The SARS pandemic became notorious in 2002 after the outbreak of a new viral infection in the USA, China, Canada, Hong Kong and 30 other countries. The new coronavirus also causes atypical pneumonia. How it manifests itself and why it is dangerous - let’s find out together with the expert ALENA PARETSKAYA
Pathophysiologist, immunologist, WHO expert ELENA ZARYANOVA Candidate of Medical Sciences, pulmonologist of the highest category, somnologist
The term “atypical pneumonia” has been used since the 30s of the last century . This is not quite the inflammation of the lungs that occurs with classic pneumonia. Often these diseases become causes of epidemics.
What is atypical pneumonia
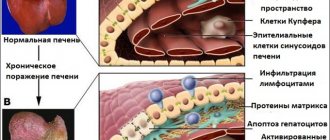
Atypical pneumonia is an inflammation not of the lung sacs themselves, where the exchange of gases occurs, but of the connective tissue surrounding them (the lung framework).
In addition, atypical pneumonia is called because it is not caused by bacteria, as in the “classical” disease, but by viruses, chlamydia, mycoplasma or even rarer pathogens. Outbreaks of atypical pneumonia, especially viral ones, are often observed. They were in 1960, 2002 - 2003, then in 2015 and at the end of 2021, when the most serious epidemics provoked by coronaviruses occurred.
Causes of atypical pneumonia in adults
Atypical inflammation in the lungs can be caused by various pathogens - mycoplasma, coxiella, chlamydia, legionella.
A significant role in the occurrence of atypical pneumonia is played by viruses - influenza A or B, parainfluenza of the first, second and third types, Ebstein-Barr virus, PC virus, hantavirus, coronaviruses and the causative agents of leptospirosis and tularemia. The main problem with these pneumonias is that they are not treated with antibiotics (if they are viruses) or require special types of antibiotics (if they are mycoplasmas and other pathogens).
You can become infected with SARS pathogens through contact with people at work or in public places. The main route of transmission is through communication, coughing or sneezing with droplets of saliva and mucus. The incubation period depends on the type of infection - it lasts from 3 to 10 days, for coronavirus - up to 14 days.
Features of the disease
Atypical pneumonia has an acute onset of symptoms. This type of pneumonia is being actively studied by pulmonologists, since this term appeared in medicine relatively recently - in the early 30s of the 20th century. Atypical pneumonia is common among young people, and the pathological process can also develop in children.
One of the tasks that modern pulmonologists solve is the selection of effective drugs that suppress the activity of viruses and bacteria. When prescribing therapeutic measures, pulmonologists use clinical recommendations for the treatment of atypical pneumonia.
The range of treatment measures prescribed to patients at the Yusupov Hospital depends on many factors, one of which is the staged nature of the process. It has been revealed that the development of atypical pneumonia occurs in several stages:
- The incubation period lasts from the moment the pathogen enters the body and the first signs of the disease appear. The average duration of this period is 8 days;
- the period of precursors lasts up to 3 days. The patient develops signs of respiratory diseases that are not specific to pneumonia;
- the period of the height of the disease is characterized by the appearance of an inflammatory process in the lungs;
- The period of convalescence is characterized by a decrease in the inflammatory process and normalization of the patient’s condition.
Treatment of atypical pneumonia in adults at the Yusupov multidisciplinary hospital is carried out in comfortable conditions. Patients who are indicated for inpatient treatment are accommodated in spacious rooms with the necessary hygiene supplies. The Yusupov Hospital is located in a place with developed infrastructure, so clients can arrive by public transport. For the convenience of patients arriving by car, a parking area is provided.
Make an appointment
Symptoms of atypical pneumonia in adults
Symptoms of the disease may vary depending on the type of pathogen.
Mycoplasma pneumonia. Often has a mild or moderate course. Characteristic symptoms are low long-term fever, dry cough for up to 2 - 3 weeks, weakness, weakness, headache and malaise. Usually both lungs are affected, but the percentage of damage is small.
Chlamydial pneumonia. It begins as an acute respiratory viral infection, then the temperature rises, body pain, dry cough, and enlarged lymph nodes in the neck occur. Both lungs are affected, shortness of breath occurs on exertion, and difficulty breathing. Often the course is similar to bronchitis and asthma.
