most common causes are lung, thyroid, breast, kidney and prostate cancer. Such a formation is not osteosarcoma - but it happens that this is where the disease is discovered for the first time.
Warning signs of osteosarcoma
The first thing that can cause anxiety is pain in the leg, shoulder or some other place. Determining exactly where it hurts is not so easy. The pain may not be strong or acute, it may increase or subside; it is usually more noticeable at night. It may seem that this is rheumatism, since the sensations are similar.
If there was a bruise or injury before, then people usually think that there is nothing to worry about: they apply ointments to the affected areas, take painkillers and wait for everything to go away. But the longer it lasts, the stronger the pain becomes, and sooner or later you will still have to go to the doctor.
After a person has tried for some time not to notice or to treat the sore spot on his own, a swelling or thickening may appear there. If the knee joint hurts, it becomes more difficult to walk, and the person begins to limp. Due to the pressure of the tumor on the tissue, spider veins may appear on the skin. Sometimes the disease leads to fractures.
Here are the symptoms of osteosarcoma, which are characteristic of all malignant tumors:
- nausea due to released toxins;
- vomit;
- lack of appetite;
- fatigue;
- temperature increase.
If your leg, arm or shoulder hurts, and in addition one of the above begins to bother you, or even several of the points coincide, you cannot hesitate, but urgently need to go to the hospital. Typically, the patient sees a doctor about three months after the disease has already begun to manifest itself. By this point, in 10-20% of cases, X-rays already show malignant formations in the lungs, and computed tomography reveals microscopic metastases in 80%.
How is the diagnosis done?
To establish a diagnosis and identify the full picture, the patient is prescribed a series of examinations. Exactly how to take x-rays of the area where a tumor is suspected will depend on the choice of the attending physician.
Here are the methods that are commonly used:
- X-ray examination
of the affected area in two projections is the first thing that will be done in the direction of a surgeon or traumatologist; it will show the approximate size of the tumor, whether it contains soft tissue components; if there are fractures, it will reveal them too; - CT scan, or computed tomography
- it will be prescribed by an oncologist if there are indications for such an examination. The image will show the pattern of bone tissue, the exact location of the tumor and its size, and the presence of metastases in the lungs. Here, CT will be much more effective than conventional x-ray; - Ultrasound, ultrasound examination
- the doctor will look at the condition of the abdominal cavity in order to identify secondary growth areas in other organs; Typically, only the lungs are affected, but in rare cases the liver may be affected. - MRI, magnetic resonance imaging
and
PET, or positron emission tomography - it
is prescribed to clarify the area of soft tissue damage in the tumor area; this study is usually prescribed after an x-ray or CT scan; - A general
and
biochemical blood test
is needed to identify concomitant diseases, as well as look at the level of alkaline phosphatase
-
an increased level indicates that the formation is actively progressing. - A biopsy
allows you to accurately determine the nature of the tumor and its malignancy.
All this data will enable doctors to create the most complete picture of the disease and prescribe the correct treatment.
What are the stages of osteosarcoma and how are they determined?
Staging systems accepted by the medical community are used to determine the severity of the disease.
TNM system
, to establish the stage of osteosarcoma, it is necessary to take into account factors such as:
T
– lat.
tutor “tumor” - the size of the primary tumor; N
– lat.
nodus “node” - the presence or absence of tumor foci in malignant nodes; M
– Greek μετάστασις - “movement” - a factor in metastases found in distant organs and tissues.
And here the level of malignancy of the tumor, which is designated by the letter G, is very important - we have already described what they are like above.
This system is used as the main one, although experts periodically make attempts to improve something in it and create new versions. Variations are added to the main stages - this makes it more convenient for doctors to more accurately make a diagnosis on which treatment depends.
Well, now it’s enough for us to figure out the main thing - how exactly the severity of damage is determined and what happens to a person at each of the four stages of the disease.
Stages of development of bone sarcoma stage I
: the tumor size is less than 5 cm, and the degree of malignancy is low or moderate - that is, it is easy to recognize the original structure of dangerous cells;
Stage II
: the formation may be larger, but its boundaries with healthy tissue are still defined;
the level of aggressiveness does not matter; Stage III
: the contours of the tumor are difficult to determine, the disruption of cell structure may vary;
metastasis has already begun; Stage IV
: the size of the tumor is not determined, metastases are present in the body.
What is the treatment for osteosarcoma?
At the end of the twentieth century, the main and almost the only method of treating sarcoma was amputation of the limb along with the tumor. Alas, this did not save many people, only 15-20% of all patients. Fortunately, the situation has changed a lot since then. This was facilitated by the development of biochemistry - new chemotherapy drugs appeared, and technological progress - it gave us more advanced diagnostic systems, and also made endoprosthetics
– replacement of a damaged bone fragment with its analogue made of special materials, which will perform the functions of the removed organ.
All these possibilities greatly influenced the course of treatment and its results.
Today, the classic version of therapy consists of three stages.
First, neoadjuvant, that is, preoperative, chemotherapy for osteosarcoma is carried out - this is a preparatory period, and it usually takes several weeks. During the procedure, a substance is infused that kills tumor cells, causing it to become smaller in size.
