Magnetic resonance imaging has high tissue and fluid contrast. The procedure allows visualization of loose structures of the body without significant invasive manipulations. MRI is actively used in neurology and neurosurgery to diagnose diseases of the nervous system. Magnetic resonance scanning is considered the most informative method of studying the brain. According to the results of tomography, inflammatory, degenerative, dystrophic changes, and tumors are detected.
Colloid cyst on MRI
A brain cyst is a benign neoplasm inside the skull. It is a closed pathological formation with predominantly liquid contents. Congenital cysts appear when intrauterine development is disrupted; acquired ones can be the result of head trauma, infectious disease, cerebrovascular accidents and other conditions. The formations are not prone to malignant degeneration, but when they reach an impressive size they can compress surrounding structures. It is important to diagnose a cyst as early as possible and determine treatment tactics. MRI scanning allows you to identify and differentiate formations and track the dynamics of the process.
Indications for the study
The presence of a retrocerebellar cyst can be suspected by some characteristic symptoms:
- Severe headaches that do not go away even after taking painkillers;
- Unreasonable loss of consciousness or fainting state;
- Sensation of squeezing and pulsation in the head;
- Deterioration of hearing or vision;
- Arterial hypertension;
- Numbness of the limbs;
- Impaired coordination of movements;
- Epileptic seizures.
Magnetic resonance imaging is required if surgical intervention in the brain area is necessary.
Note that the clinical picture and severity of symptoms depend on the exact location and size of the retrocerebellar cyst.
Etiology and pathogenesis
The causes of a congenital cyst are unfavorable factors that occur during the development of the fetus. These are:
- fetal hypoxia during delivery;
- fetoplacental insufficiency;
- taking a specific group of medications by a pregnant woman;
- Rh conflict between mother and child;
- intrauterine infections.
Factors that provoke the development of a congenital cavity with fluid are drug, alcohol or nicotine addiction of the mother. In this case, the child’s development takes place under conditions of intrauterine intoxication, which negatively affects the brain structures. The causes of the cavity can also be chronic decompensated diseases of the expectant mother.
An acquired cavity with fluid in the head develops as a result of:
- inflammatory diseases (encephalitis, brain abscess, arachnoiditis, meningitis);
- traumatic brain injuries;
- injuries of newborns received during childbirth;
- cerebrovascular accidents (subarachnoid hemorrhage, ischemic stroke, hemorrhagic stroke).
Depending on the etiology, the following types of liquid cavities are distinguished:
- A cyst of iatrogenic origin forms as a complication after brain surgery.
- Parasitic - develops with paragonimiasis, cerebral form of taeniasis and echinococcosis.
A cavity with fluid can also replace cerebral tissue during degenerative and dystrophic processes in the head.
If a cyst is present, there are a number of factors that can trigger its growth. These include obstruction of venous outflow from the skull, strokes and other vascular disorders, as well as head injuries, hydrocephalus, and neuroinfections.
Contraindications
Magnetic resonance imaging is safe for the body only if all contraindications are excluded.
Magnetic resonance imaging is not recommended in the following cases:
Very often, to obtain more informative images, doctors prescribe additional contrast. In this case, you must ensure that there are no following contraindications:
- Pregnancy of any stage.
- Breastfeeding period.
- Kidney failure.
- Chronic liver diseases.
- Allergic reaction to components included in contrast agents.
Types of brain cysts and their symptoms
Arachnoid - occurs in almost 4% of the population. A cavity with fluid can be congenital or acquired. In the latter case, it develops in response to traumatic brain injury. The formation is localized on the surface of the brain in its membranes. The cavity is filled with cerebrospinal fluid.
In most cases, an arachnoid cyst does not make itself felt for quite a long time and is discovered by chance. Severe symptoms appear only if a large amount of fluid accumulates in the cavity. In this case, cerebrospinal fluid is produced by the cells lining the cavity.
With a sharp increase in the volume of the cavity with liquid, it can rupture and, as a result, die.
Colloid cysts are recorded in 15-20% of all cases of formations inside the ventricles of the brain. Most often it is localized above the foramen of Monroe in the anterior region of the 3rd ventricle. Less common in the area of the transparent cerebral septum in the 4th ventricle.
