Brain edema is the body’s protective reaction to various types of injuries, hypothermia or infectious diseases. As a rule, the process of cerebral edema passes very quickly, the intercellular space and the cells themselves are filled with fluid, as a result of which the brain increases in volume, intracranial pressure increases, normal cerebral circulation is disrupted, and as a result, rapid death of brain cells begins. The outcome of the disease depends on the prompt and qualified provision of care to the patient.
General information
Cerebral edema is one of the manifestations of various critical conditions and is quite often encountered in clinical practice with various kinds of diseases and the development of pathologies. There are edema of the brain, spinal and bone marrow.
Brain swelling
Brain edema is an increase in its volume, caused by the accumulation of fluid in the intercellular space (interstitium) and accompanied by an increase in the volume of brain tissue. While an increase in brain volume due to intracellular fluid is defined by the term “swelling” of the brain. However, these processes (edema/swelling) can develop simultaneously and transform into each other, therefore both of these concepts can be defined as cerebral edema. ICD-10 cerebral edema code: G93.6
Edema syndrome develops as a nonspecific reaction of the body to the influence of many pathogenic factors. Possible in a number of diseases/pathological conditions that occur with damage to the nervous system - traumatic brain injury , acute cerebrovascular , infectious diseases, hypoxia , intoxication , brain tumors ( perifocal edema ), acute somatic diseases accompanied by impaired water-salt balance / hemodynamics, with endocrine disorders, blood diseases, after surgical interventions, exposure to ionizing radiation, etc. Brain edema is often one of the manifestations of critical conditions and the direct cause of death of the patient.
As a rule, cerebral edema at an early stage (with timely medical correction) is a reversible process, while with inadequate/late treatment, pathological processes increase and often end with the degeneration of brain nerve cells with disruption of their function and, in general, functional failure of brain structures.
Due to the accumulation of fluid in the interstitium of the brain, an increase in brain volume occurs in conditions of limited intracranial space with the development of mass effect (pathological effect of expanding tissue on neighboring structures, causing compression, deformation, displacement, atelectasis), which is primarily manifested by the development of intracranial hypertension (ICP) ) with a controlled increase in cerebral ischemia , and in severe cases - with displacement of brain structures and infringement of the stem sections in the tentorium of the cerebellum, accompanied by dysfunction of vital centers.
Spinal cord swelling
Most often, swelling of the spinal cord develops with traumatic injuries to the spine. Pathological disorders are formed both as a result of traumatic injury and compression of the spinal cord structures due to its edema-swelling, which is accompanied by ischemia of the brain substance, inflammatory changes and a high risk of developing irreversible disorders of the function/structure of the spinal cord. Compression of the spinal cord causes the formation of primary/secondary softening lesions in the spinal cord and is accompanied by neurological symptoms. Clinical manifestations are determined by the level of localization of edema, its severity and duration. With severe edema, it manifests itself as a syndrome of partial/complete disruption of spinal cord conduction.
Bone marrow edema (trabecular bone marrow edema)
There are subchondral and trabecular edema of the bone marrow. Trabecular edema - what is it? Spongy substance (syn. trabecular tissue) of bone consists of loose partitions/plates, the spaces between which are filled with bone marrow, which ensures hematopoiesis in the human body and the formation of immune chains. Edema of the spongy tissue is manifested by the accumulation of exudate (interstitial fluid) in the trabecular plates. At the same time, the liquid level increases from 10 to 20% or more. In most cases, the diagnosis is made late, since there are no specific symptoms and the disease is detected only on MRI.
According to the literature, bone marrow edema occurs more often in middle-aged patients and mainly affects large joints, the condyles of the tibia/femur. The most common (trabecular edema of the lateral condyle of the femur, bone marrow edema of the hip joints, bone marrow edema in the diaphysis of the radius, swelling of the condyle of the femur, etc.). Spinal bone marrow edema is much less common .