Legionnaires' pneumonia (Legionnaires' disease). It happens more often in the summer, in people who sit under air conditioning for a long time. The lobe of the lung and bronchi are affected. It is severe, with high fever up to 40 ° C, toxicosis, severe chills, and headache. The cough is first dry, then with sputum that is mucous or purulent in nature. Typical symptoms include shortness of breath, nausea with vomiting, diarrhea, abdominal pain, tachycardia, and kidney damage.
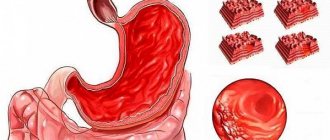
Severe acute respiratory syndrome or atypical viral pneumonia. Usually occurs with coronavirus infection, affects both lungs with manifestations of “cobblestone pavement” or “ground glass effect” on CT. Fever, cough, mostly dry, general malaise, severe weakness, decreased appetite, increasing shortness of breath, palpitations, decreased blood pressure are typical. A cytokine storm, increased blood clotting with thrombosis, cerebrovascular accidents, and heart problems also occur.
Publications in the media
Pneumonia is a group of acute infectious (mainly bacterial) diseases, different in etiology, pathogenesis and morphological characteristics, characterized by focal damage to the respiratory parts of the lungs with the obligatory presence of intra-alveolar exudation. Bacterial pneumonia is pneumonia of bacterial etiology. Classification • According to the conditions in which the disease developed •• Community-acquired pneumonia - acquired outside a medical institution (synonyms: home, outpatient) •• Nosocomial pneumonia - acquired in a medical institution (synonyms: hospital, nosocomial) •• Aspiration pneumonia •• Pneumonia in individuals with severe immune defects (congenital immunodeficiency, HIV infection, iatrogenic immunosuppression, etc.) • Along the course •• Mild - does not require hospitalization •• Severe - hospitalization is required.
Incidence • 236.2 cases per 100,000 adolescents 15–17 years of age • 522.8 cases per 100,000 population under 14 years of age • Community-acquired pneumonia - 1,200 cases per 100,000 population per year • Hospital-acquired pneumonia - 800 cases per 100,000 hospitalizations per year . The predominant age is under 20 and over 60 years. Predominant gender - no significant differences were found by gender. Etiology • Streptococcus pneumoniae - most common (30-50%) • Haemophilus influenzae (10-20%) • Atypical pathogens - Chlamidophila pneumoniae, Mycoplasma pneumoniae, Legionella pneumophila (8-25%) • Typical but rare (3-5 %) include Staphylococcus aureus, Klebsiella pneumoniae (less commonly other enterobacteria) • Moraxella catarrhalis (Branhamella catarrhalis) • Most often, community-acquired pneumonia is caused by pneumococci (their sensitivity to penicillin in many countries is significantly reduced) • In very rare cases of community-acquired pneumonia - Pseudomonas aeruginosa (with cystic fibrosis, bronchiectasis), in persons with severe immunodeficiency - Pneumocystis carinii • Escherichia coli • Anaerobic microorganisms • Atypical pneumonia.
Risk factors • Recent acute respiratory viral infection • Renal failure • Cardiovascular diseases • COPD • Immunodeficiency conditions: diabetes, chronic alcoholism, AIDS, malignant neoplasms • Dysbiosis • Risk factors for hospital-acquired pneumonia •• Mechanical ventilation •• Early postoperative period •• Dysbacteriosis • Risk factors aspiration pneumonia •• Impaired consciousness •• Convulsive seizures •• Diseases of the central nervous system •• Anesthesia •• Reflux esophagitis. Pathogenesis . Main pathogenetic mechanisms • Aspiration of oropharyngeal secretions (the main route of infection) • Inhalation of an aerosol containing microorganisms • Hematogenous spread of pathogens from an extrapulmonary source of infection (for example, with endocarditis, with septic thrombophlebitis) • Direct spread of infection from neighboring affected organs (for example, with liver abscess ) or as a result of injury and infection of the chest organs. Pathomorphology . Segmental, lobar or multifocal peribronchial compaction with stages of red (intra-alveolar exudation and erythrocyte diapedesis) and then gray (fibrous organization of intra-alveolar exudate) hepatization.
