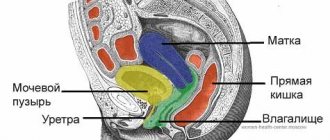
Today, many mothers know far more about pregnancy than our parents knew. Therefore, many women during pregnancy worry about the state of their health, and are very worried if the doctor talks about the condition of such an important organ during pregnancy as the placenta. This organ performs the most important functions, and without it it is impossible to carry a pregnancy to term. Deviations in the structure or functioning of the placenta can lead to complications for the mother or fetus, and certain measures must be taken in a timely manner to correct everything. But what can happen to the placenta, and how can it be dangerous? Let's figure it out together.
What is the placenta?
The term “placenta” itself comes from the Greek language and is translated by the simple word “cake”. Indeed, in appearance, the placenta resembles a large and voluminous cake with a “tail” extending from it in the form of an umbilical cord. But this cake is extremely important for every woman carrying a baby; it is due to the existence of the placenta that it is possible to carry and give birth to a child normally. In terms of structure, the placenta, or, as it may be called differently in the literature, “baby place,” is a complex organ. The beginning of its formation occurs at the time of implantation of the embryo into the wall of the uterus (from the moment the embryo attaches to one of the walls of the uterus).
How does the placenta work?
The main part of the placenta is special villi, which branch in it and form from the beginning of pregnancy, resembling the branches of centuries-old trees. The baby’s blood circulates inside the villi, and outside the villi are actively washed by the blood coming from the mother. That is, the placenta combines two circulatory systems at once - the maternal one from the uterus, and the fetal one from the amniotic membranes and the baby. According to this, the sides of the placenta are also different - smooth, covered with membranes, with an emerging umbilical cord - on the fetal side, and uneven lobulated - on the mother's side.
Trophoblast
At the beginning of the second month of embryogenesis, the trophoblast has a large number of secondary and tertiary villi, which give it a radiant appearance. The villi are immersed in the mesoderm of the chorionic plate, and at the periphery they are attached to the maternal decidua with the help of an outer layer of cytotrophoblast. The surface of the villus is covered with syncytium, which lies on a single layer of cytotrophoblast cells covering the core of the villus, formed by vascularized mesoderm. The capillary system of the core of the stem villi comes into contact with the capillaries of the chorionic plate and connecting stalk, giving rise to the extraembryonic vascular system.
Over the next months, numerous small branches grow from the stem villi into the surrounding lacunar and intervillous spaces. At first these villi are primitive, but before the beginning of the fourth month the cytotophoblast cells and some connective tissue cells disappear. Thus, the maternal and fetal vascular systems are separated only by the syncytium and the endothelial wall of the blood vessels of the chorionic villi.
The syncytium can become thinner, and large segments of it with several nuclei break off and enter the intervillous blood lacunae. Such debris - syncytial nodes - enter the maternal vascular system and of course degenerate without causing any symptoms. The disappearance of cytotrophoblast cells begins from the smaller villi and moves to the larger ones. Although some cytotrophoblastic elements remain in the large villi, they do not participate in the metabolism between the maternal and fetal circulatory systems.
What is the placental barrier?
It is in the area of the villi that an active and constant exchange of substances occurs between the baby and his mother. From the mother's blood, the fetus receives oxygen and all the necessary nutrients for growth and development, and the baby gives the mother metabolic products and carbon dioxide, which the mother removes from the body for two. And the most important thing is that the blood of the mother and fetus does not mix in any part of the placenta. The two vascular systems - the fetus and the mother - are separated by a unique membrane that is capable of selectively allowing some substances to pass through and retaining other, harmful substances. This membrane is called the placental barrier. Gradually forming and developing along with the fetus, the placenta begins to fully function by approximately twelve weeks of pregnancy. The placenta retains bacteria and viruses penetrating into the maternal blood, special maternal antibodies that can be produced in the presence of Rh conflict, but at the same time the placenta easily allows the nutrients and oxygen necessary for the child to pass through. The placental barrier has the property of special selectivity; different substances coming from different sides of the placental barrier penetrate the membrane to varying degrees. Thus, many minerals actively penetrate from the mother to the fetus, but practically do not penetrate from the fetus to the mother. And also, many toxic substances actively penetrate from the baby to the mother, but practically do not pass back from her.
What are the dangers of low placental location?
This pathology is considered dangerous to the life and health of both the child and his mother. The greatest risks include:
- Miscarriage or premature birth. The likelihood of this outcome is due to the fact that with placental insufficiency the uterus experiences higher loads than during a normal pregnancy. Any physical stress and even mental stress can cause intense uterine contractions, expelling the fetus. Moreover, the likelihood of this remains throughout the entire pregnancy.
- Fetal presentation. If the placenta has formed low in early pregnancy, the risk of fetal malposition increases by 50%. Developing in the mother's belly, the unborn child strives to take a position so that its head is in contact with anything as little as possible - including the “baby place”. Transverse or breech presentation of the fetus makes natural childbirth impossible and is a pathological condition that threatens both itself and its mother.
- Fetal hypoxia. With inferior placenta previa, the blood supply to the embryo with nutrients and oxygen deteriorates. Chronic and acute hypoxia causes irreversible changes in the child’s brain, delays his intrauterine development, and during childbirth can lead to his death.
- Uterine bleeding. This complication threatens a woman with placental insufficiency throughout pregnancy. This risk is especially great in the later stages, when the fetus becomes quite large and puts more pressure on the walls of the uterus, increasing the likelihood of placental abruption from the endometrium. Mild but regular bleeding provokes the development of anemia in the mother, which, in turn, is one of the causes of chronic embryonic hypoxia. With severe placental abruption, extensive hemorrhage may develop with hemorrhagic shock, fatal for both the woman and her child.
All of these complications make placenta previa a dangerous pathology. Therefore, when it is detected, a woman is at risk. Depending on the type of pathology, doctors develop a special treatment strategy that will save the life of both the mother and her child.
