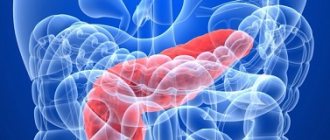
Among all diseases of the gastrointestinal tract (GIT), the incidence of chronic pancreatitis ranges from 5.1 to 9%, and in the last few decades, the incidence of pancreatitis in our country has doubled1.
Chronic pancreatitis is an insidious disease, largely due to its recurrent nature. Patients are often concerned about periods of exacerbation, accompanied by severe pain, nausea, and vomiting.
Where does chronic pancreatitis come from? What causes the disease and is it possible to fight it? Let's try to figure it out.
Symptoms of chronic pancreatitis
Symptoms of chronic pancreatitis may vary depending on the stage (remission or exacerbation), course and physical condition of the patient. The main signs of the disease are as follows:
- acute pain without clear localization. Pain can be felt in the right hypochondrium, upper or middle abdomen and spread to the back. In many patients, pain occurs immediately after eating, especially if the diet contained fatty, smoked or spicy foods;
- frequent loose stools are one of the main signs of indigestion. Digestive problems in chronic pancreatitis are caused by a lack of enzymes;
- heaviness in the abdomen, nausea, which also indicate a lack of digestive enzymes;
- increasing feeling of hunger, muscle tremors, weakness, cold sweat;
- intoxication, manifested in fever, chronic fatigue, and a feeling of general malaise.
Causes of chronic pancreatitis
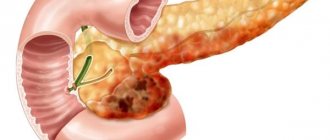
One of the most common causes of chronic pancreatitis is poor diet and unhealthy lifestyle. Constant overeating, abuse of fatty foods and alcohol cause blockage of the excretory ducts of the pancreas.
Narrowed excretory ducts provoke the accumulation and premature activation of digestive enzymes. As a result, the pancreas actually begins to digest itself, and inflammation forms1.
In addition, the following factors can lead to chronic pancreatitis3:
- ulcer of the duodenum, stomach and enteritis. Chronic inflammation of the mucous membrane of the gastrointestinal tract makes it difficult to secrete pancreatic juice, which often causes chronic pancreatitis;
- cholelithiasis. After leaving the gallbladder, the stone causes blockage of the common duct and inflammation of the pancreas develops;
- genetic predisposition;
- toxic effects of drugs.
Reasons for the development of the disease
Main causes:
- infections of the urinary and reproductive systems - prostatitis, cystitis, etc.;
- diseases of the respiratory tract and ENT organs - bronchitis, sinusitis, pneumonia, etc.;
- infection of the gallbladder ducts by parasites;
- acute or chronic inflammation in the gastrointestinal tract - colitis, dysbacteriosis, etc.
Other risk factors:
- obesity;
- biliary dyskinesia;
- autoimmune diseases;
- reflux of the contents of the duodenum into the gallbladder and bile ducts;
- violation of the composition of bile;
- changes in hormonal levels (pregnancy, menstruation);
- pathologies in the development of the gallbladder;
- abuse of fried, fatty and spicy foods;
- allergy;
- genetic predisposition;
- smoking and alcohol abuse.
Diagnosis of chronic pancreatitis
Identifying chronic pancreatitis can be difficult due to the nonspecific clinical picture. Nausea, abdominal pain, digestive problems - these symptoms are characteristic of many diseases, for example, stomach ulcers or chronic cholecystitis. Therefore, identifying the disease may require a whole range of studies. Diagnosis of chronic pancreatitis may include2,3:
- external examination of the patient. Chronic pancreatitis may be indicated by bluish areas of the skin on the front and side walls of the abdomen. In some patients, bright red patches of skin on the chest and back become noticeable. Palpation may reveal pain in the left hypochondrium and the upper third of the abdomen;
- a general and detailed blood test, which shows the presence of an inflammatory process, based on an increase in the concentration of leukocytes;
- laboratory blood test to identify markers of nutritional status;
- fecal elastase test;
- ultrasonography. In some cases, ultrasound examination (ultrasound) can be performed through the walls of the stomach and duodenum, which significantly increases the accuracy of the examination. This method is called endoUS and combines the possibility of endoscopic and ultrasound diagnostics of the gastrointestinal tract (GIT);
- computed tomography: used to determine complications of pancreatitis associated with thickening of the pancreas tissue.
