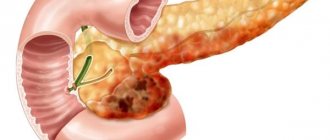
Pancreatitis is an acute or chronic inflammation of the enzymatic pancreas and peripancreatic tissues, manifested by low back pain and increased activity of pancreatic enzymes. About two-thirds of cases of acute pancreatitis (AP) are caused by long-term excessive alcohol consumption or gallstones.
The etiology of AP, recurrent and chronic pancreatitis (CP) is very diverse. Various combinations of genetic, epigenetic, metabolic and environmental factors can trigger the inflammatory process and lead to its effects in several systems that regulate and maintain pancreatic function.
When treating the patient and taking preventive measures, it is important to determine the etiological factors in order to prevent relapse of the disease. This article takes a closer look at the rarer causes of acute and chronic pancreatitis.
Epidemiology
The content of the article
According to recent studies, every 34 people out of 100 thousand get pancreatitis every year, and due to the increasing prevalence of the main etiological risk factors - obesity, alcoholism, smoking, stone formation, the disease is diagnosed in younger people. Also, such statistics are associated with improved diagnosis and identification of less common causes of pancreatitis.
An independent risk factor for AP is smoking. This habit worsens alcohol-related damage to the pancreas.
Risk factor for pancreatitis is smoking
Most patients have mild pancreatitis; in 20-30% of cases, severe pancreatitis occurs. The mortality rate from severe pancreatitis is about 15%.
Prevention
To prevent pancreatic necrosis, you need to follow some simple recommendations:
- Limit the amount and frequency of alcohol consumption.
- Avoid junk food – fast food, processed foods, soda, and minimize the consumption of fatty and fried foods.
- Do not take medications without a doctor’s prescription, especially do not abuse them.
- Try to create a diet based on natural products, try to practice split meals in small portions.
- Treat cholelithiasis in a timely manner.
- At the first symptoms indicating problems with the pancreas, consult a doctor immediately.
- Follow the principles of a healthy lifestyle.
Etiology
The etiological factors of pancreatitis are very diverse - metabolic, mechanical, infectious, vascular. Often the disease occurs as a result of the interaction of several factors. The etiology of AP is determined only in 75% of patients.
Chronic pancreatitis is classified according to etiology and risk factors according to the TIGAR-O classification (Table 1).
Table 1. Etiological classification of chronic pancreatitis (TIGAR-O)
| Toxic-metabolic |
| Alcohol; Tobacco, smoking; Hypercalcemia (hyperparathyroidism); Hyperlipidemia; Chronic renal failure; Drugs and toxins. |
| Idiopathic |
| Early start; Late start; Tropical calcific pancreatitis, fibrocalcular pancreatic diabetes. |
| Genetic |
Autosomal dominant
|
| Autoimmune |
| Autoimmune pancreatitis type 1 (IgG4 positive); Autoimmune pancreatitis type 2 (negative IgG4). |
| Recurrent (reversible) and acute |
| Ponecrotic (acute); Reversible sharp:
Ischemic (postoperative, hypotensive); Infectious (viral); Chronic alcoholism; Poradiative; Diabetes. |
| Obstructive |
Benign pancreatic duct stricture:
Malignant stricture; Periampullary carcinoma; Pancreatic adenocarcinoma. |
Table 2. Rare causes of pancreatitis
| Nosology | Characteristics | Diagnostics |
| Metabolic pancreatitis | Hypertriglyceridemia and hypercalcemia | OP or HP |
| Drug-induced pancreatitis | Azathioprine, 6-mercaptopurine, sulfonamides, estrogens, tetracycline, valproic acid, antiretroviral drugs | OP or HP |
| Autoimmune pancreatitis | Focal or diffuse enlargement of the pancreas, hypotensive pancreatic shunt, expansion of the papillary part due to lymphoplasmocytes p.
| HP |
| Hereditary pancreatitis | Usually occurs at a young age, gene mutations are detected | Acute recurrent pancreatitis |
| Pancreatitis after the procedure | Endoscopic retrograde cholangiopancreatography was recently performed | Most often OP |
| Pancreatitis with sedimentation of bile (sediment) | Bile deposits and small stones (microlithiasis) | Most often OP |
| Pancreatitis Paraduodeninio groove ( groove ) | Fibrous formations between the head of the pancreas and the thickened wall of the duodenum, leading to duodenal stenosis, cystic changes in the pancreaticoduodenal groove or duodenal wall, pancreatic and bile duct stenosis | Exclusively HP |
| Duodenal diverticulum | Periampullary diverticulum, wind deformation | OP>HP |
| Traumatic pancreatitis | Direct trauma to the pancreas, intrapancreatic hematoma, rupture of the pancreas with fluid around it | OP or HP |
| Infectious pancreatitis | Various infectious factors: viruses, bacteria, fungi. | Most often in OP |
| Ischemic pancreatitis | Pancreatitis due to circulatory disorders, arterial hypotension, cardiogenic shock | OP or HP |
Consequences and complications
Pancreatic necrosis is a dangerous disease, and if it develops rapidly, the patient may die within 24 hours after its onset. Whether a person can survive fat necrosis depends on how affected the gland is, how widespread the damage is, and how large the area of edema is.