The liquid filling the cavity of the colloid cyst has high viscosity. Patients experience symptoms of hydrocephalus and, with a certain position of the head, a paroxysmal increase in cephalgia is noted.
In rare cases, memory loss, behavioral disorders and weakness in the limbs occur.
Pineal cyst of the pineal gland - according to statistics, 10% of patients have formations of this type that are small in size and do not make themselves felt. Cystic formations are localized in the epiphysis of the brain, in most cases they are no more than 1 cm in size. Otherwise, symptoms appear. When it grows, it can block the entrance to the “plumbing” of the brain and block the circulation of cerebrospinal fluid, causing occlusive hydrocephalus.
Epidermoid or dermoid is a formation that is an anomaly of intrauterine development. In this case, the cells of the baby's future skin and its appendages remain inside the brain. Accordingly, in addition to liquid, elements of the ectoderm are present, namely sebaceous glands and hair follicles.
After the birth of a child, such a cyst quickly increases in size. The only possible treatment is surgical removal of the formation.
Choroid plexus cyst - forms regardless of the person’s age. In this case, the space between the plexus vessels is filled with cerebrospinal fluid. Symptoms are rarely present, sometimes accompanied by epileptic seizures and symptoms of intracranial hypertension.
With a congenital choroid plexus cyst, the formation is diagnosed at the 20th week of intrauterine development using ultrasound. By the 28th week, such formations resolve.
Preparation rules
During a routine examination, doctors recommend following a few simple recommendations:
- If it is necessary to administer contrast, you must come to the clinic on an empty stomach, that is, do not eat food for 7-8 hours.
- If you are afraid of research or confined spaces, be sure to consult with a specialist. Your doctor may prescribe you sedatives to make the examination process more comfortable.
- Do not bring any metal products inside the tomograph. For this reason, doctors recommend removing metal accessories in advance.
- Prepare a change of clothes that do not have metal or metal-containing accessories.
- The duration of the diagnostic test is about 40 minutes. Empty your bladder in advance to avoid discomfort during the procedure.
General principles of therapy
Drug therapy for cystic formations has practically no results. The only possible treatment is surgical removal of the fluid cavity. But, most forms are small in size and remain in a “dormant” state for many years. In this case, no methods of therapy are used; a wait-and-see regimen is chosen and the patient is regularly examined.
Formations that are accompanied by symptoms of hydrocephalus, complicated by bleeding and rupture, compressing the brain and rapidly increasing in size must be removed. Only a neurosurgeon decides which method of surgical treatment to use.
If the patient has a disorder of consciousness (coma or stupor), he is urgently referred to external ventricular drainage. This method allows you to reduce compression of the brain by the cyst and intracranial pressure. If the cyst ruptures or hemorrhages, surgery is performed. The patient undergoes craniotomy and the formation is excised.
In the absence of complications and disturbances of consciousness, the operation is performed planned and endoscopically. The advantage is the patient’s quick recovery period and low trauma. With endoscopic access, a milling hole is made in the skull, through which fluid is sucked out from the cavity. In order to avoid subsequent accumulation of fluid, several holes are made in the cavity (connected to the cerebrospinal fluid space) or cystoperiotoneal shunting is performed (a special shunt is installed).
The postoperative period involves rehabilitation therapy, including exercise therapy, reflexology and massage. The patient is prescribed drugs to improve blood supply to the brain, absorbents and decongestants.
How is an MRI performed?
To ensure that the procedure is as informative as possible and that the images are clear, experts recommend performing magnetic resonance imaging in closed-type tomographs. Before starting the study, the patient must change into clothes without metal structures, take off his shoes and lie down on a retractable table. If the doctor has prescribed additional contrast enhancement, a special drug is injected into a vein, which is distributed throughout the circulatory system in just a few minutes. Then the table moves inside the tomograph, where the research process takes place.
Maintaining immobility is the main requirement for the patient! Remember that even minimal movements can lead to a decrease in the information content of the procedure.
It is also worth noting that when performing magnetic resonance imaging, a specific loud noise is observed. If this scares you, you can use earplugs.
Patients generally tolerate MRI well. Inside the tomograph there is good lighting and ventilation, there is a loudspeaker, as well as a panic button for emergency stop of the study.