The causes of bone marrow edema are extremely diverse ( bruises / fractures , vitamin D deficiency , rheumatoid arthritis , osteoarthritis , benign / malignant tumors , osteomyelitis , spondylitis , arthrosis deformans , endocrine pathologies accompanied by impaired cellular metabolism, status epilepticus , acute neuroinfections , etc.) . The mechanisms of development of bone marrow edema are poorly understood. It is assumed that its development is facilitated by microvascular trauma, abnormal mechanical loads on bones/joints, metabolic disorders, and venous obstruction. Due to the small volume of the article, only cerebral edema will be considered.
Consequences of cerebral edema
As one of the critical conditions, cerebral edema very often ends in the death of the patient. The occurrence of edema marks either decompensated changes in the body of a general nature, or damage to brain tissue that is practically incompatible with life. All this makes cerebral edema an extremely unpredictable pathology, which may not respond to improvement with treatment. Among all the possible outcomes of cerebral edema, only three can be distinguished.
Progression of edema with transformation into brain swelling and death
A similar scenario, unfortunately, occurs in half of cases of cerebral edema of any origin. The danger of the situation is that as swelling progresses, a critical accumulation of fluid occurs in the brain tissue. This causes their pronounced swelling and increase in volume. As long as there is space in the cranial cavity to be filled with edematous cells, the condition of the patients remains relatively stable. But as soon as the free space is filled, compression of the brain occurs. As edema progresses, dense brain structures move into softer ones, which is called dislocation. Its typical variant is the wedging of the cerebellar tonsils into the brain stem, which ends in cessation of breathing and heartbeat.
Complete elimination of edema without consequences for the brain
This scenario is very rare and is possible only when cerebral edema occurs in young somatically healthy people due to intoxication with alcohol or other compounds toxic to the brain. If such patients are delivered on time to specialized toxicology or general intensive care units, and the dose of toxins turns out to be compatible with life, then the cerebral edema will be stopped and will not leave any pathological symptoms.
Elimination of cerebral edema with patient disability
The second most common outcome of this disease. Possible in patients with meningitis, meningoencephalitis of moderate severity, as well as with traumatic brain injuries in the form of small, timely diagnosed and operated on intracranial hematomas. Sometimes the neurological deficit is so minimal that it does not cause any visual manifestations.
Pathogenesis
The development of edema is initially based on microcirculatory disorders. Almost immediately after neuronal damage, regardless of its cause (hemorrhage, trauma, ischemia, tumor, inflammation), cytotoxic perifocal cerebral edema develops, and later, against its background, dysfunction of the capillary epithelium develops with accumulation of fluid in the interstitial space. In the development of endothelial dysfunction, several stages are distinguished, which are accompanied initially by functional (ion edema), then anatomical (vasogenic edema/hemorrhagic transformation) failure, as well as failure of the blood-brain barrier.
The development of cytotoxic edema is based on the accumulation of osmotically active substances inside cells (potassium/sodium/chlorine ions and glutamate molecules), which along the osmolarity gradient contribute to the movement of fluid from the interstitium into the intracellular space. That is, during this phase, cerebral edema is formed due to the trans-epithelial flow of sodium from the vascular bed, along with which chloride ions (to maintain electroneutrality) and water (to maintain osmoneutrality) move. At this stage, there is only a functional impairment of the permeability of the anatomically intact blood-brain barrier. At the same time, against this background, conditions are formed that contribute to the development of the next stages of cerebral edema (in particular, a drop in the concentration of interstitial sodium). The stage of cytotoxic edema does not lead to an increase in the volume of brain tissue and intracranial hypertension.
Developing vasogenic edema is characterized by more pronounced disturbances in the homeostasis of the interstitial space, which leads to disruption of the function/activity of neurons. As a result of increased permeability of the BBB, water accumulates in the intercellular space, which provokes the development of hypoxia and causes a malfunction of the cellular ion pumps of the brain, leading to the passive penetration of sodium ions into the cell, followed by water (the process of cell swelling).
The accumulation of fluid in a limited space according to the Monroe-Kelly formula leads to an increase in intracranial pressure , and in damaged glia (due to edema) the processes of exchange/capture of transmitter amino acids are disrupted. With the development of severe intracranial hypertension, it leads to displacement of the cerebral structures of the increased volume of the brain with herniation of the cerebellar tonsils/stem parts into the foramen magnum. And further compression of blood vessels further aggravates microcirculatory disorders/ischemia of brain cells. Dysfunction of the cardiovascular/respiratory/thermoregulatory centers located in the brain stem is a common cause of death.