With pancreatic necrosis, the following consequences are possible:
- rupture of the biliary tract;
- cerebral edema;
- damage to lung tissue;
- bleeding and, as a consequence, decomposition of the pancreas and stomach;
- peritonitis;
- peptic ulcer;
- enzyme deficiency;
- intoxication of the gastrointestinal tract;
- thrombosis of venous arteries;
- pancreatic fistulas;
- pancreatic cyst;
- suppuration in the pancreas;
- state of shock.
In addition, necrosis of the pancreas can lead to diabetes mellitus , rectal or pancreatic cancer.
Hypertriglyceridemic pancreatitis
Hypertriglyceridemic pancreatitis accounts for 1-14% of cases of AP and 56% of cases of pancreatitis in pregnant women. Hypertriglyceridemia is defined as elevated fasting triglycerides (TG) (>1.7 mmol/L). Serum TG levels above 11.3 mmol/l can lead to the development of AP in 5% of cases. In cases where the TG concentration exceeds 22.6 mmol/l, the incidence of AP is 10–20%. The risk of AP increases with a TG concentration of 5.6 mmol/l: the higher it is, the higher the risk of AP and the more severe the pancreatitis.
Pancreatitis caused by hypertriglyceridemia is associated with both primary (genetic - dyslipidemia types I, IV, V) and secondary (acquired) disorders of lipoprotein metabolism. The main causes of acquired hypertriglyceridemia are obesity, diabetes, hypothyroidism, pregnancy and medication use - treatment with estrogens or tamoxifen, beta-blockers, antiretroviral drugs, thiazide diuretics.
During pregnancy, TG levels usually rise to 3.3 mmol/L in the third trimester and do not cause pancreatitis. Inheritance is most common during pregnancy due to hereditary familial dyslipidemia.
Inflammation of the pancreas is not caused by TGs themselves, but by toxic free fatty acids formed as a result of hydrolysis of the pancreas by pancreatic lipases. The clinical picture of the disease is usually no different from ordinary pancreatitis. In some cases, severe hypertriglyceridemia, xanthoma, xantheliosis, hepatosteatosis, etc. may be observed.
It is important to promptly diagnose hypertriglyceridemic pancreatitis and correct triglyceride levels. Standard treatment of pancreatitis is also prescribed - infusion therapy, analgesics.
The main methods of reducing hypertriglyceridemia are apheresis, especially plasmapheresis, and insulin therapy. However, there is no data from randomized studies on the effectiveness of these methods. Treatment is selected based on the severity of pancreatitis and warning signs, including hypocalcemia, lactic acidosis, exacerbation of systemic inflammatory response, and progressive organ dysfunction.
Intravenous insulin should be used if the patient does not tolerate or cannot undergo apheresis. Insulin lowers TG levels, but the goal of this treatment in severe hypertriglyceridemic pancreatitis is to prevent stress-induced release of fatty acids from adipocytes. The usual insulin infusion dose is 0.1-0.3 U/kg/hour and requires hourly blood glucose measurements. To prevent hypoglycemia, a glucose solution is prescribed.
Hourly blood glucose measurements
For therapeutic apheresis, triglyceride levels should be monitored after each procedure. Plasmapheresis is continued until the TG concentration drops to 5.6 mmol/l. For insulin alone, TG levels are monitored every 12 hours. The insulin infusion is stopped when the TG concentration reaches 5.6 mmol/L (usually after a few days).
Further long-term correction of hypertriglyceridemia with TG <2.2 mmol/L is important to prevent recurrence of pancreatitis. There are medical and non-medical measures for this. The latter include diet, weight loss for obesity, increased physical activity, limiting added sugar, and good glycemic control for diabetes. You should also avoid medications that increase TG levels. Medicines include antilipid drugs, usually fibrates (fenofibrate).