Diagnostic measures
A neurologist may suspect the presence of an intracranial formation of significant size based on the patient’s neurological status and clinical symptoms. In this case, the patient is sent for examination to an ophthalmologist and otolaryngologist to check vision and hearing. Specialists perform ophthalmoscopy, audiometry, perimetry and visometry. With severe hydrocephalus, ophthalmoscopy reveals congested optic discs.
By referring the patient for echo-encephalography, it is possible to diagnose increased intracranial pressure. If the patient experiences epileptic paroxysms, he is additionally sent for electroencephalography.
It is extremely important to differentiate a cavity with fluid from a tumor, abscess and hematoma. It is not possible to do this on the basis of collected clinical data alone. Therefore, to make a clear diagnosis, neurologists use neuroimaging diagnostic methods.
By performing an ultrasound examination, it is possible to diagnose certain types of congenital cysts even at the stage of intrauterine development of the fetus. After birth, until the baby's large fontanelle closes, neurosonography is performed to make the correct diagnosis. In adulthood, to visualize a brain cyst, the patient is sent to a magnetic resonance or computed tomography scan of the head.
MRI and CT are performed with contrast in order to differentiate a cyst from a tumor. A cavity with liquid is not able to accumulate a contrast agent, unlike a tumor.
After diagnosis, constant monitoring of the patient with a cystic formation is important. During regular examinations, the doctor monitors the volume of the cyst over time.
If the cyst is a consequence of a stroke, additional vascular examinations are carried out: ultrasound, MRI and CT of vessels, duplex scanning.
MRI with contrast
In most cases, magnetic resonance imaging of the brain is performed with contrast, especially if any neoplasm is suspected. This makes it possible to examine the tumor in detail and distinguish a benign tumor from a malignant one.
The contrast agent clearly highlights the vessels, which allows you to see any tissue pathologies. Don't worry, contrast agents are safe for the human body. Most patients tolerate this procedure well. You must first consult a doctor and exclude all possible contraindications.
Classification
Classification by location:
- Cerebral (intracerebral). It is formed in areas of dead brain tissue in the internal structures of the brain.
- Arachnoid. It is formed as a result of the accumulation of cerebrospinal fluid in places of adhesions formed as a result of inflammatory processes and in places of their congenital duplication. The advantage is localized in the meninges.
The following types of brain cysts are distinguished separately:
- dermoid;
- colloidal;
- choroid plexus;
- pineal gland.
According to its genesis, a cavity with fluid can be congenital or acquired. In turn, congenital is divided into colloid and dermoid, and due to its formation into post-infectious, post-traumatic, post-stroke and echinococcal.
Decoding the results
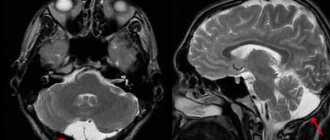
A retrocerebellar cyst is located in the brain behind the cerebellum, in the posterior cranial fossa. During magnetic resonance imaging, it is possible to clarify the exact location and size of the formation.
The report will contain all the information, but the MRI specialist cannot make a diagnosis - this must be done by your attending physician. If the diagnosis of retrocerebellar cyst is confirmed, the doctor will determine treatment tactics. For benign tumors, it is often possible to do without surgical interventions - they are required only in cases of large tumors or rapid growth. To avoid serious consequences, consult a doctor at the first alarming symptoms. Be healthy!
Is a brain cyst always a dangerous diagnosis?
The substance of the human brain is thin and delicate. Any foreign formation, be it a tumor or fluid, leads to disruption of the functioning of this organ, sometimes threatening the vital functions of the human body.
What is a brain cyst and how dangerous is it? Is surgery always necessary for a brain cyst or can it be done without surgery? These questions worry many. We will find out the answers to them from the executive director and chief physician of MRT Expert Lipetsk LLC, Oksana Egorovna Volkova.
— Oksana Egorovna, what is a brain cyst?
A cyst (translated from Greek as a bubble) is one of the most common pathological formations that can occur anywhere in our body. Indeed, the cyst is like a balloon filled with water, expanding as fluid enters.
This pathology actually appears quite often in the brain. If we talk specifically about a brain cyst, then more often it is a cavity filled with cerebrospinal fluid (CSF) washing the brain and spinal cord.
