The outer ear is formed by the pinna and the external auditory canal.
Author:
- Oganesyan Tigran Sergeevich
ENT pathology expert
(Voted by: )
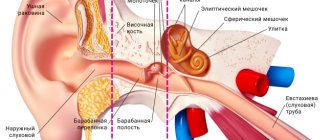
- Outer ear
- Middle ear
- Inner ear
The outer ear is the visible part of the hearing system, formed by the auricle and the external auditory canal. The basis of the auricle is elastic cartilage, covered with skin on both sides.
The lobe is a concentration of fatty tissue. The external auditory canal has several parts - the tragus, the deep notch and the antihelix. Its length usually does not exceed 2.5 cm, two-thirds of which is occupied by the membranous-cartilaginous section. The remaining part is the bony section that serves as the boundary between the outer and middle ear.
The main function of the auditory analyzer is sound transmission and sound perception. In this regard, the auricle directs sound vibrations to the external auditory canal, which acts as a conductor of sound waves to the eardrum. Moreover, it is in this part that selective amplification of sound occurs. Any reduction in the lumen leads to hearing loss.
Embryology
The outer ear begins to form in the embryo at the end of the 1st month. from the elements of the first (maxillary) and second (hyoid) arches and the first pharyngeal groove. In an embryo measuring 12 mm, three tubercles appear at the dorsal ends of these arches, more pronounced on the hyoid arch. In an embryo measuring 18 mm, the tubercles of the jaw arch merge into a single thickening, from which the tragus develops. By fusion of the more developed tubercles of the hyoid arch, the rest of the auricle is formed, with the exception of the tragus. Most of the external auditory canal is formed from the first pharyngeal groove; by the end of the 2nd month. During embryogenesis, the ectoderm of the bottom of the first pharyngeal groove grows into the location of the future tympanic cavity, separated from it by a layer of compacted mesoderm (with the handle of the malleus developing in it), lined internally with endoderm and externally with ectoderm.
Anatomy
Rice.
1. General view of the auricle (lateral surface): 1 - triangular fossa, 2 - tubercle of the auricle, 3 - scaphoid, 4 - crus of the helix, 5 - cavity of the auricle, 6 - antihelix, 7 - helix, 8 - antitragus, 9 - auricular lobule, 10 - intertragus notch, 11 - tragus, 12 - supratragus tubercle, 13 - helical-tragus groove, 14 - antihelix legs. The auricle (auricula) forms an angle of approx. 30° with the side surface of the head; on its lateral surface there are elevations and depressions (Fig. 1). The most pronounced depression is the conch of the ear (concha auriculae), the edges are divided by a protrusion - the helical leg (crus helicis) into upper and lower parts; the latter directly continues into the external auditory canal. The helix (helix), forming a thickening of the free edge of the auricle, borders it in front, above and behind. Near the transition of the upper part of the curl to the descending part, a tubercle (tuberculum auriculae) stands out. Anterior to the descending segment of the helix, a second elevation is noticeable - the antihelix (anthelix), from which the diverging legs (crura anthelicis) continue upward, limiting the triangular fossa (fossa triangularis). The helix is separated from the antihelix by a longitudinal groove - the scapha.
In front, the concha of the ear is covered by a tongue-like protrusion - the tragus; slightly lower and posteriorly the antitragus stands out, separated from the tragus by the intertragus notch (incisura intertragica). Below the notch is the earlobe, or ear lobe (lobulus auriculae), the edges do not have a cartilaginous base. Elevations on the medial surface of the auricle correspond to depressions on the lateral surface. The auricle has gender, age and individual characteristics: in women it is thinner and smaller in size than in men; in a newborn it is 1/3 the size of an adult’s ear; in old age it becomes wider and longer.
The muscles of the auricle in humans are poorly developed and have no functional significance.
Rice. 2. External auditory canal (frontal section): 1 - cartilaginous part, 2 - bone part.