As endothelial dysfunction progresses, it is accompanied by pronounced necrosis of epithelial cells and a sharp increase in the size of the intercellular space, which facilitates the passage of blood cells and leads to hemorrhagic saturation of brain tissue, which causes severe disruption of interstitial homeostasis, incompatible with the functioning of neurons and the development of hemorrhagic necrosis , which is associated with severe outcome of cerebral edema. The figure above shows the pathogenesis of cerebral edema.
Symptomatic manifestations of swelling
Typically, symptoms of acute edema in adults and children appear after the main signs of the underlying disease. They occur as swelling progresses and intracranial pressure increases. Before complications occur, the patient may experience:
- headaches, migraines, feeling of fullness in the head;
- anxiety;
- disorientation;
- nausea and vomiting;
- partial hearing impairment;
- increased blood pressure;
- arrhythmia, tachycardia, palpitations;
- drowsiness and lethargy;
- respiratory dysfunction.
Complete loss of vision is possible if the posterior cerebral artery is compressed. Possible signs of tendon loss and neck stiffness. The intensity of symptoms depends on the degree of swelling.
Nausea and vomiting usually result from increased blood pressure and migraines.
Symptoms may appear simultaneously or gradually. In severe cases, loss of consciousness and coma occurs. Cerebral edema and its consequences in such situations pose the greatest danger due to the uncertainty of the prognosis.
Classification
Due to the specific development of cerebral edema, 4 types are distinguished:
- Cytotoxic OGM - develops as a result of ischemia , hypoxia , exo/endogenous toxic effects on brain cells, causing changes in the permeability (osmoregulation) of cell membranes and dysfunction of glial cells (disorders of cellular metabolism). Cytotoxic edema is reversible within 6-8 hours due to reactivation of the ion pump, which is achieved by restoring cerebral blood flow.
- Vasogenic OGM is based on an increase in the permeability of the blood-brain barrier . Occurs perifocally in the area of ischemia , abscess , tumor, traumatic brain injury, surgery. The main role is played by the transition of fluid from the vessels to the white medulla. Due to the increase in capillary permeability, fluid partially passes from the vessels into the interstitial space), causing an increase in its volume.
- Osmotic OGM develops when the osmolarity of brain tissue increases without disrupting the blood-brain barrier. Occurs with metabolic encephalopathies , hypervolemia , drowning , inadequate hemodialysis and polydipsia .
- Interstitial OGM is the result of a rapid increase in ventricular pressure.
- It is formed when the walls of the cerebral ventricles sweat from the liquid part of the cerebrospinal fluid in the periventricular zone.
According to the degree of compensation there are:
- Compensated OGM (characterized by the absence of dislocation syndrome).
- Subcompensated OGM (characterized by the presence of dislocation syndrome in the absence of vital lesions of brain structures).
- Decompensated OGM (presence of dislocation syndrome and disturbances of vital functions).
The table below shows a general classification of OGM and characteristics of its forms.
Causes and risk factors
Swelling of the brain is associated with an increase in intracranial pressure, which normally should range from 3 to 15 mm. Hg Art. Minor fluctuations in indicators are possible during a person’s life.
Large changes are fraught with swelling. Among the main reasons for the appearance:
- infectious and inflammatory processes in the brain caused by meningitis, encephalitis, otitis, sinusitis, etc.;
- penetration of neurotropic poisons causing purulent-inflammatory processes;
- birth injuries, damage while in the womb, developmental defects (in a newborn child);
- previous surgical operations on the brain;
- strokes, heart attacks;
- withdrawal syndrome in alcoholism;
- anaphylactic reactions (allergy);
- progression of cysts and tumors that cause compression of the nerve and interfere with normal blood supply to tissues that promote fluid accumulation;
- renal or liver failure.
Among the risk factors that increase the likelihood of breast swelling are:
- severe somatic diseases;
- elderly age of the patient;
- the impossibility of surgical removal of tumors in vital systems;
- progression of metastases.