The symptoms of a brain cyst are very varied and depend on the location and compression of the area of the skull. However, over a long period of time, a bubble filled with fluid may not cause concern and can only be detected during an MRI of the brain.
You can sign up for a head MRI here
— How does a cyst differ from an abscess?
Abscesses on MRI look like large or small cysts, but are filled with purulent contents and surrounded by a zone of pronounced edema of the brain substance.
— What types of brain cysts are there and for what reasons do they occur?
Cysts are divided into congenital and acquired.
Congenital brain cysts are the result of a violation of the intrauterine development of the membranes of the brain. Most often, these types of cysts are localized in the temporal regions, in the posterior cranial fossa, the so-called pineal region (or pineal region). Intraventricular cysts are also congenital.
Acquired cysts are usually tumor cysts, and in this case the cyst is a “product” of tumor growth. The locations of such cysts are the lobes of the brain: frontal, temporal, parietal, occipital; cerebellar hemispheres.
Acquired cysts can also be post-traumatic in nature and occur after healing of areas of brain contusion.
Also in our practice, we encounter cysts that appear after strokes. In this case, transformation of the ischemic focus is noted. If the ischemic stroke was extensive and localized closer to the cortex, its outcome is cystic-glial changes, representing several small or large cysts, like a bunch of grapes. I note that such changes can also be a consequence of brain injuries, including in children.
What is the difference between ischemic and hemorrhagic stroke? Find out here
In some areas of our country, where a number of infectious diseases are endemic, parasitic cysts, for example, hydatid cysts, are common. Such cysts are filled with fluid, which is a waste product of this parasite.
— Are cystic-gliotic changes an accidental finding?
Yes, if a person suffered a stroke “on his feet”. Not long ago, a young patient came to our center and was treated for hypertension for three weeks. She complained of unsteady gait, dizziness, weakness, headaches and high blood pressure. The local doctor, deciding that the symptoms indicated a hypertensive crisis, prescribed appropriate treatment.
The patient made the decision to undergo an MRI of the brain on her own. We identified a fairly large area of recent cystic-gliotic changes, which allowed us to conclude that at the moment when the woman had a sharp increase in pressure, a stroke occurred. Consequently, the treatment tactics had to be different. The patient was saved from serious consequences by the fact that the stroke occurred in an area of the brain in which there are no vital centers. We can say that she was “born in a shirt.” But this doesn't always happen. Therefore, if you are not feeling well - your blood pressure is fluctuating, you are dizzy and have a headache, you are feeling weak - do not delay contacting the MRI diagnostic center. Based on symptoms alone, it is often difficult to make a correct diagnosis.
— What types of so-called “non-dangerous cysts” of the brain do doctors encounter most often?
We often find arachnoid cerebrospinal fluid cysts in our patients, as a variant of congenital formations. In the pictures we see that one of the brain lobes is larger than the other, and the free space is filled with cerebrospinal fluid. Such cysts appear due to the fact that during intrauterine development the brain was formed asymmetrically and do not entail any problems for human health.
I have met patients who were missing a fourth of their brain on one side. But at the same time, such an arachnoid cerebrospinal fluid cyst did not affect their well-being and mental activity in any way. This happens because the compensatory capabilities of the central nervous system are high. Therefore, it is not entirely correct to talk about the size that is normal for this type of cyst. From the case that I described, it is clear that even a huge arachnoid liquor cyst may not cause a person any discomfort, except headaches in case of increased intracranial pressure. Prescribing medications to normalize the outflow of cerebrospinal fluid helps such patients relieve headaches.
Epiphysis microcysts are another type of harmless cyst that is often detected during MRI studies. Their size is usually from 3 to 5 mm. If the formation is larger than the specified parameters, we recommend performing a contrast-enhanced MRI. This is necessary in order to exclude oncology.
When is the use of contrast in MRI necessary? Find out here
Large epiphysis cysts need to be observed dynamically; microcysts do not require such attention.
— What are the symptoms of brain cysts?
As for congenital ones, these are mainly “silent” cysts, which extremely rarely increase in size and lead to some kind of symptoms. This type of cyst does not pose any threat in terms of malignancy.