Take the first step
make an appointment with a doctor!
Hormonal function of the placenta
In addition to the excretory function, fetal breathing (since the placenta temporarily replaces the baby’s lungs), and many other functions, the placenta has another function that is important for pregnancy as a whole - hormonal. Once the placenta begins to fully function, it can produce up to 15 different hormones that perform various functions during pregnancy. The very first of these are sexual functions, which help in maintaining and prolonging pregnancy. Therefore, gynecologists, if there is a threat of early pregnancy termination, always wait 12-14 weeks, helping in the early weeks of pregnancy with external hormones (duphaston or utrozhestan). Then the placenta begins to actively work and the threat disappears. The functions of the placenta are so great that in the initial stages the placenta grows and develops even faster than your baby grows. And this is not without reason, by the time of 12 weeks the fetus weighs about 5 grams, and the placenta is up to 30 grams, by the end of pregnancy, at the time of birth, the size of the placenta will be about 15-18 cm, and the thickness will be up to 3 cm, with a weight of about 500 -600 grams.
Amnion, umbilical cord and amniotic fluid
The contact zone between the amnion and the embryonic ectoderm (amnioectodermal communication) has an oval shape and is called the primary umbilical ring. In the fifth week of development, the following structures pass through this ring:
1) a connecting stalk containing the allantois and umbilical vessels, which are represented by two arteries and one vein;
2) yolk stalk (egg strait), which is accompanied by yolk vessels;
3) a canal connecting the intraembryonic and extraembryonic cavity. The yolk sac is localized in the chorionic cavity, i.e. in the space between the amnion and the chorionic plate.
During further development, the amniotic cavity rapidly enlarges at the expense of the chorionic cavity, and the amnion surrounds the connecting stalk and the yolk sac strait, connecting them and forming the primary umbilical cord. In the distal part, the primary umbilical cord contains the yolk strait and umbilical vessels, and in the proximal part - intestinal loops and remnants of the allantois.
The yolk sac is contained in the chorionic cavity and communicates with the umbilical cord through its duct. At the end of the third month, the amnion expands so that it comes into contact with the chorion, and the chorionic cavity is obliterated. The yolk sac is also obliterated. The abdominal cavity then becomes insufficient for intestinal loops, which develop and some of them, as part of the umbilical cord, are pushed into the extraembryonic space. These pushed out loops of intestine form a physiological umbilical hernia. At the end of the 3rd month of development, the intestinal loops are retracted into the fetal body, and the cavity in the umbilical cord becomes overgrown.
After obliteration of the vitelline duct and allantois, only the umbilical vessels remain in the umbilical cord, surrounded by Wharton's jelly, a specialized type of connective tissue high in proteoglycans that functions as a protective environment for the umbilical cord vessels. The walls of the umbilical arteries have many muscle and elastic fibers, which contribute to the rapid narrowing and contraction of the umbilical vessels after ligation of the umbilical cord.
The amniotic cavity is filled with a clear, watery fluid (amniotic fluid), which is partly produced by amniotic cells and which primarily comes from the mother's blood. The amount of fluid increases from 30 ml at the 10th week of pregnancy to 350 ml at the 20th and 800-1000 ml at the 37th week. Amniotic fluid allows the embryo to move and softens shocks, separating the fetus from the amnion. The full volume of amniotic fluid is renewed every 3 hours. From the beginning of the 5th month, the fetus begins to swallow amniotic fluid: it drinks about 400 ml of amniotic fluid per day, which is half of its total amount. From the 5th month, fetal urine, which contains mainly water, is added to the amniotic fluid (end products of metabolism are removed by the placenta). During labor, the amniotic sac forms a hydrostatic wedge, which helps dilate the cervical canal.
Clinical correlations
Anomalies of the umbilical cord . At birth, the umbilical cord has a diameter of about 2 cm and a length of 50-60 cm. It is convoluted and can form pseudonodes. As its length increases, the umbilical cord can wrap around the fetal neck without adverse consequences, and a very short umbilical cord can cause premature separation of the placenta during childbirth. Normally, the umbilical cord has 2 arteries and 1 vein. In 1 in 200 newborns, only 1 artery is present, and 20% of these children may have cardiovascular defects. The umbilical cord artery either does not form (agenesis) or degenerates in the early stages of development.
Amniotic bands . Rarely, amnion ruptures in early pregnancy can lead to the formation of amniotic bands that cover parts of the fetus: limbs, fingers. This causes amputations, annular constrictions, and craniofacial deformities.
Umbilical cord
The placenta on the fetal side is connected to the baby by a special strong cord - the umbilical cord, inside which there are two arteries and one vein. The umbilical cord can attach to the placenta in several ways. The first and most common is the central umbilical cord attachment, but lateral or marginal umbilical cord attachment may also occur. The umbilical cord functions are not affected in any way by the method of attachment. A very rare option for attaching the umbilical cord may be attachment not to the placenta itself, but to its fetal membranes, and this type of attachment is called membrane.
Problems with the placenta
Most often, the placenta and umbilical cord system work harmoniously and supply the baby with oxygen and nutrition. But sometimes malfunctions may occur in the placenta due to the influence of various factors - external or internal. There are various kinds of developmental disorders or problems with the functioning of the placenta. Such changes in the placenta do not go unnoticed for the mother and fetus; often problems with the placenta can have serious consequences. We will talk about the main abnormalities in the development and functioning of the placenta and how to identify and treat them.
Blood supply to the placenta
The cotyledon receives blood from 80-100 spiral arteries that penetrate the decidual plate and enter the intervillous spaces at almost regular intervals. The lumen of the spiral arteries is narrow, so the blood pressure in the intervillous space is high. Thanks to this, blood enters to a considerable depth into the intervillous spaces and washes the numerous villi of the chorion with oxygenated blood.
