Home > Pain in the arm
This article will describe a condition such as epicondylitis of the elbow joint, symptoms and treatment of this pathology.
So, this is the most common disease associated with overload of the muscles of the forearm, which is often also called “tennis elbow.” However, repeated wrist extension occurs not only in tennis players, but also in ordinary people. Most patients with so-called “tennis elbow” have never held a racquet in their hands.
What happens inside with lateral epicondylitis?
Despite the fact that in the name we see the ending “-itis”, which refers us to inflammation, in fact, during microscopy of damaged tendons, no signs of an inflammatory reaction were found. Rather, the phenomena of degeneration of even and smooth tendon fibers into a shapeless collagen mass are revealed.
The fact is that the proximal part of the tendon fibers has a very poor blood supply, especially at the site of attachment to the bone. The main mechanism of damage is considered to be microtrauma, which, in conditions of insufficient oxygen supply, leads to degenerative changes in the structure of the tendons. Most often, these changes are found in the extensor radialis brevis tendon 1-2 cm distal to the site of attachment to the lateral epicondyle of the humerus. Since the localization of pain is in the elbow area, the condition is called “lateral epicondylitis,” although movements and stress on the elbow itself are usually painless.
Causes of medial epicondylitis of the elbow joint
Excessive stress on the muscles and tendons of the forearm is the most common cause of epicondylitis. Certain types of activities (occupational) can cause inflammation in the area where the muscles attach to the epicondyle. This activity does not have to be related to sports activities.
In some cases, the symptoms of ulnar epicondylitis are not associated with inflammation.
Instead of inflammatory cells, the body produces a type of cell called fibroblasts. When this happens, collagen loses its strength. It becomes brittle and can break. Every time collagen breaks down, the body reacts by forming scar tissue in the tendon. Eventually, the tendon thickens with additional scar tissue.
Small tears form in the tendons of the forearm, which are regenerated by scar tissue. Scar tissue does not have such strength and cannot completely restore the structure of the tendon part.
Who may have external or internal epicondylitis of the elbow joint?
According to statistics, men suffer from elbow pain no less often than women.
Most often these are middle-aged people from 35 to 54 years old.
Not everyone associates the onset of symptoms with unusual or excessive exercise. It happens that epicondylitis begins on its own without any obvious cause. The truth is that we don't really know why this pathology occurs.
In addition to the lateral (also known as external), there is also medial (also known as internal) epicondylitis of the elbow joint. It occurs in 10-20% (according to different authors) of cases of all epicondylitis. The only difference is that the pain appears not from the outside, but from the inside of the elbow joint, since the extensors of the wrist are involved in this process, not the flexors.
Medial epicondylitis of the elbow joint is also called “golfer’s elbow,” but golfers in our latitudes are even less common than tennis players.
Lateral and medial epicondylitis - treatment
In the treatment of epicondylitis
Prescribe rest for muscles whose tendon tension is accompanied by the appearance or intensification of pain. In case of severe pain, a plaster cast is applied for 3-4 weeks, and anti-inflammatory and analgesic medications are prescribed (butadione, ortofen, indomethacin, etc.). A course of physiotherapeutic treatment is carried out - electrophoresis of a novocaine solution, amplipulse therapy, hydrocortisone phonophoresis, etc. Laser therapy and cryotherapy are used to relieve pain. In some cases, reflexology is effective. A good therapeutic effect is achieved by a combination of local cooling (irrigation of the painful area with a refrigerant, for example chlorethyl) with the introduction of a local anesthetic (novocaine, lidocaine, etc.) or hydrocortisone to the point of maximum pain.
Professional medical equipment and devices for sports rehabilitation medicine ESMA.
The photo shows the following models of devices: Computer medical device - complex ESMA 12SK CAVALER Myostimulator ESMA 12.20 COMBI
ESMA devices cosmetology ESMA devices therapy ESMA devices sports medicine, fitness
Diagnosis of epicondylitis
In most cases, questioning and inspection are sufficient.
As a rule, the appearance of the hand does not change, with rare exceptions you may notice a slight swelling or change in skin color (this is more likely from repeated injections with glucocorticoids).