Secondary cysts can give symptoms, sometimes quite severe. More often these are headaches; if liquorodynamics are disturbed, there is nausea and vomiting, and focal convulsions may appear in the face, arm or leg. If the size of the cyst is so large that it leads to displacement of certain brain structures, this can lead to paresis, paralysis, and depression of consciousness.
How to relieve tension headaches? Find out here
- Can MRI determine the type of cyst?
MRI of the brain with intravenous contrast on a device with a power of at least 1.5 Tesla allows you to determine the type of cyst with high accuracy. Each type of cyst accumulates contrast agent in its own way.
— Is the diagnosis of “brain cyst” always an indication for surgery?
No. For congenital cysts that do not cause symptoms, surgery is not performed. These cysts are indicated for observation with MRI examinations every 6 or 12 months.
With acquired cysts, if we are talking about cystic forms of metastatic tumors, primary glial tumors, parasitic cysts or abscesses, the neurosurgeon often decides in favor of surgical intervention. And colloid cysts of the third ventricle are urgent situations requiring urgent surgical intervention.
— When performing surgery for brain cysts, is craniotomy always performed?
No. This depends on the location and type of cyst. For some types of cysts, cystoperitoneal shunting or microsurgical fenestration of the basal cisterns is indicated.
— Which specialty doctor should you consult if the diagnosis of “brain cyst” is indicated in the report after magnetic resonance imaging?
See a neurologist or neurosurgeon. As a rule, in recommendations, both written and oral, we indicate what specialization the patient needs to consult with a doctor.
In the photo: Volkova Oksana Egorovna
Other related articles:
What does an MRI of the pituitary gland show?
What is the difference between open and closed tomography?
MRI diagnostics for arachnoid cyst
Despite the fact that CT allows you to accurately determine the size and location of the cyst, MRI provides the most accurate and complete information about the formation. Typically, to diagnose an arachnoid cyst, an MRI scan is performed with the injection of contrast into the patient's bloodstream. At the same time, brain tumors tend to accumulate contrast, and cysts do not absorb it from the blood vessels, which is very clearly visible on MRI.
Also, MRI scanning allows you to distinguish a cyst from hemorrhages, hematomas, hygromas, abscesses and other diseases with similar symptoms. In addition, MRI makes it possible to identify a cyst even in cases where the patient does not yet have any symptoms, and the cyst itself measures only a few millimeters.
Get an MRI of the brain in St. Petersburg
Forecasts
In most cases, a frozen cavity with liquid of insignificant size does not bother the patient and does not cause any symptoms. In other cases, with adequate and timely treatment, the outcome is favorable.
In rare cases, patients after surgical removal of a cyst experience a residual moderate-to-severe liquor-hypertensive symptom. If a focal neurological deficit develops, it persists after treatment.
With the removal of the cyst, epileptic paroxysms disappear, but often appear later. This is justified by changes in the operated area of the head, in particular the formed adhesions. Secondary epilepsy is practically uncontrollable by anticonvulsant therapy.
Treatment methods for liquor cysts
The most common indications for surgical treatment of a cyst: it grows too quickly, causes seizures, causes neurological deficits, the cyst interferes with the child’s development.
The main, safest and most effective method for treating cerebrospinal fluid cysts today is fenestration. That is, dissection of the walls of the cyst for communication between the cyst and other cerebrospinal fluid spaces, where this accumulated fluid is normally located.
It is possible to install a stent (catheter) connecting the cavity of the cyst and the ventricles. It happens that the operation turns out to be ineffective and forces you to use another method of treatment - bypass surgery.
Shunt surgery (today practically not used as a primary method of treatment), although it allows you to quickly reduce the size of the cyst, but creates a lifelong dependence on the shunt system. If this method can be avoided, neurosurgeons try to avoid it.
However, when treating young children (up to two years old), as well as when treating cysts that were complicated by hemorrhage, shunt operations are inevitable.
In general, surgeries to treat cysts have a low risk of complications in the hands of experienced doctors. This operation involves hospitalization for only three to four days and several subsequent consultations with a surgeon. Deviations from this rule occur only in 10% of cases.
Most often, in such a situation, endoscopic surgery is used, but in some cases, an open microsurgical approach is more correct. An uninitiated person will not see the difference after the operation; the size of access to the brain cavity will be the same. In this case, it is not so important for the patient which instrument is used to perform this operation. It is important to make the patient feel better.