When the pressure decreases, blood returns from the chorionic plate to the decidua and from there to the endometrial veins. Thus, blood from the intervillous lacunae returns to the maternal circulation through the endometrial veins.
The intervillous space of the mature placenta holds about 150 ml of blood, which is renewed 3-4 times per minute and washes the chorionic villi, the surface area of which ranges from 4 to 14 m2. But placental exchange does not occur in all villi, but only in those where the fetal vessels are in close contact with the syncytial cover. In these villi, the syncytium forms additional microvilli, which increase the contact area, and therefore the rate of exchange, between maternal and fetal blood.
The placental barrier, which separates the mother's blood from the fetus's blood, initially consists of four layers:
- fetal vascular endothelium;
- connective tissue of the villus core;
- cytotrophoblastic layer;
- syncytium.
From the fourth month, the placental membrane becomes thinner due to the fact that the vascular endothelium comes into close contact with the syncytial membrane, thereby increasing the metabolic rate. But the placental barrier can allow many substances to pass through. Considering that maternal blood in the intervillous space is separated from the fetal blood by chorion derivatives, the human placenta is classified as hemochorial type.
Placental hypoplasia
Reducing the size or thinning of the placenta in medical language is called “placental hypoplasia.” You should not be afraid of this diagnosis, because... it occurs quite often. The fetus is affected only by a significant decrease in the diameter and thickness of the placenta. A significantly reduced placenta, a small baby's place, is uncommon. This diagnosis is made if the reduction in size is significant compared to the lower limit of normal for the size of the placenta at a given stage of pregnancy. The causes of this type of pathology have not yet been clarified, but according to statistics, usually a small placenta is associated with the development of severe genetic abnormalities in the fetus. I would like to immediately make a reservation that the diagnosis of “placental hypoplasia” is not made based on a single ultrasound; it can only be made as a result of long-term observation of a pregnant woman. In addition, it is always worth remembering that there may be individual deviations in the size of the placenta from standard, generally accepted normal values, which will not be considered a pathology for each specific pregnant woman in each of her pregnancies. So, for a small and slender woman, the placenta should be smaller in size than for a large and tall woman. In addition, there is no absolute proof of the relationship between placental hypoplasia and the presence of genetic disorders in the fetus. But when a diagnosis of placental hypoplasia is made, parents will be advised to undergo medical genetic counseling. During pregnancy, a secondary reduction in size of the placenta may occur, which may be associated with exposure to various unfavorable factors during pregnancy. This could be chronic stress or fasting, drinking alcohol or smoking, or drug addiction. Also, the causes of underdevelopment of the placenta during pregnancy can be hypertension in the mother, a sharp exacerbation of chronic pathology, or the development of some acute infections during pregnancy. But in the first place when the placenta is underdeveloped, there is gestosis with the development of severe edema, high blood pressure and the appearance of protein in the urine. Changes in the thickness of the placenta occur. A placenta is considered thin if it has insufficient mass but is of a size that is quite normal for its age. Often, such thin placentas occur with congenital defects of the fetus, and children are born with manifestations of feto-placental insufficiency, which causes serious problems with the health of the newborn. But unlike a primary hypoplastic placenta, such children are not associated with the risk of developing dementia. Sometimes a membranous placenta is formed - it is very wide and very thin, measuring up to 40 cm in diameter, almost twice as large as normal. Typically, the cause of the development of such a problem is a chronic inflammatory process in the endometrium, which leads to dystrophy (depletion) of the endometrium.
Ultrasound Gynecologist
PLACENTA, MEMBRANES AND UMBRICAL CORD
The placenta is the organ that unites mother and fetus. The development and condition of the fetus depends on the functioning of the placenta. There are many methods for studying placental function. However, the most informative remains the examination of the placenta after birth. Such an examination helps in assessing the condition of the newborn, as well as in choosing tactics for managing the postpartum period. The placenta is examined immediately after birth, primarily to assess its integrity. Then the entire afterbirth is examined more carefully. Umbilical cord blood is taken for analysis immediately after the umbilical cord is cut, even before the birth of the placenta. The afterbirth must be inspected in all cases without exception.
Examination of the placenta and umbilical cord Size and weight of the placenta: The weight of the placenta during full-term pregnancy is 1/6-1/7 of the weight of the fetus. The mature placenta has the form of a disk with a diameter of 15-20 cm and a thickness of 2-3 cm. Its average weight is 400-600 g. - Placental hyperplasia. The weight of the placenta is 1/3-1/2 of the weight of the fetus. Placental hyperplasia occurs in hemolytic disease of the newborn, congenital syphilis and diabetes mellitus classes A-C according to P. White’s classification. Moderate placental hyperplasia occurs in heavy smokers. — Placental hypoplasia is observed in women suffering from hypertension and arterial hypertension during pregnancy. Placental hypoplasia is often combined with intrauterine growth retardation. The umbilical cord has a length of 50-70 cm. During examination, pay attention to the presence of nodes and attachment of the umbilical cord (to the placenta or fetal membranes), and note the number of umbilical cord vessels. If the length of the umbilical cord is less than 40 cm, the umbilical cord is said to be absolutely short . This condition can be accompanied by serious complications during vaginal delivery. — True umbilical cord nodes occur in 1% of births. Perinatal mortality reaches 6%. True umbilical cord knots are formed when the umbilical cord is excessively long, when the fetus, due to significant mobility, slips through its coil. During childbirth, this pathology manifests itself as bradycardia in the fetus. False umbilical cord nodes are thickenings of individual sections of the umbilical cord due to sharp twisting of the umbilical arteries or varicose veins of the umbilical vein. False umbilical cord knots do not pose a danger to the fetus. Entanglement of the umbilical cord around the fetal neck occurs in 20-24% of births, usually with an umbilical cord length of more than 70 cm. Entanglement of the umbilical cord, as a rule, does not pose a danger to the fetus. Decelerations may appear on CTG during labor. The umbilical cord is usually attached to the central part of the placenta.