The cavity of the auricle, deepening like a funnel, passes into the external auditory canal (meatus acusticus ext.), ending with the eardrum. The length of the ear canal in an adult is on average 24 mm, dia. 7 mm. According to the oblique position of the eardrum, the anterior and lower walls of the external auditory canal are longer than the upper and posterior ones. The external auditory canal (Fig. 2) consists of a lateral (cartilaginous) part, 8 mm long, and a medial (bone) part, 16 mm long. The external auditory canal is tortuous and can be divided into three segments: lateral, intermediate and medial. The lateral segment has a bend, the convexity is directed forward and slightly upward, the convexity of the bend of the intermediate segment is directed backward, the medial segment is directed forward and slightly downward. In a cross-section, the external auditory canal has the shape of an ellipse with the largest diameter in the direction from top to bottom and posteriorly. Starting from the auricle, the external auditory canal gradually narrows to the medial end of the cartilaginous part; at the beginning of the bony part it widens, and then narrows again at its medial end.
The narrowest segment of the external auditory canal, called the isthmus, is located at a distance of 20 mm from the bottom of the concha; the medial end, which has a rounded shape, is closed by the tympanic membrane (see).
In the anteroinferior wall of the cartilaginous part of the external auditory canal there are fissures (Santorini fissures) made of fibrous connective tissue. Thanks to the presence of gaps, greater mobility of the external auditory canal and auricle is created. Through these gaps, the inflammatory process can spread from the external auditory canal to the parotid gland and vice versa. The external auditory canal is widest when the mouth is opened. Most of the head of the lower jaw lies in front of the bony part of the external auditory canal, only a small part of it borders on the cartilaginous part, to which the parotid gland is directly adjacent; posterior to the bony part of the external auditory canal are the air cells of the mastoid process of the temporal bone.
Blood supply
The external ear is carried out by the branches of the superficial temporal (a. temporalis superficialis) and posterior auricular (a. auricularis post.) arteries; the veins flow into the posterior auricular and maxillary veins (v. auricularis post, and v. retromandibularis). Lymph flows to the anterior and posterior ear nodes (nodi lymphatici auriculares ant. et post.). Motor innervation of the muscles of the auricle is carried out by branches of the facial nerve. The auricle is supplied with sensory nerves by the auriculotemporal and greater auricular nerves (n. auriculotemporalis and n. auricularis magnus); Sensitive branches to the skin of the external auditory canal give off the vagus and auriculotemporal nerves.
Histology
The base of the auricle is formed by elastic cartilage, rich in cells; the skin of the auricle is thin, smooth, with a poorly developed layer of epidermis and unevenly expressed papillae, on the lateral surface tightly fused with the underlying perichondrium. Continuing deeper, the skin lines the walls of the external auditory canal in the form of a tube.
It is up to 2 mm thick in the initial part of the ear canal and becomes thinner in its depth.
On the medial surface of the auricle, the skin is mobile due to a well-developed subcutaneous base. In the area of the concha and triangular fossa, the skin contains the largest number of sebaceous glands; sweat glands are concentrated on the medial surface. In the area of the tragus, antitragus and intertragal notch there are hairs, sometimes (in older men) quite long.
The skin lining the cartilaginous part of the external auditory canal is equipped with sebaceous and ceruminal glands that secrete earwax. In the bony part of the ear canal, the skin is thinned and devoid of hairs and glands.
Physiology
The auricle performs two functions - capturing sound waves and protecting. Compared to the auricle of animals, the human auricle performs the first function poorly. A person cannot turn it towards the sound source, as some animals do (dogs, horses, etc.) - The protective function of the auricle is due to the fact that its peculiar configuration prevents dust from entering the external auditory canal and further to the eardrum. The natural lubricant of the external auditory canal is earwax, which is secreted in small quantities under normal conditions. Wax is removed from the external auditory canal due to the movements of the lower jaw; Small foreign bodies and dust particles stuck to it are removed along with earwax.
The auricle is a reflexogenic zone (see), which has long been used for acupuncture (see).
Bestsellers!