The mechanism of swelling formation is similar in all cases. It involves the accumulation of fluid in certain areas or throughout the entire volume of the brain matter. The rate of development of complications depends on the causes and prerequisites.
There are rare cases in which cerebral edema occurs in athletes involved in mountaineering and exposing the body to stress at high altitudes.
The progression of the pathological condition goes through several stages and begins with the gradual filling of the cells of the nervous tissue with fluid. As a result, it increases in size and increases the volume of the GM. The swollen brain begins to put pressure on the nerves and compress itself under the skull. This leads to complications, coma and death.
Causes
The causes of cerebral edema are quite numerous, according to which cerebral and extracerebral causes of AMS are distinguished.
Cerebral causes of cerebral edema:
- Brain injuries ( subdural hematoma , brain contusion , basal skull fracture , diffuse axonal injury , intracerebral hematoma ), brain surgery.
- Primary brain tumors ( glioma , medulloblastoma , astrocytoma , hemangioblastoma , etc.) or metastatic lesions of brain tissue that promote displacement of brain structures/disturb the process of outflow of cerebrospinal fluid.
- Cerebrovascular accidents - against the background of arterial hypertension (with a stroke of ischemic / hemorrhagic origin ) or systemic atherosclerosis .
- Neuroinfections ( encephalitis , bacterial meningitis ), purulent processes of the brain (for example, subdural empyema ).
Extracerebral causes:
- Infectious diseases ( influenza , scarlet fever , measles , scarlet fever , toxoplasmosis , mumps , etc.).
- Poisoning with drugs (quinine, antidepressants, neuroleptics, antihistamines, etc.) or various neurotoxic poisons (cyanides, phenols, gasoline, etc.).
- Radiation exposure.
- Development of an allergic reaction ( anaphylactic shock , Quincke's edema ).
- Encephalopathy due to liver/ renal failure , diabetes mellitus , alcohol poisoning.
- A sharp climb without the required acclimatization (mountain edema).
In newborns, cerebral edema can be caused by intracranial birth trauma, severe toxicosis of the pregnant woman, prolonged labor, or entanglement of the umbilical cord.
Diagnosis
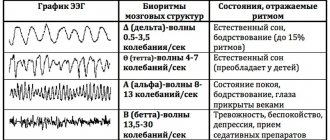
The diagnosis of general edema and swelling of the brain is based on clinical data and the results of additional research methods. The cardinal symptom of this process is an increase in intracranial pressure, which is diagnosed by measuring the pressure of the cerebrospinal fluid using tensiometric sensors, as well as on the basis of radiological signs of hypertensive changes in the bones of the skull, EEG data (the appearance of slow waves), and a slowdown in general cerebral circulation; reduction in the volume of the brain ventricles and subarachnoid spaces, detected by encephalo- or ventriculography (see Encephalography).
Local edema and swelling of the brain are diagnosed using echoencephalography (see), when the cut is determined by the displacement of the affected area of the brain; pneumoencephalo- or ventriculography, in which a displacement of the ventricular system in the opposite direction and possible deformations of the ventricle in the focal area are detected; angiography, in which a slowdown in local blood flow, displacement of the vessels of the affected area, and the appearance of a seemingly avascular area are observed in the cut; radioisotope scanning (see), based on the fact that certain isotopes (labeled albumin, 32P, etc.) accumulate in increased quantities in the area of edema and swelling of the brain. A particularly highly informative and largely differentiated understanding of edema and swelling of the brain, their relationship and dynamics of development is provided by the determination of the electrical impedance of brain tissue (see Impedance), carried out using deep electrodes and currents of a certain frequency.
Symptoms
Symptoms of cerebral edema in adults are extremely variable and are caused by dysfunction of various brain structures, disorders of metabolic processes/microcirculation and a developing increase in the volume of brain tissue, especially accompanied by displacement/herniation of certain brain structures, disruption of cerebrospinal fluid dynamics/blood flow in the vessels of the brain. The localization of edema in areas of the brain also plays a significant role, which determines its effect on specific brain structures and forms, in addition to general cerebral symptoms, focal neurological symptoms depending on the affected brain structures. Clinical symptoms of cerebral edema vary significantly depending on the stage of its development, according to which the following are distinguished.