You need to see a doctor
- If there is pain in the right hypochondrium (abdominal pain). In chronic cholecystitis, the pain is dull, aching, lasting from several hours and days to several weeks. A characteristic feature of pain in chronic cholecystitis is its occurrence or intensification after eating fatty or fried foods. In chronic cholecystitis, pain from the right hypochondrium spreads upward to the right shoulder and neck. Often, against the background of a dull aching pain, the patient notes short attacks of acute cutting pain, characteristic of exacerbation of chronic cholecystitis.
- With vomiting, which is a less constant symptom of chronic cholecystitis and, like pain, occurs mainly after the patient violates the dietary regimen. In addition to vomiting, patients with chronic cholecystitis may experience prolonged nausea, a bitter or metallic taste in the mouth, and decreased appetite.
- If you are worried about bloating, constipation and diarrhea, these are quite common symptoms of chronic cholecystitis, indicating a gradual deterioration of its function and a disorder of the digestive process. Bloating, diarrhea, or constipation are rarely caused by chronic cholecystitis alone. As a rule, in patients with more or less long experience of this disease, there is a parallel disorder of the function of the stomach and pancreas (gastritis and pancreatitis), which also affects the quality of digestion.
- Patients with advanced cholecystitis may experience severe weakness, a predisposition to frequent colds, decreased performance, and irritability.
Exacerbation of chronic pancreatitis
Chronic pancreatitis may hardly manifest itself until the period of exacerbation. Relapse of the disease is usually associated with two main reasons3:
- alcohol consumption. Even a small amount of alcohol consumed can provoke the transition of the disease into the acute phase;
- violation of the diet, overeating, a large number of fatty, fried, spicy dishes on the menu.
Other factors can also provoke exacerbation of chronic pancreatitis in adults, for example, chronic stress, physical fatigue, poisoning or the toxic effects of certain medications3.
Exacerbation of the disease is manifested by the following symptoms3:
- attack of acute or dull pain in the hypochondrium. Painful sensations spread to the subscapular region or the entire back;
- progressive diarrhea. In this case, the feces have a characteristic greasy shine. Undigested food remains are often observed in the stool;
- the occurrence of specific bitterness in the oral cavity, nausea and loss of appetite;
- whitish coating on the surface of the tongue;
- weight loss.
Exacerbation of chronic pancreatitis in adults can last for one to two weeks. You cannot fight the disease on your own during this period: the best solution is hospitalization and constant monitoring by specialists.
Treatment of chronic pancreatitis
The answer to the question “how to cure chronic pancreatitis” remains open even for modern doctors. The treatment regimen is determined by the doctor for each individual case. The main thing is that therapy should be comprehensive, affecting the main cause of the disease.
Treatment of chronic pancreatitis includes2,3,4:
- immediate cessation of bad habits. Smoking and abuse of strong alcoholic beverages aggravate the inflammatory process and contribute to the subsequent development of the disease;
- strict adherence to the diet. The daily diet should contain high-calorie foods, without spicy foods, salt and pure sugar. You should eat food often, in small portions. In case of exacerbation of chronic pancreatitis, therapeutic fasting is prescribed, which will help stop pancreatic secretion and relieve pain. After 1-3 “hungry” days, the patient is transferred to a special diet;
- basic therapy. In this case, we are talking about taking the following type of drugs: antispasmodics and analgesics, antisecretory and detoxification drugs. Treatment is carried out under the supervision of a doctor with strict adherence to the instructions;
- taking enzyme preparations, the task of which is to compensate for the impaired functioning of the pancreas. The fact is that the pancreas does not recover (it is not the liver), and therefore will no longer be able to work at full capacity during chronic pancreatitis. That is why the first line of therapy is enzyme preparations, which should be taken for life. An example of an enzyme drug prescribed for chronic pancreatitis is Creon®;
- complex therapy. May include taking antispasmodics or analgesics, antisecretory and detoxification medications. Therapy is carried out under the supervision of a physician with strict adherence to the instructions;
- taking anti-inflammatory and painkillers that improve the patient’s well-being;
- herbal medicine, which can be prescribed during remission only as prescribed by a doctor.
What to do if an exacerbation of pancreatitis occurs suddenly, and the ambulance has not yet arrived? Before the doctors arrive, you need to lie down, try to relax your abdominal muscles as much as possible and apply a heating pad with cold water to the sore spot. You should not take painkillers or any other medications - this will interfere with correct diagnosis. And, of course, any food and drinks, even plain water, are strictly prohibited, because any food or liquid can cause increased pain3.
Diagnostics
Blood analysis. The results of a blood sample during an exacerbation often reveal an increase in ESR, eosinophilia, neutrophilic leukocytosis, and a shift to the left in the leukocyte formula. Complicated forms are accompanied by an increase in blood levels of cholesterol, bilirubin, and transaminases.
