Anatomical structure
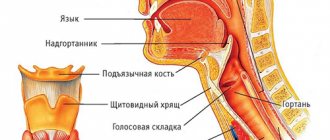
To understand the functions of the larynx, it is necessary to clearly understand its anatomical structure.
Cartilage
The components of the organ in question are paired cartilages:
- thyroid,
- ring,
- epiglottis.
Among the unpaired cartilages the following stand out:
- arytenoid,
- cricoid.
The cartilages presented above are interconnected by ligaments and joints, due to which they can move, facilitated by the muscles of the larynx.
The cricoid cartilage looks like a ring, its ring looks forward, the “stone” looks back. Next, the thyroid and arytenoids are attached. The largest is the thyroid. It forms walls. Their parts are plates that stand at an obtuse angle in women, and at an acute angle in men (due to which the “Adam’s apple” protrudes).
The arytenoid cartilages are a pyramid, the base of which is attached to the cricoid cartilage. Two types of processes extend from the arytenoids:
- muscular,
- voice.
The muscular process controls the arytenoid cartilage, causing the vocal process to change position and influence the attached vocal cord.
- What is the human pharynx and oropharynx: structure, functions
All of the listed cartilages are hyaline, that is, they have the following characteristics:
- density,
- glassiness,
- elasticity.
They show a tendency to ossify. Ossification can occur as an age-related change, which affects the timbre of the voice.
Epiglottis
This part is a kind of “lifting shield” above the entrance of the laryngeal opening. From below, the epiglottis adjoins the thyroid cartilage. The main function representing the operation of this part of the system under consideration is to protect the respiratory entrance from foreign particles entering the lungs by closing its entrance.
Vocal cords
The ligaments are the primary mechanics that produce sound, traveling from the vocal processes to the thyroid cartilage. Between their pair there is a gap that allows a stream of air to pass through when a person breathes.
Laryngeal muscles
The muscles of this system are divided into large groups:
- internal, whose role is to guide the vocal cords,
- external, controlling the movements of the pharynx.
Intrinsic muscles exhibit a special distribution pattern:
- sound laryngeal, that is, the main adductors, there are only three of them,
- abductor - one muscle,
- cricothyroid muscle, which controls the tension of the ligaments.
Each type of muscle listed above performs a number of functions:
- the abductor expands the glottis, if it is damaged, this threatens the loss of speech abilities,
- adductors are responsible for narrowing the glottis, paired and unpaired types of muscles work simultaneously,
- The cricothyroid muscle controls the thyroid cartilage upward and forward, exerting proper tension on the ligaments.
The extrinsic muscles of the larynx are classified as:
- sternothyroid,
- thyrohyoid,
- thyroid.
The coordinated work of these muscles makes it possible to carry out movements of the pharynx during swallowing, breathing, and speech production.
- Cricoid unpaired cartilage of the larynx: its structure and functions
The main function of muscles is to change the position of the cartilage of the organ. The muscles of the larynx, according to the nature of their action on the glottis, are divided as follows:
- expanding,
- narrowing,
- changing the tension of the ligaments.
Thanks to the work of the muscles, the entire work of the system in question is carried out. Without them, breathing, respiratory protection, and speech production are impossible.
Laryngeal cavity
The cavity has an hourglass shape. The middle part, which is greatly narrowed, contains folds of the vestibule, or the so-called false vocal folds. The vocal cords are located below. On the sides are the ventricles, which are atavistic in nature. In some animals, such bags are very developed and serve as resonators.
The entire cavity, except for the ligaments, is lined with a mucous membrane consisting of ciliated epithelium, which reacts to the slightest touch thanks to a huge number of glands that cause a cough reflex when the mucosa is irritated by any foreign object. The mucous membrane covers the fibro-elastic membrane.
Pain in the larynx
General information
The larynx is the upper part of the respiratory tract and also the organ of voice production. It is located at the level of the III-VI cervical vertebrae (slightly higher in children), opens from above into the pharynx, and below passes into the trachea. The skeleton of the larynx is formed by cartilages:
unpaired (cricoid, thyroid, epiglottis);
paired (arytenoid, corniculate, wedge-shaped)
They are connected to each other by joints and ligaments. The hypoglossoid membrane connects the larynx to the hyoid bone. Between the thyroid and cricoid cartilages is the cricothyroid ligament. It is sometimes resorted to dissection in case of acute laryngostenosis.
