08/15/2018 A child at any age (including a one-year-old) can develop myopia. In older children (6, 8 and 10 years old), it usually appears due to high strain on the eyes due to school or prolonged use of the computer.
Recently, the disease has been rapidly growing younger, and therefore, in order to prevent its development in your child, you should take preventive measures in advance.
Congenital myopia is a rare phenomenon; in most cases, children are farsighted. For one possible reason, this disease is caused by abnormalities in intrauterine development.
Myopia in children can develop for the following reasons:
- Heredity - as a rule, if parents suffer from myopia, then children are at risk. The development of the disease is caused by insufficient development of the eye tissue, which stretches as the eye grows.
- Congenital abnormalities - pathologies of the lens or cornea are possible; congenital glaucoma can cause the development of myopia.
- High strain on the eyes - looking at moving objects for a long time causes severe eye strain in children, which can result in the development of myopia.
- Poor health – myopia can develop as a result of previous illnesses not related to vision. Therefore, it is important not to neglect existing diseases.
- Poor diet – lack of vitamins can be one of the main reasons for the development of myopia in children.
- An inconvenient workplace - poor lighting on a child’s desk, incorrectly selected furniture - can lead not only to poor posture, but also to the development of myopia.
Features of diagnosing myopia in preschool children
Congenital myopia in preschool children is extremely rare; in most cases it is acquired. In early childhood, it is difficult to suspect the disease, since the child is not able to understand that his vision is deteriorating and does not complain about its decline, and parents do not attach importance to the child’s changing behavior due to visual impairment. It is important to undergo regular examinations at an ophthalmological center; this is the only way to identify the disease and timely treat myopia in children with a weak degree, and not wait for progressive development.
High load on the visual system
Due to the anatomical feature of the eyes, when the gaze is focused on nearby objects, the child reflexively strains some parts of the visual apparatus. The longer and more often this process occurs, the more the eyeball is subject to changes in the form of growth.
That is why, with poor-quality lighting, incorrect distance of a book, notepad, gadget, monitor or small objects from the face, or prolonged time spent watching TV, additional strain on vision occurs. These factors provoke the occurrence of myopia. For example, an 8-year-old child’s eyes are subject to excessive fatigue because he studies at school for a long time during the day, then works on homework using a smartphone and computer, and can get carried away by watching TV.
Types of myopia
| According to the course of the disease: |
|
| By origin: |
|
| For reasons that determine the position of the main optical focus relative to the retina: |
|
| By severity: |
|
| According to the presence of complications: |
|
Regardless of the type of myopia, as it progresses, it is necessary to decide on surgical treatment to prevent further progression and the development of complications.
Drug treatment
To improve and maintain vision with myopia, the ophthalmologist may recommend drug treatment to the child using such means as:
- drops: “Irifrin”, “Emoxipin”, “Ujala”, etc.;
- group of drugs (drops) with atropine (0.01%);
- vitamin complexes.
If a child has been diagnosed with myopia, a comprehensive approach to treatment should be used. That is, the use of drugs is prescribed in parallel with wearing optics and performing hardware procedures.
How to treat myopia in children
Treatment of myopia in children is performed using the following methods:
- Hardware method. Hardware treatment is used to strengthen the eye muscles and also prevent further development of the disease.
- Drug therapy. Depending on the indications, the attending physician prescribes vitamin-mineral complexes for the eyes, drugs whose action is aimed at dilating blood vessels, calcium supplements, eye drops that act on the eye muscles.
- Physiotherapy. Physiotherapy methods for myopia in children include:
- vacuum massage;
- electrical stimulation;
- laser therapy;
- massage of the cervical-collar area;
- other
- Exercises for the eyes. Ophthalmologists have developed a larger number of different exercises that increase the chance of restoring vision, without the use of harsh treatment methods. In some cases, vision is completely restored or significant progress is achieved. The essence of the technique is to train weak muscles.