Duodenal sounding. The severity of the inflammatory process is characterized by the results of analyzes of bile obtained from the body during duodenal intubation. As a rule, in this case, the bile is cloudy, it contains flakes, a significant admixture of mucus, cellular detritus, and columnar epithelium.
Bacteriological research. All portions of bile are analyzed. This makes it possible to determine the etiology of the inflammatory process and the susceptibility of the body's microflora to antibiotics.
Ultrasound and X-ray. X-ray examination can detect various signs of morphological or functional changes in the gallbladder or other digestive organs. Contrast examination of the gallbladder (cholangiography, cholecystography) makes it possible to identify disturbances in concentration ability, impaired motor function, and deformation.
Radioisotope method. Studying the state of the biliary tract and analyzing the absorption and excretion function of the liver can be carried out using the radioisotope method. More accurate diagnosis is achieved in combination with fractional multicomponent duodenal intubation. A more detailed study of the gallbladder and ducts is possible using the radio-X-ray chromodiagnostic method. Using ultrasound, it is possible to establish the absence of stones, as well as assess the contractility and condition of the gallbladder wall (a sign of chronic cholecystitis is its thickening by 4 mm or more).
The drug Creon® 25000 for chronic pancreatitis
Find out more
Decreased pancreatic function inevitably leads to a lack of digestive enzymes in the body, so-called enzyme deficiency. As a result, the quality of digestion suffers, and the body does not receive the necessary energy and nutrients for full functioning. Creon® is designed specifically to compensate for the lack of its own enzymes through their delivery from the outside and belongs to the group of enzyme preparations. The drug contains enzymes identical to those produced by the pancreas. The key feature is that the active ingredient Creon® is small particles - minimicrospheres, which are collected in a capsule. The fact is that science has been studying enzyme preparations for more than 100 years in order to increase their effectiveness. To date, scientific advances indicate that preparations with particles whose size does not exceed 2 mm4.5 can most accurately recreate the natural process of digestion. Moreover, it has been scientifically proven that the smaller the particles of the drug, the more effective it can be4,6.
Creon® is the only drug whose capsule contains hundreds of small particles - minimicrospheres7. Their size does not exceed 2 mm, which is recorded as recommended in world and Russian scientific works4,5,6.
Treatment
Medication. Treatment of chronic cholecystitis is almost always carried out conservatively by a gastroenterologist. During an exacerbation, it is aimed at eliminating acute symptoms, sanitizing the source of bacterial infection with the help of antibiotic therapy (broad-spectrum drugs are used for this, often belonging to the group of cephalosporins), detoxifying the body (introducing solutions of sodium chloride, glucose), restoring normal digestive function ( various enzyme preparations). Pain relief and inflammation relief during treatment are achieved with drugs from the group of non-steroidal anti-inflammatory drugs (NSAIDs), and spasm of the smooth muscles of the gallbladder and its ducts is relieved by antispasmodics. Elimination of bile stagnation is carried out with the help of drugs that enhance the peristalsis of the biliary tract (olive oil, sea buckthorn, magnesia). Choleretics are rarely used.
Operational. Chronic calculous cholecystitis is an indication for surgical removal of the gallbladder, which is the source of stone formation. The operation is not an emergency measure and is scheduled. Laparoscopic surgery or cholecystectomy are used. Percutaneous cholecystostomy is indicated for frail and elderly patients.
Non-surgical. If there are contraindications to surgery, non-surgical crushing of stones (extracorporeal shock wave lithotripsy) is used, but soon, as a rule, they re-form.
To make an appointment at the ABC-Medicine clinic for the treatment of chronic cholecystitis, call +7 (495) 223-38-83.
What else is important to know about enzyme preparations?
The minimum starting dosage is Creon® 25,000 units, which is stated in Russian recommendations for the treatment of chronic pancreatitis and exocrine pancreatic insufficiency2,5. The number indicates the amount of the enzyme lipase, which helps digest fats. If necessary, the doctor can increase the dosage; in European practice, the required dose per single dose can reach up to 80,000 units8. By comparison, the pancreas of a healthy person produces up to 720,000 of these units during each meal9.
Therapy should be taken seriously, since high-quality “nutrition” of the body is the key to its functioning. How long can a person live without energy from food? With chronic pancreatitis, the body must be supplied with enzymes at every meal, even with a snack. Thus, in accordance with the instructions for the drug Creon®, a full dose is required for a meal (for example, 25,000 units), and half for a snack. Creon® capsules are convenient to use: you can open them and add minimicrospheres to food, thereby selecting the desired dose10. More information about the admission rules can be found here.