The most characteristic symptom of epicondylitis is pain in the area of the protruding epicondyle of the humerus - these are the bones on the sides of the elbow joint, on the outside and on the inside.
The pain intensifies with load on the arm. For lateral epicondylitis of the elbow joint, this is extension at the wrist, for medial epicondylitis, this is flexion. Also painful will be shaking hands, carrying heavy objects (kettle, pan), all movements that require a strong grip. For example, pull-ups or barbell presses can be painful, while push-ups do not cause any pain. This is because the muscles involved work specifically in the wrist, and not in the elbow.
The range of motion may be painful in extreme positions, this is especially noticeable with severe symptoms.
If in doubt, the doctor may prescribe additional tests: X-ray, MRI, CT, electroneuromyography.
Treatment of epicondylitis
Treatment of epicondylitis is mainly conservative: the use of orthoses during an exacerbation and at night, shock wave therapy, ultrasound therapy or galvanization, sometimes local administration of corticosteroids, drug treatment (NSAIDs).
In addition, exercise therapy is necessary to restore function (gradually increasing the load on the forearm). Conservative treatment methods are effective in 90% of cases. If there is no effect from conservative treatment within 3-6 months, surgical treatment is recommended.
Prevention
Preventive measures are quite simple, however, many people neglect them. Before starting sports training, a full warm-up is necessary so as not to load unheated muscles. A light massage is helpful. Strength training is indicated to strengthen the elbow tendons. People who are at risk due to their profession need to promptly and correctly treat chronic infections that can cause complications in the form of epicondylitis. For proper functioning of the ligaments, it is recommended to take a B complex of vitamins and vitamin C.
Epicondylitis of the elbow joint: symptoms and treatment
Epicondylitis of the elbow is a condition caused by swelling of the tendons. It is accompanied by acute pain and makes it impossible to move the arm freely.
These tendons are bands of tough tissue that connect the muscles in the lower arm to the bone. This is the most common reason why people go to the doctor with painful forearm symptoms. The disease can appear in people of any age, but most often occurs around the age of 40.
We will talk about what causes inflammation, how this disease is diagnosed and treated, in this article.
Medial epicondylitis: signs
Medial epicondylitis (golfer's elbow) is a type of tendinitis that affects the inside of the elbow. The disease develops where the tendons in the forearm muscle connect to the bony part on the inside of the elbow.
Tendons attach muscles to bones. Due to injury or irritation, they may become swollen and painful.
Although medial epicondylitis is called golfer's elbow, it does not only affect golfers. This can occur from any activity that involves using the hands or wrists, including tennis and baseball. It got its name because it is in this sport that the greatest stress is placed on the inside of the elbow.
Medial epicondylitis is much less common than lateral epicondylitis (tennis elbow), with the former accounting for only 9 to 20% of all epicondylitis diagnoses. Golfer's elbow occurs as a result of the high-energy tension created by an overhead shot. In sports, this phenomenon occurs frequently in tennis, bowling, archery, weightlifting, javelin throwing, racquetball and American football.
However, from 90 to 95% of all cases, the disease is not associated with sports training.
Because chronic repetitive contractile loading of the carpi flexor and pronator muscles is the most common etiology, occupations such as carpentry, plumbing, and butchering may also cause inflammation. The pathology can also be caused by sudden tension in these tendons.
In many cases, an injury at work is the cause of symptoms.
More specific occupational factors associated with medial epicondylitis are forceful activities in men and repetitive hand movements in women. Smokers and people with type 2 diabetes are at risk.
Medial epicondylitis may occur suddenly or develop slowly over a period of time. Symptoms can range from mild to severe.
The person experiences the following symptoms:
- pain inside the elbow;
- elbow stiffness;
- weakness of the hands and wrists;
- tingling sensation or numbness in the fingers, especially the ring and little fingers;
- difficulty moving the elbow.
It is not uncommon for pain in the elbow to radiate down the arm to the wrist. This makes it difficult to perform everyday activities such as picking up objects, opening a door, or shaking hands. Typically, medial epicondylitis affects the dominant hand.