The second important goal of this stage is to see how the formation reacts to the introduced chemicals, what kind of response it gives. This way, doctors will receive valuable information about the quality of the tumor and its possible behavior after surgery, and this will allow them to correctly adjust further treatment. There are special drug programs for preoperative therapy.
Then, after preparation is completed, the operation is performed. Here, the main goal of doctors is to remove the formation as completely as possible, without damaging it in the process, so as not to cause metastasis. The doctor tries to perform a “wide resection,” that is, to remove the tumor in its entirety and at the same time include the edges of healthy tissue.
When a joint is damaged due to osteosarcoma, which happens very often, in most cases it is replaced with an artificial one during surgery, and this allows the limb to be saved. Today, the most convenient option is considered to be a modular design, which can be assembled from several parts directly during surgery, taking into account the anatomical characteristics of the patient. If an endoprosthesis needs to be installed in a child, then a special sliding one is used - such structures are created taking into account the growth of the skeleton.
In developed countries and well-equipped clinics, endoprosthetics are used whenever possible, that is, in approximately 80% of cases. However, there are situations when amputation cannot be avoided. Such a need may arise, for example, if the affected area is too large, especially if soft tissue is also severely damaged. Then, after healing, prosthetics will be needed - evolution has also taken place here, and a person with a prosthesis will be able not only to live, but also to remain socially active.
The third and final stage of the treatment itself will be a postoperative course of chemotherapy.
. Before it is prescribed, a histological examination of the removed tumor will be carried out - and then it will be clear whether to continue using the previously chosen regimen or change it. The drugs will be selected in such a way as to destroy as much as possible the malignant cells that still remain in the body and can create new lesions. In addition to standard regimens, today other substances that enhance the effect of chemotherapy can be used. This process lasts several months, with breaks between courses. The entire treatment period will be 9-12 months.
Radiation therapy March 13, 202035110 2888
Radiation therapy is sometimes used as one of the methods of combating dangerous cells. Today its use is not very common, since chemical preparations give better results. But in some cases, radiation is indicated: for example, it is prescribed in palliative therapy to relieve pain, or in the treatment of chondrosarcomas that are not sensitive to chemotherapy.
What determines the survival prognosis?
Many different factors play a role here: the volume of the tumor, its location, differentiation, or the degree of malignancy of the cells, the clarity or blurring of the boundaries of the tumor, the patient’s age, his general health, the tumor’s response to chemotherapy. Even the stage does not always accurately indicate whether a person will recover or whether the disease will return again.
Prognosis is the patient's survival rate, an approximate figure indicating a person's chances for the next five years after the end of treatment. Experts also take into account another number - it determines the probability of the absence of new metastases during this period.
The volume of the tumor is very important: it is believed that if it is less than 70 ml, then the prognosis is favorable - 97%, and if it is more than 150 ml, then the risk is high, and it increases if the tumor is insensitive to chemotherapy - about 17% survival. A neoplasm from 70 ml to 150 ml represents an average degree of danger, and here the prognosis is approximately 67%.
If we rely on the stage of development of the disease, then we can focus on the following figures: with I and II, 70-80% success and higher are expected, provided that the malignant cells are sensitive to drugs; Stage III has a cure rate of about 30%, while stage IV has the lowest prognosis of approximately 15%.
If a relapse occurs, that is, if the disease returns after some time, the prognosis for cure is noticeably reduced and is already less than 25%.
Research is currently underway in Europe and North America - groups of scientists are cooperating to increase the chances of recovery for those patients whose illness did not subside the first time.
How often should I be checked after treatment?
After the operation there is a period of recovery and observation. After three months, the patient undergoes an X-ray, CT and MRI of the operated area, and a CT scan of the chest. These tests are performed to determine whether cancer has developed in the bones and lungs. Additionally, an ultrasound may be prescribed for the same purpose. Then, during the first two years, you need to see a doctor four times a year - doing everything the same, except MRI —
it will be prescribed if there is a suspicion of relapse. For the third and fourth years, the patient undergoes these checks once every six months, and then, at least until the end of ten years, once a year is enough. If during this time the disease has not returned, then the prognosis that this will not happen increases greatly: for example, when after recovery the patient’s chances of not getting sick were 65%, then after ten years they increase to 85%.
Do I need to be examined for prevention?
The ability to easily and safely identify a disease at a very early stage would be a gift for everyone: periodic examinations could be prescribed for children and adolescents, and none of them would ever get sick, and if they did, they would be quickly and successfully cured. But there are no options for preventive cancer screening for osteosarcoma yet. A doctor does not have the right to prescribe a computed tomography scan of the bone without indications, and a simple preventive examination is unlikely to reveal anything at the very beginning of the development of the disease.
Then what is in our power?