In most cases of marginal umbilical cord attachment, childbirth occurs without complications. However, an attempt to release the placenta by pulling on the umbilical cord can lead to its separation.
Umbilical cord attachment
In this case, the umbilical cord is attached not to the placenta itself, but to the fetal membranes at some distance from the edge of the placenta. The vessels are directed from the root of the umbilical cord through the membranes to the placenta. If a section of the membranes with vessels passing through it is located above the internal os below the presenting part of the fetus, they speak of vasa previa. This pathology can be suspected when the rupture of amniotic fluid is accompanied by bleeding. The diagnosis is confirmed by detecting fetal red blood cells in a smear of the contents of the posterior vaginal vault, stained by Kleihauer-Betke, or using rapid tests. Treatment consists of emergency delivery. In some cases, when a child is born in a state of severe anemia and hypoxia, he is given a transfusion of blood products immediately after birth. In multiple pregnancies, the umbilical cord attachment may be complicated by blood loss in one or both fetuses.
The risk of velamentous umbilical cord attachment in a singleton pregnancy is 1%. With twins and, especially, with triplets, it is much higher.
Agenesis of one of the umbilical arteries
The prevalence of this pathology in singleton pregnancies is 0.2-1.1%. Risk factors include diabetes mellitus and maternal trisomy. In 25-50% of cases, the disease is combined with other malformations - cleft palate, heart defects, kidney defects, urinary tract defects, genital defects and musculoskeletal defects. Children are more often born low birth weight. Developmental defects are usually multiple, and the child is often not viable. If agenesis of one of the umbilical arteries is detected, a thorough examination of the newborn is performed.
In case of twins, this pathology is observed in one of the twins in 7% of cases. However, the risk of birth defects is significantly lower than with a singleton pregnancy.
An additional third umbilical cord artery is identified much less frequently, which is not associated with any abnormalities in fetal development.
Bleeding in the postpartum period
Retention of a fragment of the placenta in the uterus is a common cause of postpartum hemorrhage. The diagnosis is made by examining the maternal surface of the placenta. Retention of a lobule or part of a lobule is indicated by a defect in the placental tissue. Immediate manual or instrumental examination of the walls of the uterine cavity under general anesthesia is indicated.
Retention of an additional lobe of the placenta in the uterus.
Retroplacental blood clots and hematomas
The most common causes of blood clots on the maternal surface of the placenta are listed below.
Rupture of the marginal sinus is the most likely cause of bleeding from the genital tract in the third trimester of pregnancy (in the absence of previa and premature placental abruption). Upon examination, blood clots are found at one of the edges of the placenta.
Premature placental abruption. When examining the placenta, a blood clot tightly attached to it is found on the maternal surface, the dimensions of which correspond to the area of detachment. The appearance and consistency of the clot depend on how much time has passed since the detachment. An old hematoma is usually dense; when it is separated, a plate-shaped depression remains on the placenta. Blood clots on the maternal surface of the placenta can also be detected during preeclampsia (the clinical picture of premature placental abruption is often absent).
Treatment consists of delivery. The diagnosis is confirmed after examining the placenta.
Fibrin deposition in the intervillous space is observed during physiological maturation of the placenta and is especially pronounced during post-term pregnancy. Fibrin deposition takes the form of multiple whitish spots on the maternal surface of the placenta. They are dense to the touch, especially if calcification has occurred. Placental infarctions look like clearly demarcated foci of dense consistency. Heart attacks are more often located deep in the placenta, less often on its maternal surface. On a section of the lesion, you can determine the duration of the infarction (fresh - with hemorrhages or old - with signs of organization).
Small marginal infarcts are observed normally during physiological aging of the placenta as a result of its atrophy. More often, placental infarctions occur with hypertension or preeclampsia.
A fresh infarction has a dark purple color, unclear contours, its base borders the decidua. As it ages, it thickens, becomes whitish or pale yellow in color, and becomes well demarcated from surrounding tissue.
Heart attacks develop as a result of microthrombosis or prolonged spasm of the spiral arteries of the endometrium. Atherosclerotic changes in larger arteries secondary to arterial hypertension also predispose to placental infarctions. Complications of placental infarction are intrauterine hypoxia and intrauterine growth retardation. Heart attacks are often detected with premature placental abruption.
Fruiting surface of the placenta The membranes covering the fruiting surface of the placenta are thin, transparent, steel-blue in color.
Staining of the membranes with meconium is observed in 20% of births, usually during post-term pregnancy. The shells acquire a brownish-greenish color. Early childhood mortality is increased in this group of newborns. Its causes are meconium aspiration and other complications of postmaturity, as well as intrauterine growth retardation.
Chorioamnionitis. The shells are thickened, whitish, opaque, sometimes with a strong unpleasant odor.
Subchorionic fibrin deposition is normal and is considered a sign of placental maturity. On the fruit surface, gray-white overlays of dense consistency and varying diameters are determined, located singly or in groups. Subchorionic cysts are thin-walled cavities with a diameter of 4-5 cm, filled with serous or mucous contents, sometimes mixed with blood. Located on the fetal surface of the placenta. Occurs normally. Nodular amnion
Definition. On the surface of the amnion, grayish-yellow deposits with a diameter of 2-3 mm are found, especially numerous in the area of umbilical cord attachment. The overlays consist of desquamated fetal epidermis and are easily removed.
Examination. Nodular amnion occurs with oligohydramnios and is usually combined with malformations of the kidneys and urinary tract (bilateral renal agenesis, polycystic kidney disease, urinary tract obstruction). In this regard, the detection of nodular amnion must be reported to the neonatologist.
Amniotic plaques On the fetal surface of the placenta, zones of metaplasia of the columnar epithelium of the amnion into multilayered squamous epithelium are determined in the form of small grayish plaques with a granular surface. Unlike nodular amnion, plaques are difficult to remove. Amniotic plaques are commonly seen in full-term pregnancies. They are the result of physiological changes in placental tissue. Additional slices
Definition. Additional lobules are formed from trophoblast tissue that has not undergone atrophy and can be located at some distance from the placenta. In this case, the additional lobules are connected to the placenta by membranes through which blood vessels pass. The retention of an additional lobule in the uterus after the birth of the placenta can cause bleeding.