Symptoms in both tennis and golfer's elbow usually begin gradually and get worse over time.
The condition can be caused by excessive force used to bend the wrist toward the palm.
During professional activities (playing tennis, baseball), this can happen when swinging a stick or bat.
Other possible causes include:
- undeveloped playing technique;
- weak shoulder and wrist muscles;
- sudden lifting of a suitcase (any load);
- Using a tennis racket that is too heavy or too short.
Despite the “sports” name, tendon inflammation can occur in any person when performing everyday tasks: carrying heavy or bulky objects, throwing a projectile, chopping wood, operating a chain saw.
What are the causes of medial epicondylitis?
Medial epicondylitis is caused by repetitive movements, which is why the condition is most common in athletes.
Golfers can develop this type of tendonitis from repeatedly swinging a golf club, while tennis players can develop it from repeatedly using their arms to swing a tennis racket. In both cases, overuse of the hands and wrists damages the tendons and causes pain, stiffness and weakness.
Other risk factors for this type of inflammation include playing baseball or softball, rowing, and weightlifting. Activities such as playing an instrument and typing on a computer can also lead to pathology.
Symptoms of this disease are similar but occur on the inside of the arm and include:
- pain inside the elbow;
- discomfort spreads down the arm from inside the elbow;
- weakness in the hand or wrist;
- numbness or tingling in the little fingers
- pain when gripping and bending the wrist.
Most cases of golfer's elbow are not caused by inflammation. Rather, it is a problem in the tendon cells. With increased cell release and calcification, the tendons begin to lose their elasticity (collagen loses its strength). This leads to tendon fragility and ruptures.
Improper technique while playing can cause damage
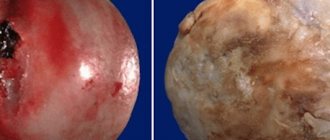
Every time collagen breaks down, the body reacts by forming scar tissue into the tendon. Over time, the tendon thickens with excess scar tissue. The tendon varies from a white, shiny and hard surface to a dull, slightly brown and soft surface.
Since the medial epicondylitis is a flexor group tendon attached to the humerus, the most sensitive area will be located near the origin of the carpi flexor group.
Lateral epicondylitis: what is the cause?
Tennis elbow (lateral epicondylitis) is a painful condition that occurs when the tendons in the elbow are overused. This usually occurs due to overload and frequent repetition of the same movement.
Despite the name, athletes are not the only ones who can experience this pathology. People whose profession involves working with their hands (carpenters, plumbers, builders) often turn to doctors with a similar problem. The pain occurs primarily where the forearm muscle tendons attach to the bony lump on the outside of the elbow. The pain may also spread to the forearm and wrist.
The following symptoms are typical for this condition:
- sharp or aching pain in the elbow;
- discomfort during a handshake;
- problems with grasping an object.
With severe inflammation of the elbow joint, the patient may experience pain from holding a coffee cup in his hand or when turning a doorknob.
This condition indicates that you should consult a doctor immediately.
Rest and over-the-counter pain relievers help relieve the condition, but do not cure it. If the conservative method does not help, the doctor may suggest surgery.
Risk factors
- Age. People aged 30 to 50 years most often turn to a specialist with a similar problem.
- Professional activity. People who have jobs that involve repetitive movements of the wrist and hand are more likely to develop this condition. Examples include plumbers, painters, carpenters, butchers and chefs.
- Certain sports. Participation in racquet sports increases the risk of tennis elbow, especially if the person has poor hitting technique.
Diagnosis and treatment
Fortunately, in most cases, both types of elbow inflammation respond well to conservative treatment.
Surgery is usually not required, although full recovery may take weeks or even months, depending on the severity of the condition. As with other forms of tendinitis, the most important aspect of treatment is to reduce the stress on the affected tendons. This may include resting the arm, using a brace or a tourniquet.
After recovery, it is mandatory for athletes to correct incorrect technique to prevent recurrence of the injury.
If elbow pain does not go away within 2-3 days, you should immediately consult a doctor.
The specialist will ask questions about your symptoms, pain level, medical history, and any recent injuries. During the consultation, you should provide information about daily activities, including work responsibilities, hobbies, and recreational activities.