- Wearing correction devices (glasses, contact lenses, orthokeratology lenses)
Balanced diet
As already mentioned, vitamins, minerals and other beneficial microelements help maintain healthy vision and maintain its sharpness. This is why it is very important to enrich your child’s daily diet with foods that contain a variety of healthy foods. These include citrus fruits, black currants, apples, spinach, pork liver, cranberries, eggs, and fish oil. They contain vitamins A, B, C, lutein, anthocyanins, which increase immunity.
So, a balanced diet to maintain healthy vision may consist of:
- vegetables - sweet red or yellow peppers, beets, pumpkin, peas, fresh and sauerkraut;
- greens - dill, parsley, spinach, lettuce;
- bread - gray, black and with bran;
- soups - fish, vegetarian, dairy, cooked from lean meat;
- meat and fish - seafood, beef, poultry, rabbit, lamb;
- cereals - buckwheat, oatmeal, dark pasta;
- eggs;
- dried fruits - dried apricots, raisins, prunes, figs;
- fresh fruits and berries - blueberries, rowan berries, melons, apricots, oranges, tangerines, grapefruits;
- fermented milk products - cheese, cream, cottage cheese, kefir, yogurt without additives;
- vegetable fats - olive, mustard, linseed oil;
It is advisable to eat food in fractional parts 4-6 times a day.
Optics for children
Wearing glasses for myopia helps relieve eye strain and creates conditions for the proper development of the child’s visual organ. Depending on visual acuity, glasses can be prescribed only for distance (usually for low myopia) or for constant wear (for moderate and high myopia). According to indications, it is possible to prescribe soft contact lenses for children starting from school age, for example, if there is myopia in only one eye or with different degrees of myopia in the eyes and poor tolerance of glasses, when the child plays certain sports, if the child refuses to wear glasses, etc. In order to inhibit the progression of myopia, orthokeratological lenses (“night lenses”) are prescribed. In any case, the correct selection of correction means is carried out by an ophthalmologist after examining the child.
Pediatric ophthalmic surgery
Surgery is performed only if myopia progresses at a rate of more than 0.5 -1.0 diopters. per year, reached 3.5-4.0 D and higher, or if complications occur - dystrophic foci of the retina, which can lead to retinal detachment. In these cases, an operation is performed - scleroplasty. Its goal is to stabilize myopia by strengthening the posterior segment of the sclera of the eye and activating metabolism in the membranes of the eyeball.
In our department, surgical interventions are performed using various gentle techniques, using equipment and consumables that meet the strict standards of modern medicine.
Prevention and contraindications
Effective measures to prevent myopia:
- The correct mode of visual stress.
- Preventive examinations at least once a year.
- Proper organization of the workplace (lighting, table tilt, table and chair height, child seating)
- Proper diet.
- Regular eye exercises.
Important! If symptoms of myopia occur, immediately consult an ophthalmologist.
Violations of visual hygiene include significant eye strain, reading while lying down, playing on the phone or texting in a vehicle while moving, etc.
One of the most common diseases in children is myopia, or myopia. Most often it manifests itself during the school age of the child, which is usually associated with increased eye strain.
In the first year of life, myopia appears in 4-6% of children. Due to the growth of the eyeball, myopia is less common in preschoolers, but in children 11-13 years old, myopia is observed in 14% of cases.
Causes of myopia
Myopia can be congenital or acquired.
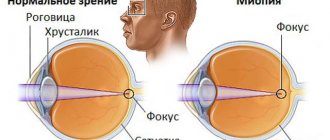
The immediate cause of the development of myopia is a violation of the proportion between the power of refraction (refraction) and the length of the anterior-posterior axis of the eye.
Due to a violation of the relationship between the size of the eye and refraction, the image of objects does not fall on the retina (as it should), but in front of it. Therefore this image will be blurry. And only negative lenses or bringing an object closer to the eye can produce an image on the retina, that is, a clear one.