Diagnosis and treatment. Broken vessels at the edges of the placenta indicate that there is an additional placenta lobe remaining in the uterus. To remove an additional lobe, a manual or instrumental examination of the walls of the uterine cavity is performed under general anesthesia.
A placenta surrounded by a cushion (placenta circumvallata) is formed as a result of detachment and twisting of the edges of the placenta in early pregnancy. In this case, the smooth chorion is located in the form of a roller around the chorionic plate. If detachment and twisting occur along the very edge of the placenta, a placenta is formed surrounded by a rim (placenta marginata).
Clinical picture. In most cases, there are no manifestations and the placenta, surrounded by a cushion, is discovered by chance when examining the placenta. Bleeding and leakage of amniotic fluid during pregnancy, premature birth, malformations and perinatal fetal death may occur.
Diagnosis and treatment. Clinical manifestations - increased uterine tone, leakage of amniotic fluid and bleeding - appear at the end of the second or beginning of the third trimester of pregnancy. There is no etiotropic treatment. Pregnancy may end in premature birth.
Afterbirth during multiple pregnancy
— Bichorionic biamniotic twins:
Each twin has its own chorion and amnion. The septum between the cavities in which the fruits are located consists of two amnions (thin transparent membranes) and two smooth chorions lying between them. To clarify the diagnosis, a histological examination of the septum is indicated.
— Monochorionic biamniotic twins:
Both amnions are enclosed in one chorion common to both twins. The septum between the fetuses consists of the membranes of two amnions. The diagnosis is confirmed by histological examination of the septum.
— Monochorionic monoamniotic twins:
The amniotic cavity is common to both twins, there is no septum. The umbilical cords of both fetuses are attached to the placenta very close to each other, as a result of which their twisting and death of the fetus is possible.
Prognosis Perinatal mortality is higher among monochorionic twins than among bichorionic twins. The reason is that in the common placenta anastomoses are formed between the vessels of the circulatory systems of the twins. Depending on the type of anastomosis (arterioarterial, arteriovenous or venovenous) and the diameter of the vessels forming them, the following outcomes are possible.
Development of two normal fetuses.
Feto-fetal transfusion, which is manifested by severe polyhydramnios of one fetus and developmental delay of the other.
Normal development of one fetus and severe pathology in the other (congenital absence of a heart, mummification).
Identical and fraternal twins
Identical twins . The type of placentation depends on the period of placental formation during which the division of a single embryonic rudiment occurred. All three types of placentation described above are possible, but more often a common placenta is formed. Separate placentas develop in 30% of cases.
Fraternal twins. When two fertilized eggs develop simultaneously, separate placentas are always formed. Placentas are often closely adjacent to each other.
Umbilical cord
Sheathed umbilical cord attachment is observed more often than in singleton pregnancies.
Agenesis of one of the umbilical arteries is observed in 7% of cases (more often in singleton pregnancies).
Placental hyperplasia
In contrast, a very large, giant placenta occurs, which usually occurs in cases of severe gestational diabetes. Enlargement (hyperplasia) of the placenta also occurs in diseases of pregnant women such as toxoplasmosis or syphilis, but this is not common. An increase in the size of the placenta may be the result of kidney pathology in the unborn baby, in the presence of Rh conflict, when the fetal red blood cells with Rh protein begin to attack the mother's antibodies. The placenta can increase significantly in case of thrombosis of its vessels, if one of the vessels is blocked, as well as in case of pathological growth of small vessels inside the villi. An increase in the thickness of the placenta more than normal may be associated with its premature aging. Thickening of the placenta is also caused by such pathologies as Rh-conflict, hydrops fetalis, diabetes mellitus in pregnancy, gestosis, viral or infectious diseases suffered during pregnancy, placental abruption. Thickening of the placenta is normal in multiple pregnancies. In the first and second trimesters, an enlarged placenta usually indicates a previous viral disease (or latent carriage of the virus). In this case, the placenta grows to prevent disease in the fetus. Rapid growth of the placenta leads to its premature maturation, and consequently, aging. The structure of the placenta becomes lobular, calcifications form on its surface, and the placenta gradually ceases to provide the fetus with the necessary amount of oxygen and nutrients. The hormonal function of the placenta also suffers, which leads to premature birth. Treatment for placental hyperplasia usually involves careful monitoring of the fetus.
Thickness
It is also determined through ultrasound examination - placentometry: after establishing the placenta attachment site, the area where it is largest is found, which is determined. The thickness of the placenta, as already mentioned, continuously increases until 36-37 weeks of pregnancy (by this period it ranges from 20 to 40 mm). Then its growth stops, and subsequently the thickness of the placenta either decreases or remains at the same level.
Deviation from the norm of at least one of these indicators may indicate trouble during pregnancy.
What is dangerous about changing the size of the placenta?