Clinical picture. • Complaints •• Cough with mucopurulent (sometimes “rusty”) sputum •• Chest pain when breathing (with concomitant pleurisy) •• Shortness of breath •• Weakness, fatigue •• Night sweats. • Intoxication syndrome •• Fever •• Tachycardia •• Tachypnea •• Hyperhidrosis •• Myalgia •• Headaches •• Anorexia. • Objective examination data •• Cyanosis •• Percussion: dullness of percussion sound caused by infiltration or pleural effusion •• Auscultation ••• Moist fine rales and/or crepitus (heard on inspiration) ••• With extensive infiltration or pleural effusion, breathing is weakened • •• Pleural friction noise with dry pleurisy •• In severe cases, meningeal signs and disturbances of consciousness (for example, disorientation and anxiety) may appear •• In 20% of cases, objective signs may be mild or absent. Laboratory tests • Leukocytosis with a shift of the leukocyte formula to the left •• Leukocytosis more than 10-12109/l is characteristic of a bacterial infection •• Values more than 25109/l or leukopenia below 3109/l indicate a poor prognosis • Hyponatremia • Increased activity transaminases • Bacteriological blood test to identify the pathogen (positive result in 20–30% of patients with community-acquired pneumonia, especially before the start of antibacterial therapy) • At the height of active inflammation and intoxication, protein may appear in the urine • Bacteriological and bacterioscopic examination of sputum: microscopy of a stained smear according to Gram, and culture of sputum obtained during deep coughing • Bacteriological examination of material obtained during bronchoalveolar lavage and thoracentesis • In the presence of pleural effusion and pleural puncture - examination of pleural fluid: counting leukocytes with a leukocyte formula, determination of pH, protein content, LDH, microscopy of a Gram-stained smear, culture for aerobic, anaerobic bacteria and mycobacteria • Study of the immune status of persons with suspected immunodeficiency. Special studies • Chest X-ray is a mandatory research method for pneumonia, allowing to visualize areas of infiltration of lung tissue (take into account the shape, size and location), assess the dynamics of the process •• The prevalence of infiltration, the presence of pleural effusion and signs of destruction of lung tissue reflect the severity of the disease and significantly influence the nature of treatment • CT scan of the lungs is performed if destruction or neoplasm is suspected • Fiberoptic bronchoscopy with microbiological and cytological examination of the biopsy specimen - if tuberculosis and tumor diseases are suspected • FVD study - for differential diagnosis with respiratory distress syndrome • With extensive infiltration, massive pleural effusion, In the presence of COPD, it is advisable to evaluate arterial blood gases, which may be the basis for hospitalization and low-flow oxygenation • The study of capillary blood gases is not very informative.
Diagnostic tactics , diagnostic algorithms. The diagnosis of pneumonia is considered definite if the patient has radiologically confirmed infiltration of the lung tissue and at least two of the following signs: • acute febrile onset of the disease (body temperature more than 38 ° C); • cough with sputum; • listening to local crepitus, shortening of percussion sound; • leukocytosis more than 10109/l and/or shift of the leukocyte formula to the left more than 10%. Differential diagnosis • Pneumonia of non-bacterial etiology (viral, fungal, caused by protozoa) • Tuberculosis (examination of at least three sputum smears, Ziehl-Neelsen stained, sputum culture, PCR diagnosis) • Pulmonary infarction (PE) • Bronchiolitis obliterans • Pulmonary contusion • Pulmonary vasculitis • Acute sarcoidosis • Exogenous allergic alveolitis • Eosinophilic infiltrate • Lung tumors • Other conditions that can cause infiltration syndrome on chest x-ray.
TREATMENT Diet. A complete diet with sufficient protein and a high content of vitamins A, C, group B • Limiting carbohydrates to 200–250 g/day, table salt to 4–6 g/day and increasing the proportion of dairy products • Introducing a sufficient amount of fluid (1500–1700 ml/day) • Saturation of the diet with foods rich in vitamin P (aronia, rose hips, black currants, lemon) • Inclusion of foods rich in B vitamins (meat, fish, yeast, wheat bran decoction) prevents the suppression of intestinal microflora by antibiotics • Foods rich in nicotinic acid • Foods rich in vitamins A and -carotene (carrots, red vegetables and fruits) promote the regeneration of the epithelium of the respiratory tract. Fruit and vegetable juices are recommended • Food is given in crushed and liquid form, meals are taken 6-7 times a day • Energy value is from 1600 kcal/day, increasing as recovery progresses to 2800 kcal/day. Indications for hospitalization • Age under 16 or over 60 years • Concomitant diseases (for example, diseases of the bronchopulmonary system or cardiovascular system, circulatory failure IIa and higher, diabetes, thyrotoxicosis) • Physical signs: respiratory rate more than 30 per minute, diastolic blood pressure less than 90 mm Hg. Art., pulse more than 125 per minute, body temperature less than 35 °C or 40 °C or more, disturbances of consciousness • Laboratory data: the number of leukocytes in the peripheral blood is less than 4.0109/l or more than 30.0109/l , arterial blood oxygen saturation is less than 92% (according to pulse oximetry), paO2 is less than 60 mm Hg. and/or paCO2 more than 50 mm Hg. when breathing room air, serum creatinine content is higher than 176.7 µmol/l or urea nitrogen is higher than 7.0 mmol/l, Ht is less than 30% or Hb content is lower than 90 g/l • X-ray data: pneumonic infiltration of more than one lobe, the presence of decay cavities, pleural effusion, rapid progression of focal infiltrative changes in the lungs (increase in the size of infiltration by more than 50% within 2 days) • Extrapulmonary foci of infection (meningitis, septic arthritis, etc.) • Sepsis or multiple organ failure with metabolic acidosis (pH <7.35), coagulopathy • Impossibility of adequate care and fulfillment of all medical prescriptions at home • Lack of effect from outpatient treatment for 3 days, long-term persistence of intoxication syndrome • Preference of the patient and/or his family members.