Risk factors for the development of myopia are:
- heredity;
- fetal prematurity;
- congenital anomaly of the eyeball, lens or cornea;
- congenital glaucoma (increased intraocular pressure);
- increased visual stress;
- violations of visual hygiene;
- infectious diseases (including frequent acute respiratory viral infections, influenza, pneumonia);
- poor nutrition of the child;
- decreased immunity;
- some common diseases (diabetes mellitus, Down's disease, etc.).
The hereditary factor is of great importance for the development of myopia, but it is not the disease itself that is inherited, but the predisposition to it. Moreover, it increases significantly if both parents have myopia.
Congenital myopia may not progress if there is no hereditary predisposition (weakness or high extensibility of the sclera). But, as a rule, they are combined and lead to severe vision loss and constant progression. These irreversible changes in the eye can even cause disability. Myopia also develops in the case of a combination of glaucoma and scleral weakness.
In rare cases, infants have temporary, transient myopia. 90% of full-term children have “farsightedness with a margin” of 3-3.5 diopters. Farsightedness is therefore normal for children. This is due to the small size of the eye: the anterior-posterior axis of the eye in an infant is 17-18 mm, by 3 years it reaches 23 mm, in adults – 24 mm.
It can be seen that the greatest growth of the eyeball occurs before the age of 3, and its full formation is achieved at 9-10 years. During this period, the “reserve” of farsightedness is consumed, and eventually normal refraction is formed.
But if at birth there is farsightedness of 2.5 diopters (or less) or generally normal refraction, then the likelihood of the child developing myopia is very high: such a “reserve” is not enough for the eyeball to grow with age.
In premature babies, myopia develops in 30-50% of cases.
But still, more often children develop acquired myopia, which progresses during their school years.
This is facilitated by:
- significant strain on the eyes;
- posture disorders;
- improper organization of a workplace for a child;
- poor nutrition (lack of vitamins, magnesium, zinc and calcium);
- excessive passion for the computer and TV shows.
Some parents mistakenly believe that the glasses prescribed for their child contribute to the progression of myopia. This is wrong. Myopia will increase only with incorrectly selected glasses.
It is also a mistake to believe that myopia develops as a result of reading a large number of books. Myopia can be associated with reading only in the case of incorrect body position when reading or insufficient lighting.
Symptoms
A child with myopia has reduced visual acuity and finds it difficult to see distant objects.
The first sign of myopia in a child is a decrease in distance visual acuity, which causes the child to squint. Sometimes such visual impairment is temporary, transient, and reversible.
A symptom of myopia is also the rapid onset of eye fatigue when reading or when looking at any objects close up. Children may try to move their eyes closer to the text while reading or writing.
Myopia detected at this stage can be stopped, which is why it is so important to show the child to an ophthalmologist regularly, regardless of whether he or she has any complaints.
A divergent strabismus in a 6-month-old baby (or older) can also be a manifestation of myopia. In this case, consultation with an ophthalmologist is also necessary.
After a year, evidence of myopia may be the baby's frequent blinking and his desire to bring any object closer to his eyes for examination.
At school age, children may not see the text written on the board, but from the first desk they can see better. Near vision remains normal. Guys also notice rapid eye fatigue.
This condition can cause not only myopia, but also a spasm of accommodation (that is, a spasm of the intraocular muscles that regulate the refractive power of the eye). The spasm can be a manifestation of vegetative-vascular dystonia in a child, increased nervous excitability, or appear when the rules are violated while reading (insufficient lighting, incorrect posture, etc.).
The appearance of “floating spots” before the eyes may indicate a complication of myopia - destructive changes in the vitreous body.
There are the following types of myopia:
- physiological: appears during eye growth;
- pathological: is actually a myopic disease; differs from physiological myopia in its progressive course;
- lenticular: associated with high refractive power of the lens when it is damaged due to diabetes mellitus, congenital cataracts or exposure to certain medications.
According to the course, myopia can be non-progressive and progressive.