General cerebral syndrome
Clinical signs at this stage are caused by an increase in ICP (intracranial pressure), and their manifestations/severity are determined by the rate of its increase.
headache appears vomiting may occur , often without preceding nausea. The intensity of pain after vomiting usually decreases. Transient dizziness . A common symptom is congested optic discs/transient episodes of visual impairment. Changes in the cardiovascular system are noted: bradycardia , increased systolic blood pressure, decreased breathing (the so-called “Cushing triad).” Characterized by slowly increasing changes in the psyche according to the type of disinhibition: irritability, anxiety, moodiness. Objective symptoms of intracranial hypertension with a slow increase in ICP are congestion of the veins/swelling of the optic disc, radiographically - thinning of the bones of the cranial vault, osteoporosis of the sella turcica.
With a rapid increase in ICP, severe pain of a paroxysmal/paroxysmal nature appears, often bursting pain, accompanied by vomiting, which does not bring relief with the subsequent development of coma . Bradycardia , oculomotor disorders appear Against the backdrop of ICP progression, mental inhibitions are noted, which is manifested by decreased memory, severe drowsiness , non-communication of the patient, and slower speech/thinking.
Syndrome of rostrocaudal diffuse increase in neurological symptoms
Clinical signs of cerebral edema at this stage are determined by the gradual involvement of certain brain structures in the pathological process. As a rule, the pathological process first involves the cortical, later the subcortical, and ultimately the structures of the brain stem. Edema of the cerebral hemispheres is characterized by impaired consciousness and the appearance of generalized clonic seizures.
The spread of the process to the subcortical/deep structures of the brain occurs with psychomotor agitation, the development of grasping/protective reflexes, hyperkinesis , and an increase in epileptic paroxysms .
When the pathological process moves to the hypothalamic region/upper parts of the brain stem, the degree of impairment of consciousness increases sharply, manifesting as coma / stupor with initial manifestations of impaired breathing and function of the cardiovascular system. A posture of decerebrate rigidity (installation of the limbs in an extension position). The convulsions are of a stem nature ( opisthotonus / hormetonia ), mydriasis (dilated pupils) with a sluggish reaction to light is noted.
Swelling of the tegmentum of the cerebral pons causes specific breathing disorders in the form of periodic breathing, maximum bilateral miosis (constriction of the pupils), truncal gaze paresis and leads to the disappearance of the oculovestibular/oculocephalic reflexes. As the edema moves to the medulla oblongata (lower part of the brainstem), disturbances in vital functions increase, which is manifested by a slower pulse/decreased blood pressure and breathing. Neurological examination reveals areflexia of deep reflexes , diffuse muscle hypotonia , lack of pupillary response to light, immobility of the eyeballs.
Phase of dislocation of brain structures
It is based on the process of dislocation and temporo-parietal/occipital herniation of brain structures, which is manifested by characteristic focal symptoms, the main of which are brainstem symptoms ( bradycardia , decerebrate rigidity , dysphagia etc.) with damage to the oculomotor nerves ( mydriasis , ptosis , divergent strabismus ). Often there is sudden vomiting, stiffness of the neck muscles, convulsions of the extensor muscles, lack of pupillary response to light, a decrease in body temperature, a decrease in heart rate and the development of life-threatening conditions - a sharp drop in blood pressure, depression of consciousness (coma), breathing disorders (cessation).
The particular danger of displacement/herniation of supratentorial structures is determined by the high risk of developing vascular disorders and occlusion of the cerebrospinal fluid outflow pathways, which sharply intensifies the primary pathological processes, which turn from potentially reversible disorders into irreversible ones.
Tests and diagnostics
Cerebral edema is an urgent condition that requires urgent medical care in a hospital setting (intensive care/resuscitation department), therefore, the initial diagnosis of acute brain injury should be as fast as possible and carried out during treatment. The primary guideline for diagnosing AGM is clinical symptoms, however, it must not be forgotten that at this stage they can be minimally pronounced. If OGM is suspected, a neurological/ophthalmological examination is carried out, during which pain, verbal-acoustic, behavioral reactions, ocular/pupillary reflexes, the condition of the optic nerve head, and intraocular pressure indicators are assessed. A clinical/biochemical blood test and lumbar puncture are required.