The doctor performs a standard external examination, which may include applying pressure to the elbow, wrist, and fingers to check for stiffness or discomfort.
Before diagnosing medial epicondylitis, your doctor may order x-rays of the inside of your elbow, arm, or wrist to rule out other possible causes of pain, such as a fracture or arthritis.
When making a diagnosis, a specialist takes into account many factors: professional, household, degree of pain and development of the disease. If there was a history of injury to the shoulder or elbow, it is necessary to mention this. There are cases when inflammation appears several months after the tendon is damaged.
You should also tell your doctor if you have a history of rheumatoid arthritis or nerve disease. These factors will help to correctly diagnose the disease and prescribe a competent course of therapy.
During the examination, the doctor uses various tests to accurately determine the diagnosis. For example, the specialist may ask to straighten the wrist and fingers against resistance while keeping the arm fully extended to see if this causes pain.
If the reaction is positive, the specialist can determine muscle damage.
To rule out the possibility of another diagnosis, your doctor may recommend additional tests:
- X-rays. These tests provide clear images of dense structures such as bones. This test can help rule out elbow arthritis.
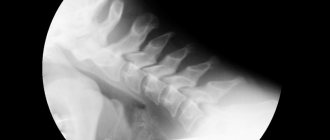
- Magnetic resonance imaging (MRI). If your specialist suspects your symptoms are related to a neck problem, an MRI may be ordered. Tomography shows details of soft tissues and helps determine the presence of a herniated disc or arthritis in the neck. Both of these factors can cause pain.
- Electromyography (EMG). The analysis helps to exclude compression of the nerve. Many nerves are concentrated around the elbow, and the symptoms of nerve compression are similar.
Given the painful symptoms, this disease requires immediate diagnosis and treatment.
Delayed therapy can cause a chronic condition. In this case, the slightest injury or careless movement of the shoulder joint may return the painful condition in the future.
Treatment of the elbow joint
Doctors classify two types of therapy for epicondylitis: surgical and conservative.
Approximately 80% to 95% of patients are treated successfully with non-surgical methods.
- The first priority is to rest your hand. This means that it is necessary to completely stop participating in training, competitions, and put off hard work for several weeks.
- Anti-inflammatory drugs. These medications reduce pain and swelling.
- Physiotherapy. Specific exercises are useful for strengthening the forearm muscles. The therapist may also perform ultrasound, ice massage, or muscle stimulating techniques to promote muscle healing. The technique is prescribed after a complete examination and diagnosis of the degree of inflammation of the joints.
- Using a bandage. The bandage is applied to the center of the back of the forearm. This method helps to immobilize the hand, giving the necessary rest, and significantly relieves pain.
- Steroid injections. Steroids such as cortisone are very effective anti-inflammatory agents. A specialist may prescribe a course of such injections to relieve pain.
- Extracorporeal shock wave therapy. Shockwave therapy sends sound waves into the elbow, where they create a “microtrauma.” This promotes the body's natural healing processes. Shock wave therapy is still considered experimental, but today studies show its effectiveness.
Also, if you are injured during sports games or training, prevention is important. A specialist may advise checking the equipment to ensure it fits correctly in your hand.
Stiffer racquets and more flexible racquets can often reduce the stress on the forearm. If you are using the wrong size racquet, switching to a smaller head size may help prevent symptoms from recurring.
Treatment methods for epicondylitis:
Surgical intervention
1. Open surgery (excision of the area)
2. Arthroscopic surgery (through a puncture)
Non-surgical therapy
Drug treatment
2. Physiotherapy
3. Massage
4. Physical therapy
Surgery
If painful symptoms do not go away after 6-12 months of general therapy, the doctor may give a referral for surgery.
Most surgical procedures for epicondylitis involve removing the affected muscle and rebuilding the healthy muscle back to the bone.
The correct surgical approach depends on a number of factors:
- extent of injury;
- previous therapy;
- state;
- activity.
Before surgery, you should consider all possible risks associated with surgery and evaluate the need for such treatment.
Surgical intervention can take two forms: open and superficial.