Drug therapy. The basis of treatment is antibacterial therapy. It begins from the moment of diagnosis, but after collecting material for bacterioscopic and bacteriological examination of sputum. At home, as well as in a hospital, in the first days of the disease (before receiving the results of bacteriological studies), drugs are selected empirically. After receiving the results of a bacteriological study, treatment is carried out taking into account the sensitivity of the pathogen to drugs •• Treatment of community-acquired pneumonia in an outpatient setting ••• Persons under 60 years of age without concomitant diseases are prescribed amoxicillin (500 mg 3 times / day) or amoxicillin + clavulanic acid, or macrolides ( spiramycin, clarithromycin, azithromycin, midecamycin, etc.), or pneumotropic fluoroquinolones (levofloxacin) ••• For non-severe pneumonia in patients over 60 years of age and/or with concomitant diseases, treatment with amoxicillin/clavulanate or cefuroxime is started; levofloxacin is an alternative ••• If it is impossible to take drugs orally, parenteral administration of ceftriaxone is used ••• The effect of treatment is assessed after 48–72 hours, primarily by reducing body temperature. In this regard, NSAIDs should not be used during this period without special indications. If the temperature and intoxication syndrome do not decrease, a change in antibiotic is indicated with a re-assessment of the advisability of hospitalizing the patient •••• If amoxicillin was used, switch to macrolides; if amoxicillin + clavulanic acid or cefuroxime were used, switch to levofloxacin; if macrolides were used, switch to amoxicillin + clavulanic acid or levofloxacin ••• Antibacterial therapy is stopped with stable normalization of temperature on the 3-4th day •• Treatment in a hospital ••• For mild pneumonia, therapy begins with intravenous administration of ampicillin (or amoxicillin/clavulanate, cefuroxime, cefotaxime or ceftriaxone) with switching to oral administration of drugs of the same group (stepped therapy) ••• In severe pneumonia, treatment begins with intravenous administration of a macrolide (erythromycin, spiramycin, clarithromycin) in combination with an intravenous β-lactam drug (amoxicillin/clavulanate, cefotaxime, ceftriaxone) •• • An alternative may be the intravenous administration of a combination of third-generation cephalosporins with early fluoroquinolones (ciprofloxacin, ofloxacin) or the intravenous administration of new fluoroquinolones (levofloxacin, moxifloxacin) •• Treatment of nosocomial pneumonia in general wards: prescribe IV amoxicillin + clavulanic acid, ampicillin / sulbactam or cephalosporins of II–III generations, alternatives are new fluoroquinolones (levofloxacin, moxifloxacin), carbapenems, cefoperazone + sulbactam, cefepime; in intensive care units and wards - carbapenems, cefepime or cefoperazone + sulbactam, ticarcillin + clavulanic acid, piperacillin / tazobactam •• In the treatment of aspiration pneumonia, intravenous forms of cephalosporins of III-IV generations, levofloxacin, moxifloxacin, ticarcillin + clavulanic acid, piperacillin / taz are recommended obactam , amoxicillin+clavulanic acid, ampicillin/sulbactam. For persons with periodontal diseases or alcoholism - a combination of III-IV generation cephalosporins with metronidazole or lincomycin •• In the treatment of pneumonia in patients with AIDS, intravenous combinations of co-trimoxazole with amoxicillin and itraconazole (or fluconazole) are recommended •• For destructive pneumonia (or abscess formation) they are used IV amoxicillin + clavulanic acid, ampicillin / sulbactam, cefoperazone + sulbactam or carbapenems, ticarcillin + clavulanic acid, piperacillin + sulbactam, combination of lincomycin with an aminoglycoside; combination of benzylpenicillin + metronidazole with a transition to the combination of amoxicillin + metronidazole orally (stepped therapy). The duration of therapy is 3–4 weeks or more.