Hearing aid Aurica Pixel 440CIC
Digital hearing aid of the bronze category for those who lead an active lifestyle and continue to work: home, telephone, conversation, TV, store, playground, street, work. Ideal for mild hearing loss. Find out more >>>
Hearing aid Microtech Focus 30 BTE
A gold category hearing aid is an ideal solution for people who value the taste of life (noisy parties, travel, street, work, playground, home, telephone, conversation, TV, store). Ideal for all degrees of hearing loss. Ideal for all degrees of hearing loss. Find out more >>>
Hearing aid Microtech Thrive w30 BTE
A gold category hearing aid is an ideal solution for people who value the taste of life (noisy parties, travel, street, work, playground, home, telephone, conversation, TV, store). Ideal for all degrees of hearing loss. Find out more >>>
All hearing aids
Research methods
The lateral and inner surfaces of the auricle are examined by inspection. Pulling the auricle upward and backward (in adults) and posteriorly and downward (in infants), the cartilaginous part of the external auditory canal is examined, then an otoscopy is performed using an ear funnel (see). If pain occurs when palpating the tragus area, this indicates inflammation in the external auditory canal. For special indications, in some cases, rentgenol is also used. methods, in particular Fistulography (see).
Possible complications of otitis externa
As a rule, otitis externa does not cause complications and is easily treated. However, if complications do occur, they may include the following:
- temporary hearing loss in the affected ear. Goes away after recovery from otitis media;
- chronic external otitis. It usually occurs when there are difficulties in treating external otitis, for example, in fungal and mixed bacterial-fungal forms;
- spread of infection to deep tissues - cellulitis of the neck, lymphadenitis, osteomyelitis. Similar complications (malignant otitis media) can occur in patients with immunodeficiency conditions, diabetes, and those receiving chemotherapy. Such complications can be life-threatening.
Pathology
Developmental defects
Rice.
3. Malformations of the external ear: 1 - macrotia on the left; 2 - microtia on the right. There may be a complete absence of the auricle - anotia. Excessively large ears are also observed - macrotia (Fig. 3, 1) or too small - microtia (Fig. 3, 2). There are various deformities of the auricle: a pointed auricle (satyr's ear), an angular auricle (macaque ear), an ear with a large antihelix (Wildermuth's ear), etc. In the area of the tragus there may also be appendages, or appendages, of the auricles, which usually consist of skin and subcutaneous tissue, but sometimes also of cartilage.
Often, a congenital preauricular fistula (fistula) is found somewhat anterior to the peduncle of the helix - a trace of non-closure of the first branchial cleft. Congenital cysts can form in this same place.
Developmental defects such as the complete absence of the external auditory canal or an unusually sharp narrowing of its lumen are also possible. This pathology is often combined with malformations of the auricle.
Treatment of developmental defects is surgical. The pendants are excised along with the cartilage. It must be remembered that the fistula tract has a very narrow lumen, as a result of which it cannot be completely identified during fistulography. Most often it ends at the surface of the scales of the temporal bone. Excision of the fistula must be carried out along its entire length. With incomplete removal, relapses are usually observed. A number of operations are performed to restore the external auditory canal.
Damage
Bruises, cut wounds of the auricle, bites, etc. are observed. During the war, gunshot wounds of the auricle and external auditory canal predominated. Such injuries were most often combined with violations of the integrity of the tissues surrounding the ear. The consequences of these injuries can be divided into three groups: deformation of the auricle, narrowing or fusion of the external auditory canal, and combinations of these injuries. Treatment: plastic surgery.
Diseases
Sulfur plug
. Earwax, produced by special glands of the external auditory canal, is a natural lubricant of its walls, the edges are constantly removed. Normally, it is released in small quantities. But in some cases, earwax acquires a denser consistency and accumulates in the external auditory canal in the form of sometimes a very dense mass that gradually fills its lumen. As long as there remains at least a small gap between the cerumen mass and the wall of the external auditory canal, hearing is usually not severely impaired. When water gets into the ear, earwax swells and complete obstruction of the external auditory canal can occur with a significant decrease in hearing due to damage to the sound-conducting apparatus. The pathological accumulation of earwax in the external auditory canal is called “cerumen plug”.
In most cases, wax plugs can be removed by rinsing the external auditory canal with 2% sodium bicarbonate solution using a 100-200 ml syringe. The auricle is pulled upward and backward, and the stream of flushing liquid, heated to t° 37°, is directed to the superoposterior wall of the external auditory canal (see Ear rinsing). In some cases, the cerumen plug can be very dense, then the patient is prescribed instillation of 2% sodium bicarbonate solution or hydrogen peroxide into the ear for 3-4 days several times a day. These solutions soften the sulfur plug, and removing it by washing is not difficult. Cases have been described in which cerumen plug was the cause of vestibular disorders.