Why are doctors so worried about significant changes in placenta size? Usually, if the size of the placenta changes, functional insufficiency in the functioning of the placenta may also develop, that is, so-called feto-placental insufficiency (FPI), problems with the supply of oxygen and nutrition to the fetus, will form. The presence of FPN may mean that the placenta cannot fully cope with the tasks assigned to it, and the child experiences a chronic lack of oxygen and the supply of nutrients for growth. In this case, problems can grow like a snowball, the child’s body will suffer from a lack of nutrients, as a result, it will begin to lag behind in development and IUGR (intrauterine growth retardation in the fetus) or fetal growth restriction syndrome (FGR) will form. To prevent this from happening, it is best to engage in advance prevention of such conditions, treatment of chronic pathology even before pregnancy, so that exacerbations do not occur during pregnancy. During pregnancy, it is important to control blood pressure, blood glucose levels and protect the pregnant woman as much as possible from any infectious diseases. You also need a good diet with enough proteins and vitamins. When diagnosing “placental hypoplasia” or “placental hyperplasia”, careful monitoring of the course of pregnancy and the condition of the fetus is first required. The placenta cannot be cured or corrected, but there are a number of medications prescribed by a doctor to help the placenta perform its functions. In the treatment of emerging feto-placental insufficiency, special drugs are used - Trental, Actovegin or Curantil, which can improve blood circulation in the placental system on both the maternal and fetal side. In addition to these medications, intravenous infusions of drugs can be prescribed - rheopolyglucin with glucose and ascorbic acid, saline solutions. The development of FPN can have varying degrees of severity and should not be self-medicated; this can lead to the loss of the child. Therefore, it is necessary to follow all the appointments of the obstetrician-gynecologist.
Changes in the structure of the placenta
The normal placenta has a lobular structure; it is divided into approximately 15-20 lobules of equal size and volume. Each of the lobules is formed from villi and a special tissue that is located between them, and the lobules themselves are separated from each other by partitions, however, not complete ones. If changes occur in the formation of the placenta, new variants of the structure of the lobules may arise. Thus, the placenta can be bilobed, consisting of two equal parts that are connected to each other by special placental tissue; a double or triple placenta can also be formed, the umbilical cord will be attached to one of the parts. Also, a small additional lobule may be formed in a normal placenta. Even less commonly, a so-called “fenestrated” placenta may occur, which has areas covered with a membrane and resembling windows. There can be many reasons for such deviations in the structure of the placenta. Most often this is a genetically determined structure, or a consequence of problems with the uterine mucosa. Prevention of such problems with the placenta can be the active treatment of inflammatory processes in the uterine cavity even before pregnancy, during the planning period. Although deviations in the structure of the placenta do not have such a strong effect on the child during pregnancy, and almost never affect its development. But during childbirth, such a placenta can cause a lot of trouble for doctors - such a placenta can be very difficult to separate from the wall of the uterus after the baby is born. In some cases, separation of the placenta requires manual control of the uterus under anesthesia. Treatment for the abnormal structure of the placenta during pregnancy is not required, but during childbirth you must remind the doctor about this so that all parts of the placenta are born and no pieces of the placenta remain in the uterus. This is dangerous due to bleeding and infection.
Discharge of placenta after childbirth
Normally, after the birth of a baby, the placenta should separate and be released on its own within 20-30 minutes. During this time, the doctor observes the discharge of the placenta without forcing it. There are certain signs of separation of the placenta (a woman may feel a weak contraction; when the woman breathes deeply, the umbilical cord section does not retract, the fundus of the uterus rises higher and deviates to the right), and only after its separation can the placenta be removed from the genital tract if it is not born on its own. Pulling the unseparated placenta by the umbilical cord and squeezing it through the anterior abdominal wall are not used, as they are dangerous due to bleeding.
Faster separation of the placenta and better contraction of the uterus is facilitated by putting the baby to the breast immediately after birth. This is explained by the fact that when the nipple is irritated, the hormone oxytocin is released, which has a contractile effect on the uterus.
If the placenta does not separate on its own within 30 minutes, proceed to manual separation of the placenta. This procedure is performed under intravenous anesthesia.
After the birth of the placenta, it must be examined by a doctor. It is important for the doctor to make sure that the placenta is intact, because if a placenta lobe is retained in the uterus, bleeding may occur. Therefore, if a defect in the placental tissue is suspected, a manual examination of the uterine cavity is performed under intravenous anesthesia.
A possible complication is the placenta accreting into the uterine wall. It is impossible to separate it. In this case, it is necessary to remove the uterus along with the placenta, since an attempt to separate it leads to massive bleeding that is life-threatening.
Degree of maturity of the placenta
During its existence, the placenta goes through four successive stages of maturation: Placenta maturity level 0 – normally lasts up to 27-30 weeks. Sometimes at these stages of pregnancy there is 1 degree of placental maturity, which can be caused by smoking or drinking alcohol during pregnancy, as well as by previous infection. Degree of placental maturity 1 – from 30 to 34 weeks of pregnancy. During this period, the placenta stops growing and its tissues thicken. This is a crucial period when any deviations can pose a danger to the health of the fetus. Degree of placental maturity 2 – lasts from 34 to 39 weeks of pregnancy. This is a stable period when some advance in the maturity of the placenta should not cause concern. Placenta maturity level 3 – can normally be diagnosed starting from the 37th week of pregnancy. This is a stage of natural aging of the placenta, but if it is combined with fetal hypoxia, the doctor may recommend a cesarean section.