On the inner surface of the larynx there are vocal folds, the basis of which are paired vocal cords and vocal muscles. Above them are the vestibular folds, their basis is made up of the ligaments of the vestibule. Between the vestibular and vocal folds on each side are the ventricles of the larynx .
The space between the vocal folds is called the glottis. There are three sections in the laryngeal cavity: the upper, or vestibule (above the vestibular folds), the lower (under the vocal folds) and the middle, narrowest, located between the vestibular and vocal folds. The mucous membrane of the larynx is covered with columnar ciliated epithelium. On the vocal folds and upper parts of the epiglottis, the epithelium is multilayered squamous. The submucosal layer of the lower part of the larynx is loose, prone to swelling, especially in childhood. The larynx performs a respiratory, protective (spasm of the larynx and cough when a foreign body enters it or the presence of harmful impurities in the air) and voice-forming functions.
Pain in the larynx due to illness
With bruises, compression, cartilage fractures , or separation of the larynx from the trachea, shock may occur. Other signs of damage are expressed by the following characteristic symptoms:
- hemoptysis;
- pain in the larynx when swallowing and coughing;
- labored breathing.
On palpation , crepitus of the subcutaneous tissue (subcutaneous emphysema) and crunching of broken cartilages are noted. The victim may be at risk of suffocation caused by displacement, laryngeal edema and mediastinal emphysema. Poisoning with acids and caustic alkalis (acetic essence, soldering liquid, bath washing liquid, carbolic, oxalic acid, caustic soda, ammonia). Signs of poisoning are burns of the lips, oral mucosa, as well as:
- pain in the larynx;
- copious amounts of saliva;
- bloody vomiting.
The most common inflammatory diseases of the larynx are acute and chronic laryngitis. Less commonly, abscess, phlegmon, chondroperichondritis, diphtheria, tuberculosis and syphilis of the larynx develop. An abscess occurs as a result of the introduction of infectious agents during injury to the mucous membrane of the larynx. The disease initially occurs as a common sore throat, followed by hoarseness and difficulty breathing. Phlegmon of the larynx occurs with the following symptoms:
- high body temperature;
- chills;
- difficulty breathing;
- sharp pain in the larynx when swallowing,
Against this background, and also as a complication of influenza , chondroperichondritis of the larynx can occur, in which the inflammatory process spreads to the hyaline cartilages of the larynx, causing them to suppurate and melt with the formation of fistulas and sequestration. Diphtheria of the larynx (diphtheria croup) occurs more often in children. Due to the formation of fibrinous exudate in the area of the vocal cords and under them, increasing stridor, laryngostenosis develop, and pain in the larynx . Severe intoxication is noted. Laryngeal tuberculosis is often a complication of pulmonary tuberculosis. Patients' complaints of a sore throat, pain in the larynx, and hoarseness depend on the stage, location, extent and form of the process. When diagnosing, one should take into account the medical history, complaints, general condition of the patient, laboratory data (detection of Mycobacterium tuberculosis in sputum, results of tuberculin tests). A patient with suspected laryngeal tuberculosis should be referred to a phthisiatrician or otolaryngologist. Of the benign tumors, the most common are fibromas and papillomas . Angiomas and lymphangiomas are rarely observed. The main symptom of benign tumors of the larynx is hoarseness and pain in the larynx. To establish a diagnosis in all cases, a histological examination of the material obtained from a tumor biopsy is necessary.
Laryngeal cancer
Laryngeal cancer occurs predominantly in men, usually over the age of 40. Precancerous diseases of the larynx can be:
- leukoplakia;
- papillomas;
- keloid scars.
With cancer of the upper part (vestibule) of the larynx, there is soreness, a sensation of a foreign body, and pain in the larynx when swallowing, often radiating to the ear. With cancer of the true vocal cords, the most characteristic initial symptom is hoarseness .
With cancer of the lower larynx, slowly increasing difficulty breathing and hoarseness are more typical. As the tumor spreads to surrounding tissues and organs, these symptoms intensify, laryngostenosis gradually develops, metastases appear in the lymph nodes and nodes of the neck, and the general condition of the patients worsens.
When localized on the true vocal cords, voice formation is disrupted very early: first, the timbre of the voice changes, it becomes rough, and then hoarseness . Hoarseness most often forces the patient to see a doctor.