- Do an extended blood test instead of a standard one
When undergoing a preventive examination or solving some other health problems, we sometimes donate blood. There is a routine clinical test that reveals the number of red and white blood cells, hemoglobin level and other standard indicators. But if we take the advanced test rather than the general test, we will learn more about our health. Some tests can detect elevated alkaline phosphatase levels or excessive amounts of calcium. If, when donating blood “for show,” you ask for an expanded version instead of the usual standard, there will definitely be no harm, and it will add peace of mind. - Show attention to the health of yourself and those around you
When something unusual happens in the body, anxiety begins to speak up - but we often “shut it down” because we are scared, or have no time, or are simply not used to taking care of ourselves. And it is important to listen to the sensations of your body and understand what exactly is wrong. Well, if something bad happens to a loved one, and he ignores it, well, you will have to become that same harmful neighbor who will not lag behind until he is convinced that there is no reason to worry. - Do not self-medicate, but go to a specialist. It
is highly recommended not to experiment with medications, nor to rely on the magical power of your grandmother’s tincture: rubbing and warming a sore spot is generally a risky undertaking. The best solution would be to make an appointment with a surgeon or traumatologist - this will at least help dispel unnecessary fears, and even save a life. - Correctly convey information to the doctor
At the appointment, you need to explain your concerns to the specialist with all the convincing that you are capable of. It is likely that he will not see any reason for concern and will say that your teenager has a normal bruise, which is a common thing if he, for example, plays sports. But your task is to explain that the symptoms are not typical, and they differ from the consequences of household or sports injuries. The doctor does not know you and your loved ones as well as you do, and the disease at an early stage cannot be visually identified - so do not give in to the temptation to calm down, but ensure that the necessary studies are carried out.
Features of treatment of patients with osteosarcomas
High-quality treatment of osteosarcoma should be carried out in a special oncology department, in a clinic specializing in providing medical care to patients with bone tumors. Treatment tactics are selected strictly on an individual basis, taking into account the stage of the disease, tumor size, patient’s age and other characteristics.
As a rule, the choice of doctors when treating patients with sarcomas is complex treatment, including surgical removal of the tumor, radiation and drug therapy. A course of chemotherapy is usually given before surgery. The use of modern chemotherapy drugs makes it possible to reduce the size of osteosarcoma and destroy micrometastases that were not detected during diagnosis.
During the operation, the entire pathological focus is removed, including healthy tissue. Until recently, patients with osteosarcomas underwent amputation. Today, the possibilities of surgery make it possible to eliminate tumors while preserving a limb, replacing part of the bone with an endoprosthesis made of metal, plastic, or the patient’s own bone tissue. Currently, amputations are carried out only for special indications (for large tumor sizes, often relapsing course of the disease). In addition to resection of the tumor focus, operations are performed to remove distant metastases from the lungs and resection of lymphatic vessels affected by the oncological process.
After surgery, chemotherapy is given. A repeated course of using cytostatics allows you to completely destroy all the smallest metastases in the body. Thanks to the active use of new generation combination drugs, it is possible to avoid many complications that usually occur after chemotherapy treatment. In rare cases, radiation therapy is also used.
Classification
According to the WHO classification, there is a localized (locally advanced) version of osteosarcoma - 80% and a generalized (metastatic) - 20% of cases. Based on the examination of the material obtained through biopsy, the pathologist gives a histological assessment of the tumor. Tumors are divided into central (high and low grade of malignancy), superficial, intracortical, gnotic, extraskeletal and secondary - associated with Paget's disease, radio-induced, as a rule, this is a variant of high grade of malignancy.
In addition to histological classification, the TNM system is used, which evaluates the size of the tumor, the extent of damage to regional lymph nodes, the presence or absence of distant metastases, and the degree of differentiation of tumor tissue.
Based on the data from instrumental studies and histological findings, the disease is staged.
Prognosis for treatment for osteosarcoma
The prognosis for osteosarcoma can vary depending on the size of the tumor, the stage at which surgery was performed, the results of chemotherapy, and the age of the patient. With properly organized treatment and timely assistance, the survival rate is quite high - 70%.
The success of treatment depends on the quality of tumor resection and all detected metastases, as well as on the results of chemotherapy. In many clinics in Europe, care for patients with sarcomas is provided at a very high level, and similar conditions are organized in large oncology centers in Russia. A special role is given to primary diagnosis, since time is almost priceless for people with sarcomas.
Treatment of osteosarcoma
Over the past 30 years, significant advances have been made in the treatment of osteosarcoma. In the 60s, the only treatment method was amputation of the limb. Depending on the stage of the disease, patient survival for 2 years ranged from 5 to 20%. Since the introduction of effective chemotherapy, it has become possible to use it before and after surgery, and in some cases it was possible to avoid amputation of a limb.
Currently, the 5-year survival rate of patients with localized osteosarcoma exceeds 70%. The survival rate of patients with chemotherapy-sensitive tumors varies between 80-90%.
After examining the patient and clarifying the stage of osteosarcoma, a treatment plan is developed. It should be borne in mind that due to the rarity of osteosarcomas, treatment should be carried out only in specialized departments with sufficient experience.
Patients with localized but intractable osteosarcoma after chemotherapy generally have a poor prognosis. This category includes patients with osteosarcomas of the base of the skull, spine and pelvic bones.