The most common approach to tendon repair is open surgery. The operation involves an incision above the elbow.
The open method is usually performed quickly and does not require long-term rehabilitation. The patient does not even need an overnight hospital stay.
Arthroscopic surgery.
Inflammation can also be treated using miniature instruments and small incisions. Like open surgery, it is a one-day or outpatient procedure.
This therapy has recently gained great popularity as it minimizes the risk of surgery and does not require long recovery.
The surgeon will mark the elbow joint before the procedure. To do this, the patient's elbow is bent at an angle of 90 degrees.
The procedure is performed using two methods: in supination or pronation position.
In the first case, the patient lies on his back, and the arm is moved to the side. In the pronation position, the patient lies on his stomach, the hand is fixed in a special way through a suspension device. The operation is performed on the elbow joint, bent at a 90-degree angle.
A tourniquet is pulled onto the upper forearm with a maximum pressure of 250 mmHg. The first stage involves filling the joint with a special saline solution through a lateral approach. This allows the nerve fibers to be displaced to prevent damage. Next, the surgeon carefully inserts the needle into the muscle of the joint capsule.
Possible risks:
- infection;
- loss of strength;
- loss of flexibility;
- long recovery;
- damage to nerves and blood vessels;
- need for further surgery
Postoperative rehabilitation
After the intervention, it is very important to immobilize the arm so that there is no load on it at all. The specialist applies a splint, which is removed after 6-7 days.
The specialist shows a special training for stretching the elbow and restoring flexibility. Light exercises with gradual strengthening begin 2 months after surgery.
Returning to professional activities and sports training is an individual matter. And in each individual case, the expert gives his recommendations, depending on the type of operation, the severity of inflammation and the effect of rehabilitation. This is usually 4 to 6 months after surgery. Tennis elbow surgery is considered successful in 80-90% of patients.
Treatment with folk remedies
Alternative treatment allows you to relieve pain symptoms and relieve the main tension from the tendons. However, none of the methods is a panacea and if symptoms recur, you should consult a doctor for professional medical treatment.
- Ice – Depending on the severity of the tendinitis, icing the affected area may help reduce pain and inflammation. Ice should be applied immediately when pain flares up. A tourniquet can be used for fixation. Experts recommend doing this for 20-30 minutes every 3-4 hours for 2-3 days or until the pain goes away.
- Anti-inflammatory drugs (Ibuprofen, Naproxen) are recommended in the early stages of inflammation. They help reduce discomfort, but do not cure the problem.
- Stretching exercises – Exercises that stretch the involved forearm muscles can help relieve stress on sore tendons.
- Using an elbow strap to protect the injured tendon from further stress.
- Massage. Any manual procedures can be performed only after acute inflammation has been relieved, otherwise any pressure may aggravate the situation. A competent massage helps restore tendons, helps strengthen muscle tissue, and prevents atrophy.
Manual therapy
- The use of compresses to relieve swelling and inflammation. This ointment-based compress can be easily prepared at home. An effective method is a blue clay compress (the powder is diluted in a 1:1 ratio with warm water).
An application of ointment based on horse sorrel root and vodka shows good effectiveness.
In case of severe pain, doctors recommend applying a compress with camphor alcohol or vodka. This method helps relieve swelling and inflammation.
For minor tendinitis, you can do an iodine grid and rest your arm.
Conclusion
Symptoms for both tennis and golfer's elbow usually begin gradually and get worse over time.
Both conditions are types of tendonitis, or inflammation of the tendon, and both are usually caused by excessive repetition of the same movement. This may occur due to overuse on a regular basis (such as hitting a golf or tennis ball) or other repetitive activities that use the forearm muscles.
Over time, tendons can go from inflamed to ruptured. Therefore, when primary symptoms appear, it is important to immediately seek medical help.
Types of disease
The disease is classified depending on the location of the inflammatory processes and their severity. The following types of illness are distinguished.
- External or lateral epicondylitis - the inflammatory process mainly spreads along the outer part of the elbow. This type of disease is also called “tennis elbow” because typical for professional tennis players. When performing grasping movements, carrying or lifting objects, there is a disturbance in the movement of the hands, which is accompanied by painful pressing sensations over the bones that enter the joint area.