• Tactics of antibacterial therapy after obtaining the results of bacteriological studies, if the sensitivity of microorganisms to antibiotics has not been determined •• For pneumococcal damage - benzylpenicillin 1-2 million units intramuscularly every 4 hours, erythromycin 500 mg every 6 hours, roxithromycin 150 mg 2 times a day or azithromycin 500 mg 1 time / day. For resistant strains - cefotaxime, ceftriaxone, imipenem + cilastatin •• For H. influenzae infection - co-trimoxazole 2 tablets every 12 hours. Reserve drugs: cephalosporins of the II and III generations (cefuroxime 0.25-1 g IV every 12 h, cefaclor 0.5–1 g orally every 6 hours), chloramphenicol 0.5–1 g every 6 hours, amoxicillin + clavulanic acid •• For Staphylococcus aureus lesions - oxacillin 6–10 g/day, first generation cephalosporins or clindamycin 600–800 mg IV every 6–8 hours. For resistant strains - vancomycin •• For Klebsiella lesions - aminoglycosides, third generation cephalosporins (cefotaxime 2 g IV every 6 hours, ceftazidime 2 g IV every 8 hours; ceftriaxone 2 g IV every 12 hours), fluoroquinolone derivatives (ciprofloxacin 500–750 mg 2 times / day), imipenem + cilastatin 1 g 2 times / day •• For Escherichia coli lesions - aminoglycosides, cephalosporins II and III generations. Alternative drugs - fluoroquinolone derivatives, imipenem + cilastatin, chloramphenicol •• For Pseudomonas aeruginosa lesions - a combination of aminoglycoside and carbenicillin or ceftazidime, azlocillin or imipenem + cilastatin •• For Enterococci lesions - a combination of ampicillin and gentamicin •• For Moraxella catarrhalis lesions - cefa II generation losporins or amoxicillin + clavulanic acid, co-trimoxazole, clarithromycin •• If Acinetobacter is affected - imipenem + cilastatin or aminoglycosides, co-trimoxazole. • Expectorants •• Agents that stimulate expectoration ••• Direct-acting drugs, for example potassium iodide ••• Reflex-action drugs, for example, thermopsis herb infusion, licorice root preparations, etc. •• Mucolytic drugs, for example acetylcysteine, trypsin, bromhexine, ambroxol. • Oxygen therapy for patients with cyanosis, hypoxia, shortness of breath.
Surgical treatment of pneumonia is not performed. The question of surgical intervention arises when an abscess forms, especially a chronic one, or when pneumonia is complicated by pleural empyema. Monitoring the effectiveness of treatment • Clinical indicators •• Fever •• Shortness of breath •• Cough • X-ray dynamics (lags behind clinical) • Bacteriological examination of sputum - if treatment is ineffective. Complications • Pleural effusion (complicated and uncomplicated) • Destruction/abscessation of lung tissue • Acute respiratory distress syndrome • Acute respiratory failure • Infectious-septic shock • Pleural empyema. • Secondary bacteremia, sepsis, focus of hematogenous dissemination • Pericarditis, myocarditis • Nephritis. Prevention • Prevention of aspiration in bedridden patients • Rational use of antibiotics • Annual influenza vaccination for people at high risk • Polyvalent pneumococcal vaccine (currently not available in Russia) is recommended for people over 65 years of age and children over 2 years of age with the following risk factors •• Dysfunction spleen or asplenia •• Lymphogranulomatosis •• Multiple myeloma •• Liver cirrhosis •• Chronic alcoholism •• Renal failure •• Immunodeficiency. Age characteristics • Children •• Focal-confluent nature of the lesion predominates •• In the clinical picture - acute onset, severe intoxication against the background of a weak (or absence) pain syndrome, pronounced auscultation pattern •• Dynamics against the background of antibacterial treatment - rapid positive effect •• High mortality in children under 1 year of age • Elderly and old people: morbidity and mortality are increased over the age of 70 years, especially with concomitant pathology or the presence of risk factors. Features for pregnant and lactating women • During pregnancy, the use of β-lactam antibiotics, macrolides, metronidazole is permissible; fluoroquinolones, tetracyclines, aminoglycosides, lincosamides, co-trimoxazole are contraindicated • When breastfeeding, penicillins, cephalosporins, azithromycin are acceptable with caution; macrolides, fluoroquinolones, carbapenems, tetracyclines, lincosamides, co-trimoxazole are not recommended. Course and prognosis • Depend on the severity of the course, the pathogen, the patient’s age, the time of initiation of treatment, the adequacy of initial therapy, the state of the immune system, concomitant diseases • Mortality from community-acquired pneumonia: 1–3% - among young previously healthy people, 15–30% - in older age groups with concomitant diseases.