Sources
- Tiwari D., Das CR., Sultana R., Kashyap N., Islam M., Bose PD., Saikia AK., Bose S. Increased homocysteine mediated oxidative stress as a key determinant of hepatitis E virus (HEV) infected pregnancy complication and outcome: A study from Northeast India. // Infect Genet Evol - 2021 - Vol - NNULL - p.104882; PMID:33905889
- Salmanian B., Belfort MA., Shamshirsaz A.A. The risk of placenta accreta spectrum in women with in vitro fertilization in different populations. // Am J Obstet Gynecol - 2021 - Vol - NNULL - p.; PMID:33905744
- Olmos-Ortiz A., Olivares-Huerta A., García-Quiroz J., Zariñán T., Chavira R., Zaga-Clavellina V., Avila E., Halhali A., Durand M., Larrea F., Díaz L. Placentas associated with female neonates from pregnancies complicated by urinary-tract infections have higher cAMP content and cytokines expression than males. // Am J Reprod Immunol - 2021 - Vol - NNULL - p.e13434; PMID:33905581
- Tandl V., Hoch D., Bandres-Meriz J., Nikodijevic S., Desoye G., Majali-Martinez A. Different regulation of IRE1α and eIF2α pathways by oxygen and insulin in ACH-3P trophoblast model. // Reproduction - 2021 - Vol - NNULL - p.; PMID:33904834
- Ji S., Gumina D., McPeak K., Moldovan R., Post MD., Su EJ. Human placental villous stromal extracellular matrix regulates fetoplacental angiogenesis in severe fetal growth restriction. // Clin Sci (Lond) - 2021 - Vol - NNULL - p.; PMID:33904582
- Shmeleva EV., Colucci F. Maternal natural killer cells at the intersection between reproduction and mucosal immunity. // Mucosal Immunol - 2021 - Vol - NNULL - p.; PMID:33903735
- Moreno-Sepulveda J., Espinós JJ., Checa MA. Lower risk of adverse perinatal outcomes in natural versus artificial frozen-thawed embryo transfer cycles: a systematic review and meta-analysis. // Reprod Biomed Online - 2021 - Vol - NNULL - p.; PMID:33903031
- Owen MD., Cassidy AL., Weeks AD. Why are women still dying from obstetric hemorrhage? A narrative review of perspectives from high and low resource settings. // Int J Obstet Anesth - 2021 - Vol - NNULL - p.102982; PMID:33903002
- Liu CN., Yu FB., Xu YZ., Li JS., Guan ZH., Sun MN., Liu CA., He F., Chen DJ. Prevalence and risk factors of severe postpartum hemorrhage: a retrospective cohort study. // BMC Pregnancy Childbirth - 2021 - Vol21 - N1 - p.332; PMID:33902475
- Munoz JL., Kimura AM., Xenakis E., Jenkins DH., Braverman MA., Ramsey PS., Ireland KE. Whole blood transfusion reduces overall component transfusion in cases of placenta accreta spectrum: a pilot program. // J Matern Fetal Neonatal Med - 2021 - Vol - NNULL - p.1-6; PMID:33902384
Disturbances in placental maturation
For each stage of placenta formation, there are normal periods in weeks of pregnancy. Too fast or slow passage of certain stages by the placenta is a deviation. The process of premature (accelerated) maturation of the placenta can be uniform or uneven. Typically, expectant mothers with underweight experience uniform premature aging of the placenta. Therefore, it is important to remember that pregnancy is not the time to follow various diets, since their consequences can be premature birth and the birth of a weak baby. The placenta will mature unevenly if there are problems with blood circulation in some of its zones. Typically, such complications occur in overweight women with prolonged late toxicosis of pregnancy. Uneven maturation of the placenta occurs more often with repeated pregnancies. Treatment, as with feto-placental insufficiency, is aimed at improving blood circulation and metabolism in the placenta. To prevent premature aging of the placenta, it is necessary to take measures to prevent pathologies and gestosis. But delays in the maturation of the placenta occur much less frequently, and the most common reasons for this may be the presence of diabetes mellitus in the pregnant woman, alcohol consumption and smoking. Therefore, it is worth giving up bad habits while carrying a baby.
Possible pathologies
The most common violations:
- discrepancy between the pace of development of the placenta and the baby;
- the appearance of blood clots that obstruct blood flow;
- incorrect location of the organ;
- excessive thickening;
- heart attack - cessation of blood flow through the arteries;
- various inflammations, tumors.
The reasons for these phenomena may be:
- toxicosis;
- diabetes;
- atherosclerosis;
- infectious phenomena in the mother's body;
- Rhesus conflict;
- excessive or insufficient weight of a woman;
- emotional stress;
- bad habits;
- woman's age over 35 years.
It is important that the expectant mother monitors her own well-being throughout the entire period of carrying the child. The appearance of any unusual symptoms - vaginal discharge, pain, cramps, increased swelling should be a signal for urgent contact to our center.
Placental calcifications
The normal placenta has a spongy structure, but by the end of pregnancy some of its areas may become stone; such areas are called petrificates or placental calcifications. Hardened areas of the placenta are not able to perform their functions, but usually the remaining parts of the placenta do an excellent job with the task assigned to them. As a rule, calcifications occur due to premature aging of the placenta or postterm pregnancy. In such cases, the doctor will closely monitor the pregnant woman to exclude the development of fetal hypoxia. But usually such a placenta functions quite normally.
Low attachment and placenta previa
Ideally, the placenta should be located in the upper part of the uterus. But there are a number of factors that prevent the normal location of the placenta in the uterine cavity. These could be uterine fibroids, tumors of the uterine wall, malformations, multiple pregnancies in the past, inflammatory processes in the uterus, or abortions. A low-lying placenta requires more careful monitoring. It usually tends to rise during pregnancy. In this case, there will be no obstacles to natural childbirth. But it happens that the edge of the placenta, part of it, or the entire placenta blocks the internal os of the uterus. If the placenta partially or completely covers the cervix of the uterus, natural childbirth is impossible. Typically, if the placenta is abnormally located, a caesarean section is performed. Such abnormal positions of the placenta are called incomplete and complete placenta previa. During pregnancy, a woman with placenta previa may experience bleeding from the genital tract, which leads to anemia and fetal hypoxia. The most dangerous is partial or complete placental abruption, which leads to the death of the fetus and a threat to the life of the mother. A pregnant woman needs complete rest, including sexual rest; she cannot exercise, swim in the pool, walk a lot, or work.
Villous and main decidua
In the first weeks of development, villi cover the entire surface of the chorion. During pregnancy, the villi at the embryonic pole continue to grow and spread, giving rise to the villous chorion. The villi at the opposite pole degenerate, and by the third month of embryogenesis a smooth chorion is formed. The difference in the structure of the embryonic and protiembryonic poles of the chorion also affects the structure of the decidual membrane, which is the functional layer of the endometrium and is rejected during childbirth.
The part of the decidua above the villous chorion is the main decidua (basal decidua) consists of a compact layer of large decidua cells, which are filled with lipids and glycogen. The decidua layer above the protiembryonic pole is called the bursa decidua (capsular decidua). As the size of the chorionic sac increases, this layer stretches and degenerates.