Surgical treatment can consist of either removing the tumor and preserving the limb, or amputating the limb. Limb-sparing surgery can be performed in 50-80% of cases, although in some cases amputation must be resorted to later.
For some patients, amputation is the only type of possible surgery.
This applies to patients with extensive spread of the tumor into surrounding tissues, germination of blood vessels and nerves. After prosthetics, such patients are able to walk within 3-6 months after amputation.
Surgical removal of metastases is used in patients with damage to lung tissue. This takes into account the number, size and location of metastases, as well as the effectiveness of chemotherapy.
Chemotherapy refers to systemic treatments.
An antitumor drug introduced into the body enters the bloodstream and reaches tumor cells, destroying them. In most cases, osteosarcoma patients receive chemotherapy before or after surgery.
The following drugs are used: methotrexate in high doses in combination with leucovorin, which neutralizes the drug and prevents side effects, doxorubicin (Adriamycin), cisplatin, carboplatin, etoposide, ifosfamide, cyclophosphamide.
Chemotherapy leads to the destruction of tumor cells.
However, this also damages normal cells. The severity of side effects depends on the type of drug, dose and duration of use.
Temporary side effects include nausea, vomiting, deterioration or loss of appetite, hair loss, mouth ulcers, menstrual irregularities, hemorrhagic cystitis, impaired renal, liver and heart function. Damage to bone marrow cells may be accompanied by infections and bleeding.
In rare cases, chemotherapy increases the risk of developing second tumors, such as leukemia, but it should be kept in mind that the value of chemotherapy for osteosarcoma outweighs the risk of second tumors.
Radiation therapy
To treat patients with osteosarcoma, external irradiation using high-energy rays or particles is used.
However, this type of therapy has a limited role in osteogenic sarcoma. It can be effective in patients after incomplete tumor removal. In addition, radiation therapy is used to control pain and in patients if the tumor recurs (comes back) after surgery.
Ewing's sarcoma and PNET
Ewing sarcoma and peripheral primitive neuroectodermal tumors (PNET) belong to a large group of closely related tumors that grow in bones and soft tissues and are characterized by an unfavorable course.
This group of malignant neoplasms can affect patients of working age. According to long-term observations, the average age of patients does not exceed 25-30 years. Tumors of this type are most often diagnosed in childhood and adolescence, mainly in males. In 1921, Ewing's sarcoma was discovered by James Ewing, an American oncologist and pathologist.
Over many years of studying these oncological tumors, scientists have come to the conclusion that they are neurogenic in nature and must belong to the same family. Ewing's sarcoma and primitive neuroectodermal tumors have similar molecular genetic features. Neoplasms grow very quickly, are difficult to diagnose early, and almost always give metastases during the period of their detection. Because of this aggressive spread, they are considered the most dangerous tumors affecting the skeletal system.
But modern medicine has made a huge breakthrough in improving methods for diagnosing and treating cancer of this type. Patients with malignant bone tumors, if they seek professional help in a timely manner, today receive highly effective complex treatment that eliminates the pathological focus, metastases and prevents relapses of the disease.
Causes of development of bone PNET and Ewing's sarcoma
Despite the persistent research work carried out by scientists regarding a family of tumors similar to Ewing's sarcoma, the exact cause of the appearance of these tumors could not be determined. But today there are a number of predisposing factors to the development of these diseases:
- hereditary factor: it has been noted that people with gene mutations or cases of sarcomas in the family are more likely than others to suffer from PNET and Ewing's sarcoma;
- race: according to statistics, malignant bone tumors most often affect people of the Caucasian race, mainly males (boys suffer from Ewing's sarcoma twice as often as girls);
- benign bone tumors;
- young age (5-30 years);
- traumatic factor: a connection between bone injuries and the development of sarcomas can be traced, but it has not been confirmed;
- X-ray examination: X-ray diagnostics is the main method for detecting pathological foci in bone tissue;
- computed tomography, magnetic resonance imaging: allow you to determine the stage of development of sarcoma, the exact location of the tumor, the degree of damage to tissues and blood vessels;
- tumor histology: this method cannot be considered as the main one, since the results of a biopsy of other tumors may coincide with the results of a histological examination of Ewing’s sarcoma;
- laboratory tests: in the presence of sarcomas, pronounced leukocytosis, increased ESR and lactate dehydrogenase levels are observed;
- bone marrow biopsy;
- scintigraphy: the use of radiopharmaceuticals to detect bone pathologies;
- ultrasound diagnostics;
- molecular genetic diagnostics.
Diagnostics
If osteogenic sarcoma is suspected, a diagnostic search is carried out by specialists such as a pediatric oncologist, a pediatric surgeon, a pathologist, and a radiologist. The final diagnosis is established based on the results of histological examination.
At the first meeting with a young patient, the doctor collects an anamnesis, clarifies information about the presence or absence of any chronic diseases of the musculoskeletal system, previous injuries, surgical interventions, hereditary syndromes, and family hereditary oncological pathology. A clinical examination of the patient includes an assessment of the focus of the affected limb, regional lymph nodes, and physical status (general condition of the patient).