ICD-10 • J13 Pneumonia caused by Streptococcus pneumoniae • J14 Pneumonia caused by Haemophilus influenzae [Afanasyev-Pfeiffer bacillus] • J15 Bacterial pneumonia, not elsewhere classified • J17.0* Pneumonia in bacterial diseases classified elsewhere
Causative agents of atypical pneumonia in adults
Although atypical pneumonia is a whole group of diseases in which inflammation of the lungs occurs, 4 types of pathogens are most often found:
- mycoplasmas are microorganisms that do not have a typical cell wall; they belong to bacteria, but have some characteristics of viruses;
- chlamydia are intracellular parasites that infect lung tissue;
- legionella - pathogenic bacteria that cause pneumonia and Legionnaires' disease;
- coronaviruses – provoke outbreaks of pneumonia, damage to internal organs, thrombosis, and cytokine storm.
Forecast
The prognosis of how atypical pneumonia will develop is determined by the symptoms and type of pathogen. With timely therapy and a strong immune response, the prognosis is favorable. In childhood, pneumonia can be complicated by damage to the alveoli and the development of emphysema. In addition, self-medication may cause the disease to become chronic.
If left untreated, death is possible, but modern therapeutic methods make it possible to provide quality care to patients with various forms and severity of the disease. Doctors at the Yusupov Hospital carry out emergency hospitalization and take measures necessary to improve the patient’s condition.
Patients can go to the Yusupov Hospital if their condition worsens at any time of the day. You can make an appointment with candidates and doctors of science with many years of experience at a convenient time, and find out about the cost and terms of service by calling the Yusupov Hospital.
Diagnostics
The basis for diagnosing atypical pneumonia is the patient’s complaints and external examination, changes in the lungs that the doctor hears by listening to the chest with a phonendoscope.
However, this is the only way to determine pneumonia. Additionally needed:
- blood and urine tests, sputum cultures,
- PCR study to detect viruses or mycoplasmas, chlamydia;
- X-ray of the lungs;
- CT scan of the lungs to determine the percentage of damage to the lung tissue and the typical pattern of changes;
- additional tests to detect lesions in other organs (ECG, ultrasound, MRI).
Modern methods of treatment
Mycoplasma pneumonia is treated with antibiotics from the macrolide group (Erythromycin or Azithromycin), or in some cases Clindamycin is prescribed.
The course should last at least 7 - 10 days. Chlamydial pneumonia is treated with macrolides and tetracycline antibiotics; the course lasts at least 10-14 days. If these drugs do not help, doxycycline or fluoroquinolones (Ofloxacin) are prescribed.
Pneumonia caused by Legionella is treated with intravenous antibiotics - Doxycycline, Ofloxacin, Rifampicin. Sometimes the patient needs mechanical ventilation, as the lungs are often very damaged. Often, hormones (short course corticosteroids) are also used against the background of antibiotics.
There is no specific treatment for viral pneumonia. There is evidence of the effectiveness of Favipiravir and Remdesevir, but they are used for severe cases. Hormones, drugs that prevent cytokine storm, and blood thinners are also used.
General treatment for all atypical pneumonia is correction of symptoms:
- antipyretic drugs (Nurofen, Ibuklin, Paracetamol, Theraflu, Coldact, Coldrex);
- drugs for thinning sputum (ACC, Ambroxol, Ambrobene, Bromhexine);
- vitamins (ascorbic acid and vitamin D);
- drinking plenty of fluids or giving intravenous fluids;
- bed rest, full sleep;
- oxygen support for severe shortness of breath.