According to the severity of myopia, there are:
- weak (up to 3 diopters);
- medium (3-6 diopters);
- strong (above 6 diopters).
Diagnostics
- Survey of the child and parents: allows you to find out the presence of complaints and the timing of their appearance, the course of pregnancy and childbirth, previous and concomitant diseases, family or hereditary factors, changes in visual acuity over time, etc.
- Examination of the child includes:
- External examination of the eyes: makes it possible to determine the position and shape of the eyeballs;
- examination with an ophthalmoscope: determination of the shape and size of the cornea, assessment of the anterior chamber of the eye, lens and vitreous body, examination of the fundus; with myopia, a myopic cone is detected around the optic nerve head, atrophic changes in the fundus, pigmentation and hemorrhages, and even retinal detachment with high myopia may be observed;
- skiascopy (using an ophthalmoscope and a skiascope ruler) to determine the type of refraction and degree of myopia;
- Ultrasound helps determine the size of the anterior-posterior axis of the eye and identify the presence of complications;
Up to 3 years, only the named methods are used, but the results are compared with previous data (at 3 and 6 months).
From the age of 3, visual acuity is additionally checked using special tables. If visual acuity is reduced, lenses are selected to correct distance vision: this allows you to determine the degree of myopia.
It is possible to replace skiascopy with autorefractometry: after 5 days of atropinization of the eyes (instillation of atropine solution into the eyes), examination using a slit lamp. 2 weeks after atropinization, the necessary corrective lenses are re-determined.
Schoolchildren are at risk for developing myopia, so their visual acuity should be checked annually. Reduced visual acuity in them can be either a manifestation of myopia or a spasm of accommodation.
Therefore, re-determination of both visual acuity and refraction is carried out after 5 days of atropinization. In the case of spasm of accommodation, normal refraction and visual acuity are found. In this case, treatment is prescribed and examination by a neurologist is recommended.
In case of myopia, a repeated examination will again reveal an impairment of refraction and visual acuity, and correction is achieved only with the help of negative lenses. Myopia in schoolchildren is often weak or moderate. It usually does not progress and does not lead to complications.
But such children should be observed by an ophthalmologist every 6 months so as not to miss the progression of the process and the development of complications (atrophic changes in the retina and even retinal detachment). Therefore, the results of each subsequent inspection must be compared with previous data.
An increase in myopia by 0.5-1 diopter per year indicates a slow progression of the process, and more than 1 diopter indicates a rapid progression. It can lead to a sharp decrease and even complete loss of vision, irreversible complications in the retina (hemorrhages, tears, detachment, destructive changes). Typically progression occurs from 6 to 18 years of age.
Treatment
Correct selection of glasses and their constant use helps slow down the progression of the disease.
It is impossible to cure myopia in childhood. You can get rid of it after 18-20 years. Treatment depends on the degree of myopia, type (progressive or non-progressive), and existing complications.
Goals of treating myopia in childhood:
- slowing or stopping progression;
- prevention of complications;
- vision correction.
With progressive myopia, the sooner treatment begins, the greater the opportunity to preserve the child’s vision. An increase in myopia of less than 0.5 diopters per year is acceptable.
The following methods are used in the treatment of myopia:
- eye gymnastics;
- vision correction;
- orthokeratological method;
- drug treatment;
- physiotherapeutic treatment;
- general strengthening of the body and correction of postural disorders;
- surgical treatment.
At the initial stage of myopia development, daily exercises with special eye gymnastics, which will relieve eye tension and fatigue, have a good effect. There are many techniques to strengthen the intraocular muscle. An ophthalmologist will help you choose a specific set of exercises. Such exercises are not difficult; they should be performed at home at least 2 times a day. in a day.
Some doctors conduct ciliary muscle training in the eye office: negative and positive lenses are alternately inserted into special glasses.
For mild myopia, sometimes the doctor selects “relaxing” glasses with low-positive lenses. Computer programs are also used to relax accommodation at home.