Inflammatory diseases
the external auditory canal (otitis externa) and the auricle are limited (boils) and diffuse.
Boils are observed only in the cartilaginous part of the external auditory canal. Characteristic symptoms: pain when chewing and pressure on the tragus, sometimes decreased hearing (usually with multiple boils, which is noted with general furunculosis), narrowing of the lumen of the external auditory canal.
Treatment: antibiotics corresponding to the suspected or identified pathogen, sulfonamide drugs, as well as sulfur preparations (Sulfur depuratum) but 0.5 g 3 times a day; Turundas with 3% boric solution in 70% alcohol are injected into the external auditory canal, and then 1% yellow or 3% white sedimentary mercury ointment is applied. It is necessary to prevent contamination of the skin of the external auditory canal with pus secreted from the boil to prevent the occurrence of new boils. Sometimes diffuse inflammation of the skin of the external auditory canal and auricle occurs. Skin eczema is also observed.
Diffuse skin inflammation
Well. in some cases it is caused by mycelium of fungi (see Otomycosis). The main symptoms: discharge of purulent secretion from the external auditory canal, itching in it, sometimes decreased hearing, concentric narrowing of the lumen of the auditory canal. If purulent discharge reaches the eardrum, then it is also involved in the process. In these cases, otoscopy reveals redness and infiltration of the tympanic membrane; its characteristic morphological signs are difficult to determine.
Treatment: thoroughly clean the walls of the external auditory canal with alcohol, potassium permanganate solution, furatsilin, and then lubricate with 2-3% silver nitrate solution, Lassar paste, 1% salicylic paste, etc.
Perichondritis
external ear infection develops when infection penetrates into the perichondrium of the auricle. Moreover, the skin of the Outer Ear is involved in the process. It is characterized by severe pain in the ear area, hyperemia and swelling, and increased temperature. In the case of a mild course, the process ends at this stage; in a severe course, suppuration occurs. Purulent exudate accumulates between the perichondrium and cartilage, and purulent melting of the cartilage occurs. The skin wrinkles, the auricle becomes deformed.
Treatment: at the beginning of the disease, warm compresses, antibiotics, and UHF therapy are used. When suppuration occurs, a wide incision is made along the edge of the auricle and all necrotic areas of cartilage are removed. Antibiotics are injected into the wound. If the auricle is deformed, plastic surgery is indicated.
Lupus
outer ear is most often the result of a process spreading from the face. Nodules appear, sometimes with ulceration of the skin in the area of the auricle, most often the earlobe; tuberculous perichondritis is possible. The diagnosis is made based on the presence of other tuberculosis lesions and biopsy results. For treatment, specific anti-tuberculosis drugs are used - see Skin tuberculosis.
Syphilis
external ear is usually observed in the second stage of the disease, less often in the third. It manifests itself in the form of a secondary syphilitic rash, syphilitic (gummy) chondritis. The diagnosis is made on the basis of other manifestations of syphilis, medical history, course of the disease, and serological test data. Treatment is carried out with specific means - see Syphilis.
Ear pain in a healthy person
Unpleasant sensations in the organ of hearing can occur in a completely healthy person, and there are many reasons for this (we will look at some in more detail):
- sensitivity to strong wind and cold (Due to a long stay in the wind, a hematoma may form in the ear - it will go away on its own in a few days. No additional measures need to be taken in this situation.);
- water getting into the ear;
- presence of sulfur plug;
- mechanical injuries (if, in addition to pain, bleeding from the ear begins, consult a doctor immediately);
- acoustic injuries (occur due to exposure to loud sounds on the organ of hearing, for example, at a rock concert, in a noisy industry, or during prolonged use of headphones. As a rule, the pain goes away when moving away from the source of noise. If, due to the nature of the work, it is impossible to eliminate the source of noise, You definitely need to use special earplugs.);
- barotrauma (manifested by changes in atmospheric pressure; most often occur during air travel or diving. When your ears are blocked on an airplane, you need to yawn more often, swallow, or simply chew something to eliminate the condition of “stuffiness”);
- foreign body.