In this regard, the smooth chorion comes into contact with the wall of the uterus and the parietal decidua is formed, with which it merges, obliterating the uterine cavity. Consequently, the only part of the chorion that participates in the metabolic process is the villous chorion, which, together with the excretory membrane, forms the placenta. When the amnion and chorion merge, the amniochorionic membrane is formed, which obliterates the chorionic cavity. It is this membrane that ruptures during childbirth (when amniotic fluid breaks).
What is placental abruption?
What is premature placental abruption? This is a condition when the placenta (normally or abnormally located) leaves its place of attachment before its due date, that is, the third stage of labor. In case of placental abruption, an emergency cesarean section is necessary to save the life of the mother and fetus. If the placenta has separated in small areas, then doctors try to stop this process, maintaining the pregnancy. But even with minor placental abruption and slight bleeding, the risk of repeated episodes of abruption remains until childbirth, and the woman is carefully monitored. The causes of placental abruption can be injuries or blows to the abdomen, the presence of chronic pathologies in a woman, which leads to problems with blood circulation, defects in the formation of the placenta. Premature placental abruption can be caused by complications during pregnancy - most often gestosis with increased pressure, protein in the urine and edema, which affects all organs and systems of the mother and fetus. It is important to remember that premature placental abruption is the most dangerous complication of pregnancy!
Placental abruption Fig. 1 - complete placenta previa; Rice. 2 - marginal placenta previa; Rice. 3 - partial placenta previa 1 - cervical canal; 2 - placenta; 3 - umbilical cord; 4 - amniotic sac
Dense attachment and placenta accreta
Sometimes anomalies occur not only in the location, but also in the method of attachment of the placenta to the wall of the uterus. A very dangerous and serious pathology is placenta accreta, in which the placental villi are attached not only to the endometrium (the inner layer of the uterus, which peels off during childbirth), but also grow deep into the tissues of the uterus, into its muscular layer. There are three degrees of severity of placenta accreta, depending on the depth of villous germination. In the most severe, third degree, villi grow into the uterus to its full thickness and can even lead to uterine rupture. The cause of placenta accreta is the inferiority of the endometrium due to congenital defects of the uterus or acquired problems. The main risk factors for placenta accreta are frequent abortions, cesarean sections, fibroids, as well as intrauterine infections and uterine malformations. Low placentation may also play a certain role, since in the area of the lower segments the growth of villi into the deeper layers of the uterus is more likely. With true placenta accreta, in the vast majority of cases, removal of the uterus with placenta accreta is required. An easier case is the dense attachment of the placenta, from the accreta to the differing depth of penetration of the villi. Tight attachment occurs when the placenta is low or previa. The main difficulty with such attachment of the placenta is the delay in its birth or the complete impossibility of spontaneous passage of the placenta in the third stage of labor. If the attachment is tight, they resort to manual separation of the placenta under anesthesia.
Diseases of the placenta
The placenta, like any organ, can hurt. It can become infected, infarctions (areas deprived of blood circulation) can develop in it, blood clots can form inside the vessels of the placenta, and the placenta itself can even undergo tumor degeneration. But this, fortunately, does not happen often. Infectious damage to placental tissue (placentitis) is caused by various microbes that can penetrate the placenta in various ways. So, they can be brought with the bloodstream, penetrate from the fallopian tubes, ascending from the vagina, or from the uterine cavity. The inflammation process can be spread throughout the entire thickness of the placenta or occur in its individual areas. In this case, treatment must be specific, and it depends on the type of pathogen. Of all the possible drugs, the one that is acceptable for pregnant women at this stage will be selected. And for the purpose of prevention before pregnancy, it is necessary to carry out comprehensive therapy for chronic infections, especially in the genital tract. Placental infarction usually develops, like any other, as a result of prolonged ischemia (spasm of placental vessels), and then the areas of the placenta that receive blood from these vessels die as a result of oxygen deficiency. Typically, infarctions in the placenta occur as a result of severe gestosis or the development of hypertension in the pregnant woman. Placentitis and placental infarction can cause FPN and problems with fetal development. Sometimes, as a result of inflammation or damage to the vascular wall, when blood viscosity is disrupted, or due to sudden movements of the fetus, blood clots form inside the placenta. But small blood clots do not affect the course of pregnancy in any way.
Structure of the placenta
At the beginning of the fourth month of development, the placenta is mature and consists of two parts: the fetal part, formed by the villous chorion, and the maternal part, formed by the main membrane. On the fetal side, the placenta is limited by the chorionic plate, and on the maternal side by the main membrane, the decidua of which grows deeply into the placenta.
At the junction, trophoblast and decidual cells mix. This area is characterized by the presence of decidual and giant syncytial cells and rich intercellular amorphous substance. By this time, most cytotrophoblast cells have degenerated. Between the chorionic and decidual plates there are intervillous spaces filled with maternal blood. They develop from syncytiotrophoblast lacunae and are lined with syncytium of embryonic origin. The branches of the villi are located in the intervillous blood lacunae.
Over the course of 4-5 months, the membrane forms numerous partitions - decidual septa, which protrude into the intervillous spaces, but do not reach the chorionic plate. Such septa have a core of maternal tissue. But their surface is covered with a layer of syncytium, which separates the maternal blood in the intervillous lacunae from the fruiting tissue of the villi. Thanks to the development of septa, the placenta is divided into sections - cotyledon. Due to the fact that the decidual septa do not reach the chorionic plate, the intervillous spaces of different cotyledons maintain contact with each other.
Along with the growth of the fetus and the expansion of the uterus, the placenta grows. An increase in the surface area of the placenta occurs as the uterus enlarges; at the end of pregnancy, the placenta occupies about 15-30% of the internal surface of the uterus. The increase in the thickness of the placenta is due to the branching of existing villi, and not their subsequent penetration into the maternal tissue.