Special laser vision glasses are also used. These perforated glasses are called “trainer glasses”: they provide the necessary load to weakened eye muscles and relaxation to overly tense ones. You need to use them for 30 minutes a day. They can also be used for preventive purposes for teenagers who spend a long time at the computer.
In order to correct vision, the ophthalmologist selects glasses for the child - a traditional and common method of correction. Although they do not have a therapeutic effect, you should encourage your child to wear glasses (or contact lenses for older children). Research by specialists in the USA and Europe shows that it is not wearing glasses that leads to the worst course of myopic disease.
Glasses not only create comfort for the child, but also reduce eye strain, which reduces the progression of the disease. In the case of congenital myopia, glasses should be prescribed as early as possible. For mild and moderate myopia, glasses are prescribed for distance vision only.
Constantly wearing glasses is necessary for high and progressive myopia. It is also necessary to wear glasses for divergent strabismus.
Wearing contact lenses is recommended for older children in the case of a significant (above 2 diopters) difference in refraction in both eyes, that is, in the case of anisometropia. The selection of lenses should be carried out by a specialist, since poor-quality optics and correction can aggravate myopia.
If you have myopia, you need to change your glasses in a timely manner, because excessive accommodation stress will contribute to the progression of myopia. The disadvantages of vision correction with glasses are: inconvenience when playing sports, limited peripheral vision, impaired spatial perception, and risk of injury.
Correction with lenses is more convenient, but the use of lenses is contraindicated in the event of infectious diseases. The disadvantage is also the possibility of injury to the eyes due to improper use or infection when putting on non-sterile lenses.
Currently, lens correction is used in night mode - the orthokeratological method, or corneal refractive therapy - the use of special lenses for 6-8 hours that cause a change in the shape of the cornea (flatten it) for up to 2 days. During this period, 100% vision is achieved without glasses. Lenses are used at night, during sleep, which is why this method is called night vision correction. Then the shape of the cornea is restored again.
The result of night correction is close to laser (changes the refractive power of the cornea) and differs only in the short duration of the effect, which is associated with the constant renewal of corneal cells.
A safe method of night correction can be used in children from 6 years of age. These special lenses not only completely relieve accommodation spasms in children, but also inhibit the development of myopia and its progression.
To reduce tension in the intraocular muscles, eye drops (usually Atropine) are sometimes prescribed for a 7-10 day course. But you should not use medication on your own. In addition, for mild myopia, vitamin complexes containing lutein can be used. For example, the dietary supplement “LUTEIN-COMPLEX® Children”, specially developed for eye health, is a multicomponent product that contains substances necessary for the normal functioning of the visual organs of a schoolchild from 7 years of age: lutein, zeaxanthin, lycopene, blueberry extract, taurine , vitamins A, C, E and zinc. A combination of biologically active components carefully selected taking into account the needs of the visual organs protects the child’s eyes, which is especially important to do starting from the age of 7, when the first serious visual stress begins in primary school, and reduces the risk of eye diseases.
To prevent complications and progression of the process, nicotinic acid, Trental, and calcium supplements are prescribed. For the initial manifestations of dystrophy, Emoxipin, Dicynon, and Ascorutin are used. In some cases, it is advisable to use absorbable drugs (Lidase, Fibrinolysin, Collalysin).
Of the physiotherapeutic methods, the use of Dibazol in the form of electrophoresis has a good effect. The so-called “myopic mixture” can be administered in the same way: Diphenhydramine, Novocaine and calcium chloride. In some cases, reflexology is effective.
Physiotherapeutic devices for treatment at home are also used to improve vision. Their operating principles are different: “massage of the pupil” (constriction and dilation), improvement of blood supply to eye tissue, electrical stimulation, magnetic therapy, ultrasound therapy, etc. Alternate treatment using various devices is possible.