The main methods of instrumental diagnostics are computed tomography and nuclear resonance imaging, which allow one to visualize the localization/extension of the area of hyperhydration and identify signs of compression syndrome. According to indications, ultrasound of the skull in different projections, echoencephalography/electroencephalography, neuroophthalmoscopy, and cerebral angiography can be performed.
Differential diagnosis is carried out with thromboembolism of cerebral vessels , metabolic disorders , and status epilepticus .
Diet
Nutrition in the first 1-3 days of AGM is carried out parenterally, for which protein hydrolysates, glucose solutions, amino acids, plasma, albumin, a complex of vitamins, and special nutritional mixtures are administered. The timing of the start of enteral nutritional support through a tube is determined depending on the patient's condition, however, to restore gastrointestinal motility, it should begin as early as possible. For this purpose, special quickly digestible high-calorie nutritional mixtures are used, enriched with vitamins/microelements, a set of essential/essential amino acids in optimal dosages ( Nutrizon Energy , Nutrizon , Berlamin , Nutrizon Protein , etc.). It is recommended to use highly concentrated mixtures to reduce the volume of fluid administered, but at the same time provide the body with the necessary amount of calories. The patient can begin eating by mouth after regression of brain disorders.
Prevention
There is no specific prevention of cerebral edema, since it develops secondary. Among the general recommendations, we can only cite the need to follow some rules:
- Minimize the risk of head injury: use protective devices when moving (protective helmet when rollerblading/biking/skating, skiing; seat belts when driving in a car, do not jump your head into a body of water, etc.).
- Treat infectious/somatic diseases in a timely manner.
- Monitor your blood pressure .
- Lead a healthy lifestyle.
- When climbing to altitude (mountains), do not forget about the need to acclimatize to the altitude.
Consequences and complications
The consequences of cerebral edema, even in cases of rapid relief, can manifest as long-term consequences (absent-mindedness, disturbances in sleep/motor activity, communication abilities, depression). In severe cases, the consequences of cerebral edema can develop in the form of:
- decerebral syndrome (characterized by persistent extensor muscle rigidity, strabismus, severe mental defect);
- decortication syndrome (characterized by impairment/disappearance of speech, motor and mental skills;
- posthypoxic encephalopathy (characterized by dysfunction of the cortex with the development of a cerebral intellectual-mnestic defect).
The most severe complication is death from cerebral edema.
Consequences of a stroke
There are transient ischemic attack (less than a day), minor stroke (from 1 day to 3 weeks) and stroke with persistent residual effects. The consequences of a stroke are expressed mainly in motor and sensory disorders, the formation of muscle contractures (pronounced constant restriction of movements in the joints), speech and swallowing disorders. General symptoms may also remain, including confusion, disturbances in thinking, will, and emotional regulation. Complications can develop: from epilepsy to bedsores, encephalopathy and anxiety-depressive syndrome [1, 3].
Forecast
The prognosis for acute hypertension can vary significantly depending on its etiology, severity, localization, level of intracranial hypertension , and the presence of brain dislocation. Brain edema in the initial stage is a reversible process; as it increases, neuronal death/destruction of myelin fibers develops, leading to irreversible changes in brain structures.
However, even in surviving patients after cerebral edema, in the vast majority of cases there are residual effects, which can vary significantly from subtle manifestations in the form of increased intracranial pressure , frequent headaches , forgetfulness, irritability, absent-mindedness, depression , sleep disturbances, emotional disorders, slowness intellectual processes) to severe disorders of motor/cognitive functions, mental sphere, leading to the patient’s disability.
Severe complications develop especially often during stroke and coma . Accordingly, the prognosis for cerebral edema after a stroke, like the prognosis for coma, is disappointing, at best with disability due to impaired coordination/motor disorders and mental disorders, at worst the patient’s death occurs. Mortality rates for cervical edema, depending on the etiology and severity, vary between 35-70%.