- Internal or medial epicondylitis - localization of the inflammatory process occurs along the inside of the elbow joint. A person experiences discomfort in this area.
- Inflammation of the posterior area of the elbow - characteristic is the development of bursitis and damage to the mucous membrane of the bursa.
Diagnostics
The basis of diagnosis for suspected epicondylitis is a thorough examination by a doctor and the presence of clinical manifestations of the disease. When compiling an anamnesis, it is imperative to find out the patient’s professional activity and his regular additional activities (for example, playing sports).
Changes in the elbow joint can only be detected as a result of a long course of the disease. In some cases, the doctor prescribes an x-ray or computed tomography to accurately diagnose epicondylitis. No laboratory tests are required for diagnosis.
Exercises for epicondylitis
Therapeutic exercises help restore the functionality of the joint. You can start it only after the acute stage of the disease has subsided. The exercise therapy complex must be compiled by the attending physician. Basic exercises are aimed at stretching and relaxing muscles and tendons.
When doing gymnastics, you must adhere to the following rules:
- Increase the load and duration of classes gradually;
- Stop doing exercises immediately if acute pain occurs, as they should not cause pain;
- Do exercises daily.
Exercise therapy improves blood circulation, stimulates lymph flow and the secretion of synovial fluid, increases the elasticity of ligaments and strengthens muscles, which generally increases the endurance of the elbow joint.
Exercises recommended for epicondylitis are divided into active and passive movements performed with the other, healthy hand.
Passive movements:
- Grasp the other arm with your healthy hand and slowly bend it until a feeling of tension appears in the elbow area, trying to ensure that the angle between the hand and forearm is 90 ° C. Stay at the extreme point for 10-15 seconds. Do two sets of 7-10 times. Repeat the same exercise, extending the hand (that is, moving it upward).
- Standing, place both palms in front of you on the table. Lean forward slightly so that your palms form a right angle with your forearms.
- Place your hands on the table with the back surface (palms up), fingers pointing towards you, elbows slightly bent. Also try to create a right angle between your hands and forearms by leaning slightly away from the table.
After stretching exercises no longer cause any discomfort, you can move on to exercises aimed at strengthening muscles and ligaments.
Active movements:
- Alternately move the free hand to the position of pronation and supination, with the palm first looking down, then up;
- Consistently bend and straighten the forearm, while the shoulder remains motionless;
- Bend your arm at the elbow, alternately clench and unclench your fist;
- Join your hands into a lock, bend and straighten both arms at the elbows;
- Rotate your shoulders forward and backward, then perform circular movements with your forearms;
- Raise your arms straight in front of you and alternately move one after the other (“scissors”).
- Take a thick rubber cord and wrap its ends around your hands. Place the hand of the healthy hand on the table, and place the hand of the affected hand above it, palm down. Perform slow extensions and flexions of the affected arm, while stretching the cord, which will provide resistance. Then turn your hand palm up and repeat the exercise.
- Stand up straight, feet shoulder-width apart, back straight, holding a gymnastic stick in a vertical position in front of you. Slowly turn the stick until it is parallel to the floor (palm pointing down), and also slowly return your hand to its original position. Then turn the stick again to a horizontal position, only the palm now faces upward. Continue twisting the stick, pausing at extreme positions. Do 2-3 sets of 20 reps.
Then you can move on to strength exercises with minimal load, for example, working with a wrist expander, but while avoiding muscle strain.
Some exercises:
- Take a hammer or any other heavy object that is comfortable to hold; the hand is facing upward, the angle at the elbow joint is 90-120 °C. Supinate (extend) the hand and return to its previous position. Do 2 sets of 10 repetitions, with a break of 2-3 minutes.
- Take the hammer in the same way, only the hand is facing downwards (palm up). Bend and straighten your wrist. Do 2 sets of 10 repetitions, with a break of 2-3 minutes.
On the subject: Tinctures for the treatment of joints - recipes and methods of preparation
Diagnosis of tennis elbow
Diagnosis of tennis elbow begins with a detailed interview with the patient. The doctor must find out how long ago these symptoms began, whether they were preceded by injury, and with what movements the pain occurs.