The diagnostic search consists of the following studies:
- radiography of the affected area;
- computed tomography (CT) with contrast enhancement of the tumor-affected area and chest organs;
- osteoscintigraphy;
- Magnetic resonance imaging of the affected area.
The most common and simplest method for diagnosing osteogenic sarcoma, which can be performed on an outpatient basis, is an x-ray examination of the affected limb. Situations cannot be excluded when the formation is an accidental finding during radiography performed for a traumatic injury. In such situations, the patient is indicated for further examination.
Characteristic radiological signs of osteogenic sarcoma (Fig. 2):
- destruction and sclerosis of bone tissue in the affected area;
- Codman's periosteal visor, which is the periosteum exfoliated by the tumor;
- needle periostitis with multiple bone spicules;
- foci of pathological bone formation in soft tissues (fields of ossification) in the area of formation;
- pathological fracture of the affected limb.
Rice. 2. Radiological signs of osteosarcoma
For clearer visualization of the process, clarification of the size of the formation, spread, and exclusion of soft tissue damage, children are advised to perform computed tomography. In addition, this method allows you to evaluate the primary tumor and detect the presence of distant metastatic foci.
Skeletal scintigraphy has long been the standard method for diagnosing bone lesions, being more sensitive than x-ray methods. It allows you to study the entire human body in a short period of time. This study is based on an increase in the accumulation of phosphorus compounds in the lesion, which indicates the activity of a process characteristic of malignant neoplasms (Fig. 3).
Fig.3. Pathological accumulation of radiopharmaceutical (Technetium mTc)
Magnetic resonance imaging (MRI) of the primary tumor lesion involving the adjacent joint is the optimal method for local staging. MRI monitoring against the background of systemic therapy makes it possible to assess the dynamics of the process and, accordingly, plan the scope of surgical intervention in the future.
One of the key stages of diagnosis is a biopsy of the formation and subsequent histological and immunohistochemical examination of the obtained material.
There are two different approaches to obtaining material: using a trephine needle and an open type of biopsy. The manipulation is performed under CT or ultrasound navigation or using an electron-optical converter (Fig. 4).
Fig. 4: Biopsy using a trephine needle
Methods for diagnosing Ewing's sarcoma and PNET
- FISH (fluorescent in situ hybridization) method: determination of translocation between certain chromosomes with identification of gene changes and synthesis of the EWS/FLI1 protein, which occurs only in patients with Ewing sarcoma;
— polymerase chain reaction (PCR): the method allows you to repeatedly copy a certain section of DNA, detecting the slightest changes in genes.
- angiography.
Diagnosing sarcoma can be quite difficult for a primary care doctor. In city clinics and provincial hospitals, this disease is often mistaken for a common inflammatory process, bruise or sprain, without prescribing an initial X-ray diagnosis. As a result of this, the treatment regimen chosen is completely incorrect, and some methods of therapy can even aggravate the patient’s condition and contribute to the progression of the disease.
Staging of osteosarcoma
Staging means determining the extent of the process.
In principle, osteosarcomas are divided into localized and metastatic .
With localized osteosarcoma, only the bone and adjacent tissues, including muscles, tendons, etc., are affected.
In the case of metastatic osteosarcoma, there is multiple damage to the bones and lungs (85%). In addition, the brain and other internal organs may be involved.
Patients with metastases have a worse prognosis than patients with localized disease. However, in the case of surgical removal of metastases and chemotherapy, the prognosis improves.
Clinical picture
Ewing's sarcoma and primitive neuroectodermal tumors can develop in any bone, affecting the surrounding soft tissue. Almost half of Ewing's sarcomas affect the lower extremities and pelvic region. Often the bones of the upper extremities are also involved in the pathological process. PNETs most often affect the bones and soft tissues of the chest, lungs, mediastinal organs and pleura.
The main sign of pathology is pain. At first, the pain is mild and may spontaneously weaken or even disappear for a while. But as the cancer process develops, the pain progresses and becomes more noticeable. All patients with bone sarcoma note swelling in the area of development of the tumor process. The swelling gradually affects the surrounding articular surfaces, causing impaired mobility of the joint and the limb as a whole.
During palpation, the area of edema is painful, characterized by severe hyperemia, an increase in the vascular pattern and pastosity, and is hot to the touch. There is a moderate increase in lymph nodes. If a tumor develops in the pelvic area, then dysfunction of the internal organs of this area may occur (fecal incontinence, urinary incontinence, paralysis). The pain tends to intensify at night, and often cannot be relieved by traditional methods. As tumor cells increase, the load on the bones increases, which can result in fractures.
Some patients at the time of diagnosis of the disease note signs of intoxication: patients complain of weakness, weight loss, and a slight increase in body temperature. Tumors of this family tend to metastasize very quickly to the lungs, bone marrow, and bones.