List of sources
- Pavlenko, A.Yu. Cerebral edema: conceptual approaches to diagnosis and treatment / A.Yu. Pavlenko // Emergency Medicine. - 2007. - No. 2 (9). — P. 11-15.
- Principles and methods of diagnosis and intensive therapy of cerebral edema and swelling: method. recommendations / V.I. Cherny [and others]. - Donetsk, 2003. - 49 p.
- Slynko E.I. Traumatic injuries of the spine and spinal cord / E.I. Slynko, A.N. Honda. - K.: PP Gamma-Print, 2010. - 288 p.
- Martynov V.A., Zhdanovich L.G., Karaseva E.A., Ageeva K.A., Khasanova L.A. Edema-swelling of the brain: tactics of patient management // Infectious diseases: news, opinions, training. 2018. – T. 7. – No. 1. – S. 124-13.
- Zadvornov A.A., Golomidov A.V., Grigoriev E.V. Clinical pathophysiology of cerebral edema. Part 2 // Bulletin of anesthesiology and resuscitation. – 2021. – T. 14. – No. 4. – S. 52-60.
Pathological anatomy
Frontal section of the cerebral hemispheres during swelling: an increase in the volume of the left hemisphere, blurring of the boundaries between the white and gray matter, collapse of the lateral ventricles, more pronounced on the side of the swelling (indicated by arrows).
Macroscopically, edema and swelling of the brain are characterized by a number of signs: moisture and turbidity of the surface, an increase in volume, increased flabbiness (water content) of the brain matter, which has a yellowish-pink color, and unclear boundaries between the gray and white matter (Fig.). Due to the general increase in the volume of the brain, deep depressions are found in the area of the cerebellar hemispheres and protrusion of its tonsils, which is a morphological sign of strangulation of the stem sections in the foramen of the tentorium of the cerebellum. However, differences in the signs of edema and swelling are also noted. With predominant edema, there is plethora and swelling of the soft membrane of the brain, and a clear liquid drains from the surface along with blood. There is an increased amount of cerebrospinal fluid in the ventricles of the brain. On sections, the brain substance appears to be excessively moist, it can be easily cut with a knife, and clear liquid flows from the cut surface. With predominant swelling of the structural elements of the brain, the soft meninges, on the contrary, are dry, the brain substance is dense, the knife sticks to the cut surface. In the ventricles of the brain, cerebrospinal fluid is absent or contained in small quantities; the ventricles are slit-like.
Features of the microscopic picture are determined by the presence in the medulla of interstructural spaces filled with interstitial fluid, which occupy up to 10-15% of the organ’s volume. Electron microscopic data on the gapless fit of the structural elements of brain tissue and the predominantly intraglial nature of cerebral edema require correction. The possibility of rupture of astrocytic processes overloaded with fluid is also recognized by some supporters of the intrastructural theory of edema. Increased hydration of brain tissue under light microscopy is manifested by its loosening, more or less widespread dystrophic changes in the neurons of the cortex and subcortical centers, as well as the walls of intracerebral vessels, swelling of the myelin sheaths of nerve fibers with the formation of balloon-shaped swellings, dystrophic and proliferative changes in astrocytic neuroglia with phenomena of disintegration of processes ( clasmatodendrosis), hydropic transformation of hyperplastic oligodendroglia (especially along the brain capillaries), sometimes activation of microglia.
When pathomorphol. diagnostics must take into account a complex of macro- and microscopic signs, as well as their relationship with each other. The presence of individual signs, for example, expansion of the perivascular spaces, does not yet indicate edema and swelling of the brain, since it may be a consequence of the redistribution of tissue fluid without increasing its quantity. Therefore, the common term “perivascular cerebral edema” is relative. One of the reliable indicators of edema and swelling is a violation of the specific density of brain tissue. Edema and swelling of the brain can be predominantly local (perifocal) or diffuse. The process usually involves both gray and white matter, but according to some researchers, it predominates in white matter. It is not possible to clearly identify areas of brain tissue that are particularly susceptible (or resistant) to edema and swelling.