Later, as the tumor grows, the hoarseness intensifies, and the patient can only speak in a whisper. Along with this, another symptom develops, shortness of breath. In advanced stages, pain appears when swallowing.
With cancer of the epiglottis and arytenoid cartilages, the feeling of pain is preceded by a feeling of awkwardness or something foreign. In case of tumor disintegration and secondary perichondritis, pain in the larynx increases significantly. After some more time, hemoptysis, choking, and difficulty in passing food through the esophagus appear.
The decaying tumor emits a stench. Patients lose weight, become weaker, and cachexia increases. Clinical manifestations of laryngeal cancer are quite varied and depend primarily on the location and extent of the tumor lesion . Symptoms of cancer of the supraglottic region are scanty; at first, mainly unpleasant sensations or slight pain in the larynx are noted.
When the vocal folds are affected, the early and main symptom is gradually increasing hoarseness . Only cancer of the subglottic region occurs latently for a long time, difficulty breathing increases gradually and hoarseness increases slowly.
Other reasons
Foreign bodies enter the larynx mainly from the oral cavity. More often observed in children who have the habit of holding small objects in their mouths. A dangerous condition associated with small objects entering the respiratory tract: fish bones, needles, beads, coins. If the foreign body cannot be coughed out, it slips down into the trachea (all the way to the bronchi).
Larger objects can cause complete blockage of the lumen of the larynx - suffocation develops. With small foreign bodies, a convulsive cough, pain in the larynx, the face and lips turn blue, and hoarseness are observed. When completely blocked, suffocation occurs and death occurs. The main symptoms of gastroesophageal reflux disease are:
- heartburn;
- acute pain in the larynx;
- air burps;
- burning and feeling of pressure.
Zhennia occurs in the epigastric region 15-40 minutes after eating and is provoked by foods that stimulate the synthesis of acid and bile: fried, spicy food, sour juices, alcohol, especially dry red wine, carbonated drinks, consumption of soft-boiled eggs, radishes, radishes, large amounts of vegetable fat If you have pain in the larynx, seek help from an otolaryngologist, oncologist, or infectious disease specialist.
Morbidity statistics
Laryngeal cancer accounts for 2.6% of all cancers. It is in first place in terms of incidence among head and neck tumors. In 95% of cases, malignant lesions of the larynx are squamous cell carcinoma, 2% each are glandular cancer and basal cell carcinoma, and 1% are rare types of cancer.
Men are more susceptible to the disease - they are diagnosed 9-10 times more often than women. 80-95% of patients are men from 40 to 60 years old. Most of them are heavy smokers.
The survival prognosis directly depends on the stage at which the cancer is detected and its location. If the tumor is detected at stage I, the five-year survival rate is 85%, at stage II – 70%, at stage III – 60%, at stage IV it decreases to 20%.
When chemoradiation therapy is started in the early stages, stable remission is achieved in 85-95% of cases, in late stages - in 30-40%.
Neoplasms of the upper part of the larynx give metastases to regional lymph nodes in 35-45% of cases, of the lower part - in 15-20%. In the area of the vocal cords, the lymphatic network is less developed, so the tumor in this area metastasizes rarely and late.
Diagnosis of laryngeal cancer
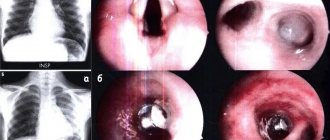
During the initial visit, the doctor collects an anamnesis of the patient’s life and illness, asks him about the presence of provoking factors, conducts a visual examination, palpation of the neck, indirect laryngoscopy - examination of the larynx with a mirror on a long curved handle.
If there is still suspicion of a tumor formation, the patient is prescribed direct laryngoscopy . This is an invasive diagnostic procedure during which the larynx, trachea, and bronchi are examined using a laryngoscope (rigid method) or a flexible fiberscope. As a rule, during direct laryngoscopy, a biopsy of the neoplasm is performed - biomaterial is taken for cytological and histological analysis.
of tumor markers SCC and CYFRA 21-1 is considered an effective diagnostic method . To analyze tumor markers, venous blood is taken from the patient.
To assess the degree of tumor invasion, damage to the lymph nodes, and the presence of metastases in distant organs and tissues, additional procedures are used: CT or MRI , PET scan , biopsy of sentinel lymph nodes , scintigraphy , radiography .