Many patients do not seek medical help when pain and swelling occur, as they attribute these symptoms to minor inflammation that develops after an injury or illness. Due to late diagnosis of the tumor, before effective treatment measures are taken, severe metastasis already develops, as a result of which treatment of Ewing sarcoma and PNET is often ineffective. It is extremely important to promptly contact doctors as soon as early signs of pathology appear.
Sarcomas should be treated only in specialized clinics that have modern diagnostic equipment and experience in managing patients with similar diseases. Modern medicine, alas, is imperfect, many doctors are incompetent, and delay in this case is simply unacceptable. Patients with sarcomas need treatment from real professionals.
The most important thing is diagnosis and timely treatment. Insist on being examined, even if the doctor does not see the need for it. The patient is an active participant in the treatment process. Many specialists have long recognized this fact and are successfully implementing it into their modern practice.
Treatment of osteogenic sarcoma in children
Treatment methods for osteosarcoma have remained virtually unchanged over the past 20 years. To date, the main methods of treatment remain polychemotherapy and surgery.
There are two options for surgical intervention:
- organ-preserving,
- organ-carrying (crippling).
In the absence of contraindications, in most cases organ-preserving treatment is performed to help the child preserve not only the functional abilities of the limb, but also to minimize cosmetic defects. For this purpose, all the achievements of modern medicine in bone grafting and reconstructive surgery are used.
Endoprosthetics
Endoprosthesis replacement is an option for organ-preserving intervention. This is an operation to replace a joint with implants that have the anatomical shape of a healthy joint and allow full range of motion. Total endoprosthesis replacement is more often used due to the impossibility of preserving the joint (Fig. 5).
Rice. 5. Total knee replacement consists of three components: femoral, tibial and patella
Arthrodesis
Other options for organ-preserving intervention include arthrodesis. This is a surgical procedure that fixes the joint in a permanent position. The bones are rigidly connected for complete immobilization and fastened with metal clamps (special screws, knitting needles, pins). This joint provides support and motor function.
Rice. 6. Arthrodesis
Exoprosthetics
In cases of large spread of the tumor to surrounding tissues, involvement of the neurovascular bundle in the process, or growth of the tumor mass during treatment, amputation/disarticulation is performed, followed by prosthetics with an exoprosthesis (Fig. 7, 8, 9). Considering the quality of modern exoprostheses and the development of medical rehabilitation, it is possible to fully preserve functionality even with such organ-removing treatment. Rehabilitation aims not only to restore functional abilities, but also to help the child cope with the social and emotional consequences of limb loss.
Fig.7 Exoprosthesis of the upper limbs
Rice. 8 Exoprosthesis of the lower extremities
Fig.9 Exoprosthetics of the lower limb
Rotational plastic
Rotation plasty is a treatment method that is the method of choice in relation to mutilating amputation/disarticulation operations. The principle is resection of the affected part of the femur and rotation of the tibia by 180°. In this case, the ankle joint takes on the function of the “knee joint” (Fig. 10). The indication for this type of intervention is a tumor in the distal part of the femur with a pronounced soft tissue component, when the surrounding soft tissue is involved in the tumor process and organ-preserving surgery is impossible. In this case, a necessary condition for the operation is the preservation of the sciatic nerve.
Fig. 10 Rotational plastic
Methods for effective treatment of Ewing's sarcoma and neuroectodermal bone tumors
In recent years, methods of treating oncological lesions of the skeletal system have significantly improved, which has a positive effect on the life expectancy of patients and the prognosis of the course of these pathologies. Treatment should be comprehensive, affecting both the tumor itself and the entire body - with the goal of destroying all areas with metastases.
Treatment methods include the following:
- Surgical removal of the pathological focus. During the operation, the femur, pelvic bones, and ribs may be partially removed. The scale of resection depends on the extent of the pathological process. Endoprostheses can be placed in place of the removed bone areas. Today, all surgeons in the world try not to carry out radical interventions that end in limb amputation and disability.
- Radiation therapy. Radiation exposure is carried out repeatedly: before surgery and after surgery. High-quality radiation therapy can effectively combat metastases and prevent relapses of the disease. The radiation dose is selected individually. One course of radiation treatment usually lasts 4-6 weeks.
- Chemotherapy. The introduction of certain chemotherapy drugs into the body (cyclophosphamide, adriamycin, vincristine) helps destroy the smallest metastases, which are very common in sarcoma. Diagnosing them can be difficult, and chemotherapy affects all human organs and tissues, making it possible to fight micrometastasis and slow down tumor growth. Cytostatics are prescribed in courses with breaks of 2-3 weeks between them. If metastases are detected in the bone marrow, the use of large doses of chemotherapy drugs with a stem cell transplant is indicated.
Survival Prognosis for Patients
The prognosis for Ewing's sarcoma and neuroectodermal neoplasms is quite unfavorable. The outcome of treatment depends on the stage of the disease at which the patient seeks medical help and the degree of spread of the tumor process. Patients with metastases in the lungs have a better chance of recovery than patients with evidence of metastases in the bone marrow or bones. If the tumor is detected in a timely manner, when it has not yet had time to disseminate, then the chances of a complete recovery are quite high - up to 70%.