Then the elbow joint area is examined. The doctor performs functional tests to confirm the diagnosis.
Functional diagnostic methods may be needed: X-rays of the elbow joint to exclude other diseases. An x-ray can determine whether there is calcification (calcium deposits) in the area of the epicondyle.
Ultrasound examination (ultrasound) allows you to obtain an image of the structures of interest and determine their size and localization.
Magnetic resonance imaging (MRI) clearly shows soft tissue: altered tendons, inflamed areas.
Treatment
If epicondylitis of the elbow joint is diagnosed, treatment should be comprehensive and take into account dysfunction of the joint, as well as the degree of damage to the tendons and muscles.
During therapy you need:
- Relieving pain at the site of injury.
- Normalization of blood circulation.
- Restoring the motor ability of the elbow joint.
- Prevention of forearm muscle atrophy.
Acute lateral epicondylitis of the elbow joint requires constant fixation of the arm with an elastic bandage in a bent state for 7-8 days; in chronic cases, the forearm and elbow joint are fixed only during the day; the bandage should be removed at night.
SWT reduces to zero the risk of surgical intervention, which is necessary in cases of unsuccessful conservative treatment for 3-4 months. Recovery after surgery takes time, and patients are not always able to return to their usual work. It is easier and smarter to prevent such an outcome by completing a course of shock wave therapy on time.
When to see a doctor
Which doctor treats epicondylitis and in what case is it recommended not to postpone a visit to him? A specialist in the diagnosis and treatment of epicondylitis is an orthopedic traumatologist. Specialists from JSC “Medicine” (clinic of academician Roitebrga) provide consultations in the central district of 2nd Tverskoy-Yamskaya lane 10. Tverskaya, Chekhovskaya, Novoslobodskaya and Mayakovskaya metro stations are located nearby, within walking distance, which makes visiting the clinic as comfortable as possible.
Our main advantages are highly qualified specialists, high-quality equipment, affordable prices, the shortest possible time for conducting research, and an individual approach. Our specialists have accumulated invaluable experience in the successful treatment of epicondylitis.
Reasons for development
The main cause of epicondolitis is the loads that fall on the elbow area. This can include intense physical activity, power lifting, sudden movements, or not very intense, but regular and monotonous actions. They are usually associated with human activities - professional or amateur, sports. For example, they can be provoked by sports in which the hands are actively involved, and professions associated with carrying various heavy objects. It is the regular performance of monotonous movements, which are based on flexion and extension of the elbow joint with simultaneous load on the hands and forearms, that becomes a factor contributing to the development of the disease.
Another common cause is trauma and microtrauma. In particular, the cause of inflammation in the posterior area of the elbow is most often a fall on the elbow.
The risk group includes people with congenital connective tissue dysplasia. Often, people with thoracic and cervical osteochondrosis also develop epicondylitis.
Epicondylitis is more common in men. The risk of developing the disease is present in the more active hand, that is, right-handers are more likely to develop right-sided epicondolitis, and left-handers are more likely to develop left-sided epicondolitis.
Symptoms and signs
Symptoms of epicondylitis can be divided into two main types.
The lateral form is characterized by pain and discomfort:
- locally in the outer area of the elbow;
- when moving;
- when twisting the arm with the elbow bent inward;
- when feeling the outer area of the elbow;
- when bending the hand or strongly clenching the palm into a fist.
The hand does not hurt when at rest or when performing passive movements.
The medial form is characterized by pain in the inner part of the elbow joint when the internal epicondyle is affected. Twisting the arm inward or bending it at the elbow leads to pain that radiates along the inner surface of the shoulder up to the armpit and towards the thumb.
It is not necessary to undergo heavy physical activity to develop internal epicondylitis. Loads can be relatively small, but regular. Therefore, people with the same type of constant loads fall into the risk zone - for example, seamstresses, machinists, golfers. This type of disease often occurs in women after lifting weights.
Are you experiencing symptoms of epicondylitis?
Only a doctor can accurately diagnose the disease. Don't delay your consultation - call