One of the effective devices approved for use for children over 3 years old is called “Sidorenko Glasses”. The device combines the following methods of influencing the eye: pneumomassage, phonophoresis, color therapy and infrasound. It has no side effects, and in many children it allows one to avoid surgery for progressive myopia. The device is widely used in the complex treatment of children.
As a general strengthening treatment, it is recommended to adhere to a daily routine, dosage of visual stress (including regulated time watching TV programs and studying on the computer), a fortified balanced diet for the child, daily walks in the fresh air, and swimming. With a high degree of myopia, and even more so when complications arise, active sports (running, jumping, etc.) are contraindicated. Children with this pathology should be given a special set of exercises.
With rapid progression of myopia, scleral-strengthening injections and surgical treatment (scleroplasty) are recommended.
Indications for it are:
- myopia 4 diopters or more;
- rapid progression of the process (more than 1 diopter per year);
- rapid growth of the anterior-posterior axis of the eyeball;
- no complications from the fundus.
During the operation, the posterior pole of the eye is strengthened, preventing the eye from growing further. To improve blood supply to the sclera, 2 intervention options are possible: suturing a graft from donor sclera (silicone or collagen) or introducing a liquid suspension of crushed tissue behind the posterior pole of the eyeball. The operation does not lead to a cure, it only reduces the progression of the disease.
Laser vision correction is the safest type of surgery for myopia, which lasts about 60 seconds under local anesthesia, and provides a lifelong effect, eliminating the need to use glasses or contacts. But, unfortunately, such operations are contraindicated for children (under 18 years of age).
The best results for myopia are obtained by using all methods of conservative treatment in combination, and with rapid progression - in combination with surgery.
Forecast
Weak and moderate myopia in schoolchildren has a favorable course: it does not progress and does not cause complications, and is well corrected with glasses.
A high degree of myopia leads to decreased visual acuity even with lens correction.
Failure to correct myopia can lead to the development of divergent strabismus.
With progressive and congenital myopia, if complications arise, especially from the retina, the prognosis is unfavorable, and there is a significant decrease in visual acuity.
Prevention
From a very early age, you need to teach your child to follow a few simple rules when reading:
- the distance from the book to the eyes is at least 30 cm;
- ensure correct posture at the table;
- do not read while lying down;
- Read only in sufficient lighting.
Care should be taken to ensure that the table (desk) matches the child’s height. You should also pay attention to the chair: legs bent at the knees at an angle of 90 degrees should reach the floor. When reading, drawing and writing, the light should always fall on the left for a right-handed person and on the right for a left-handed person. Even in a children's playroom, good lighting should be provided.
Before starting school, you should consult an ophthalmologist and find out which desk your child should sit at and whether he needs vision correction.
You should limit your time watching TV and playing on the computer within reasonable limits. You should not watch TV in the dark.
A balanced diet and periodic use of vitamin complexes for the eyes will help not only in the treatment, but also in the prevention of myopia in children.
Summary for parents
Myopia in a child can lead to the development of a persistent decrease in visual acuity and serious complications. Much depends on timely vision correction and treatment. This is why it is so important to visit an ophthalmologist with your child every year (and for children at risk twice a year).
If myopia is detected, you must immediately follow all the doctor’s recommendations in order to prevent rapid progression of the disease and avoid surgical intervention.
There are several methods of conservative treatment of myopia. Even eye gymnastics can have a good effect if used regularly.
If a child is prescribed glasses, it is necessary to monitor the conformity of the lenses in them and change them in a timely manner.
Ophthalmologist of the 4th City Clinical Hospital named after. NOT. Savchenko
Kuropatkina Olga Arkadyevna
Surgical intervention
Surgical treatment of childhood myopia, as a rule, is not performed. There are various methods of refractive surgery that help correct ocular abnormalities in adults, for example scleroplasty, laser correction and others, but they are not applicable to children. In the vast majority of cases, this is due to the lack of a predictable result and the risk of various complications. Despite the proven effectiveness and safety of surgical treatments that restore vision, children are not prescribed them until they reach adulthood.