Modern chemotherapy drugs do not have as severe side effects as before. During chemotherapy and radiation treatment, most complications can be avoided. But the success of therapy also depends on the patient himself. It is very important for the patient to understand that sarcoma is not a death sentence. The capabilities of modern medicine make it possible today to overcome almost any disease. If you do not create obstacles to treatment, follow all medical recommendations, look for the best doctors and believe in your own recovery, then the disease will recede.
Time is very important. If even the slightest signs of illness appear, it is necessary to carry out a diagnosis. Having discovered a tumor, doctors will do everything possible to destroy the pathological process. The patient needs to mobilize, tune in to long-term treatment, accept the support of his family and think only about the best.
How to treat osteosarcoma
The therapeutic approach is based on the localization of the formation, its stage, relapses and other information. In general, treatment of osteosarcoma in adults is carried out in the following sequence:
- Preoperative chemotherapy aimed at suppressing micrometastases in the lung tissue. Thanks to it, it is possible to reduce the size of the tumor. During chemotherapy, the patient may be prescribed the following drugs: high-dose Methotrexate, Ifosfamide, Adriablastin, Etoposide, Carboplatin, Cisplatin.
- Excision of the tumor, which often saves most of the bone. Previously, doctors resorted to extensive surgery, during which the patient’s limb affected by the tumor was often amputated. Modern methods of therapy allow for gentle excision of the tumor, in which only part of the bone is removed. The removed area is replaced with a plastic or metal implant.
- Postoperative chemotherapy, taking into account the results of preoperative chemotherapy.
In some particularly severe cases, when the tumor grows into the neurovascular bundle, a pathological fracture occurs, or the tumor is very large, doctors have to remove the affected limb. Modern treatment methods make it possible to save organs even in the presence of large metastases, for example, to the lungs. They are simply removed surgically. In cases where surgery is not possible for any reason, the patient may be prescribed radiation therapy.
The use of modern approaches to the treatment of osteosarcoma, including various types of chemotherapy and surgery, allows us to achieve very good results. Thanks to this, the survival rate of patients with this diagnosis is only increasing every year.
Chondrosarcoma
Chondrosarcoma is a type of malignant tumor that affects cartilage tissue. The disease is quite common, accounting for up to 10-15% of all bone tumors. It is diagnosed in people of all ages, but more than 60% of patients belong to the mature age group (after 40 years). In 15% of patients with chondrosarcomas, the tumor develops secondarily from osteochondral exostoses, chondromas, and deforming osteosis.
It has been noted that chondrosarcoma most often affects the bones of the pelvis, upper limbs and ribs. Men get sick slightly more often than women. The etiology of the disease is not completely clear. Predisposing factors include gene mutations, the presence of certain hereditary pathologies, and carcinogenic effects on the human body.
Causes
The etiological aspects of the formation of osteosarcoma of bones have not yet been fully studied, although there are several factors that contribute to their occurrence.
Osteosarcoma can develop in bones that have previously been exposed to ionizing radiation during treatment for malignant or benign tumors. Radiation-induced bone disease usually manifests itself three years after the end of irradiation, in the form of osteosarcoma. Some role in the causes of certain cases of malignant tumors is assigned to carcinogenic ankylating agents and anthracyclines. In addition, since osteosarcoma develops in those bones that grow relatively quickly and are exposed to physical stress, a certain role of these loads as a putative factor in the formation of osteosarcoma cannot be ruled out.
Sometimes the history of patients with osteosarcoma reveals existing injuries. However, they are not currently considered a direct cause in the development of this disease. Although there are suggestions that they provoke an anomaly, the cells of which are already present in the body.
It is also believed that many pathologies, such as fibrous degeneration, chondromas, deforming osteosis, and osteochondral exostoses can transform into osteosarcoma.
Signs of chondrosarcoma
Chondrosarcoma is characterized by an asymptomatic gradual course. At the initial stage of development, there are no pathological signs. As the tumor grows, pain begins to occur in the area where the chondrosarcoma is located. If it is located near the joint, then in the clinical picture of the disease there are signs of limited movement.
If the tumor begins to compress the sciatic nerve (if localized in the thigh area), then the pain changes from minor to unbearable. The skin above the tumor becomes swollen; the tumor itself, which has reached a significant size, can be easily palpated. In 15% of patients, fast-growing chondrosarcomas are found, prone to accelerated growth and rapid malignancy.
Disease of the young
Like many cancers, osteosarcoma begins gradually. Initially, a person is bothered by itchy, vague pain that occurs near the joint, to which the patients themselves, and in some cases doctors, do not attach much importance.
The sad truth is often revealed too late, when the parts of the bone tissue affected by the tumor increase in volume, and the pain becomes sharp and unbearable (especially at night).
The low oncological alertness towards osteosarcoma can be partly explained by the relative rarity of this disease, which occurs in 1 in 100 thousand adults and in 5-6 out of 100 thousand children, mainly in adolescents 14-15 years old, which many experts associate with rapid growth and hormonal changes in the body.
Article on the topic
Heredity and stress. What do you need to know to save yourself from cancer?
Methods for diagnosing chondrosarcoma
The capabilities of modern medicine make it possible to detect bone tumors already at the initial stage of development. But since chondrosarcoma is rarely detected at an early stage of growth, diagnosis can be delayed. Many patients and doctors mistake pain, inflammation and other early signs of the disease for arthrosis, bursitis, injuries and are in no hurry to conduct a detailed examination. And the outcome of treatment and the further prognosis of the disease largely depend on the timeliness of diagnosis.
Among the modern and popular diagnostic methods for chondrosarcoma are the following:
- X-ray examination: the images reveal foci of destruction with areas of calcification, the tumor itself and signs of its growth into soft tissues;
- osteoscintigraphy;
- magnetic resonance, computed tomography;
- biopsy of tumor tissue with further study under a microscope.
Patients with chondrosarcomas should be examined in large diagnostic centers that have modern technical equipment and a professional staff of specialists who know the technique of decoding the diagnostic results obtained.
Central chondrosarcomas often have intraosseous areas of destruction. On x-rays, characteristic calcifications are diagnosed with such neoplasms. Areas of calcification are often diagnosed along the edges of the neoplasm.
Diagnosis of the disease
Due to the similarity of the symptoms of a tumor with inflammatory processes, in some cases an incorrect diagnosis is made, and, consequently, the wrong treatment is prescribed. Diagnosis of osteosarcoma relies on radiological findings in conjunction with histopathological criteria.
This is done using the following methods:
- X-ray examination. Gives an extremely diverse idea of the location and development of the tumor. Shows changes in bones and their elements. A characteristic sign by which, during X-ray examination, one can judge the development of osteosarcoma is the “Codman triangle”. This is a kind of triangular spur or “visor”. To these can be added needle-like spicules, which also indicate the development of pathology.
- CT scan. Helps determine the exact location of the tumor, find out its size and distribution. If radiology reveals only macrometastases throughout the body, then here they can be examined in more detail - at the level of micrometastases.
- Morphological examination. A biopsy that involves local spread of tumor cells often makes organ-sparing surgery impossible. Because of this, a biopsy should be performed by a surgeon, or even better, a trepanobiopsy. It is better than a knife biopsy in that it protects the tissue near the tumor.
- Angiography. Performed immediately before the start of the operation. Using this method, it is determined how strongly the tumor affects the vessels and whether they are free from it. This affects the overall volume of the operation. If tumor emboli have leaked into the vessels, then it will not be possible to save the organs during the operation.
- Osteoscintigraphy. It also helps to detect foci of inflammation located in the bones. The content of the isotope used in this procedure is analyzed before and after completion of chemotherapy, which allows us to judge its effectiveness. If much smaller accumulations of the isotope are found in the tumor, this indicates a positive histological response of the pathology to chemotherapy treatment.
- Magnetic resonance imaging. The method is the most accurate, since it shows the relationship of the tumor to the surrounding tissues, and with chemotherapy, the effectiveness of the treatment process and the development of events during the operation are visible. MRI is performed using a special substance that accumulates along the perimeter and area of the tumor - gadolinium, which indicates its location. For MRI, modern clinics use a new method called DEMRI. It consists of capturing the contrast agent introduced during MRI. Then, using special equipment, the presence of oncology cells is determined in percentage terms before the start of chemotherapy, and after, thereby determining the histological response of the tumor to therapy even before the start of surgery.
A general blood test is also mandatory; based on its results, you can find out about osteosarcoma. This will be indicated by a high level of alkaline phosphatase and ESR, and in half of the cases – leukocytosis. Anemia is noted, which continues to progress in the final stages.
Treatment options for chondrosarcomas
In the early stages of tumor development, radiation treatment with surgical excision of chondrosarcoma is used. If the disease has a high risk of malignancy, then minimally invasive operations have to be abandoned and complete amputation must be performed. Partial bone removal with subsequent plastic surgery is appropriate only if long-term tumors that are not prone to malignancy and metastasis are detected.
Chondrosarcoma cells are quite resistant to radiation exposure (especially at later stages of development) and chemotherapy. Therefore, these methods are perceived not as the main ones, but as auxiliary methods for the treatment of chondrosarcomas. The main emphasis is on complete surgical excision of the pathological focus and metastases. When a tumor grows in the pelvic bones and humerus, it is sometimes necessary to perform extensive surgery to remove half of the pelvis and amputate the entire upper limb. But in any case, doctors try to perform organ-preserving operations if the situation and clinical picture allow it.
Forecast
The prognosis for recovery of patients with chondrosarcomas is quite favorable. It directly depends on the timeliness of treatment, the degree of malignancy of the tumor and the quality of the operation performed. Treatment of chondrosarcomas requires considerable professionalism from doctors. Therefore, when choosing a clinic, you should give preference to specialized institutions with considerable experience in treating bone tumors and an individual approach to each individual patient.
After successful surgical intervention, more than 25% of patients live for 5 years or more. To prevent recurrence of the pathology, such patients are recommended to undergo regular diagnostics and preventive examinations.