Diet for pancreatic necrosis
Diet for pancreatic necrosis of the pancreas
- Efficacy: therapeutic effect after 21 days
- Timing: constantly
- Cost of products: 1800-1900 rubles. in Week
Diet Table No. 5p for pancreatitis
- Efficacy: therapeutic effect after 14 days
- Timing: constantly
- Cost of products: 1400-1500 rubles. in Week
In the first days of treatment for this disease, it is necessary to practice therapeutic fasting. The doctor determines its duration individually. Next, you need to adhere to a strict diet, completely eliminating salty, fatty, smoked, sweet, fried foods, as well as alcohol from the menu. The list of prohibited products is quite wide. You cannot consume cabbage, figs, grapes, bananas, bell peppers, onions, garlic, coffee, cocoa, sausages, canned food, fatty fish, soda, mushrooms, jam, fresh bread, egg yolk, ice cream, millet and barley cereals, and baked goods.
During this period, you are allowed to eat the following foods:
- boiled vegetables;
- porridge with water - oatmeal, rice, semolina, buckwheat;
- lean meat - veal, chicken;
- dairy products;
- baked fruits;
- crackers;
- refined vegetable oils – 10 g per day;
- vegetarian soups with potatoes, carrots, zucchini, pumpkin.
Your doctor will help you create the right diet. This diet must be strictly followed for about a month. If the dynamics are positive, the diet is gradually expanded.
Nutrition after surgery should be supervised by a specialist for the first time. Before the operation, the patient does not eat at all. A day after surgery, he is prescribed parenteral nutrition, using special solutions with a complex of nutrients. Such solutions contain fatty acids, amino acids , minerals, and vitamins. About a week after the operation, the patient begins to have food administered through a tube into the stomach.
Then, after some time, the patient gradually switches to a gentle diet, in which carbohydrates are the basis of the diet, and fats are kept to a minimum. Food needs to be chopped and eaten small and little by little. You should not overeat; the menu should include only boiled and steamed food.
Calcific (hypercalcemic) pancreatitis
Calcific pancreatitis is very rare. The most common causes of hypercalcemia (about 90%) are hyperparathyroidism and malignancy. According to studies, hyperparathyroidism causes about 0.4% of cases of AP.
It is believed that calcium accumulated in the pancreatic duct activates trypsinogen in the pancreatic parenchyma. The low incidence of pancreatitis among patients with chronic hypercalcemia suggests that other factors (sudden increases in serum calcium levels) also influence OP.
Patients with hyperparathyroidism and associated hypercalcemia develop pancreatitis 10 to 20 times more often than the general population. The most common causes of hyperparathyroidism are:
- parathyroid adenoma (80%);
- hyperplasia of all 4 parathyroid glands (15–20%);
- thyroid cancer (2%).
Parathyroid adenoma
The most important principles of treatment are the correction of hypercalcemia and elimination of the root cause. In patients with asymptomatic mild hypercalcemia (calcium concentration 3.5 mmol/L), initial treatment is 200 to 300 ml/hour of isotonic sodium chloride solution based on a urine output of 100 to 150 ml per hour.
For immediate short-term treatment, patients who develop symptoms (lethargy, stupor) are given calcitonin, and for long-term treatment, an intravenous bisphosphonate is added. If bisphosphonates are contraindicated, zoledronic acid or denosumab can be used.
Treatment with folk remedies
When a patient's pancreatic necrosis worsens, he experiences severe pain. Folk remedies that are used in parallel with the main treatment can help improve the condition a little. But, before practicing such methods, it is necessary to visit a doctor, establish a diagnosis and begin practicing the correct treatment regimen.
- The fruits of Japanese Sophora - a decoction is prepared from them. A spoonful of raw materials should be filled with 1 tbsp. boiling water and leave for 5 hours. Drink warm before every meal. The course of treatment is 10 days.
- Blueberry berries and leaves - a decoction is prepared from them by pouring boiling water over dried or fresh raw materials and boiling for 5 minutes. (2 tbsp. raw materials per 250 ml of water). Drink instead of tea.
- Immortelle herb - a decoction helps relieve pain and inflammation. To prepare the decoction, take 1 tbsp. l. dry herbs and a glass of water, cook for 5 minutes. Strain the resulting broth and drink throughout the day.
- Oat decoction helps relieve irritation and restore organ cells. To prepare the product, you need to soak the grains and wait a few days for them to sprout. Sprouted grains need to be dried and ground. Pour the mixture with cold water (1 tablespoon of oats per 1 glass of water) and leave for about half an hour. You need to drink 2 glasses of this product a day.
- Lemon – helps reduce pain. To do this, boil the lemon in water for 5 minutes, then squeeze the juice out of it and mix with raw yolk. Drink the product on an empty stomach and do not eat for three hours after it. Take it five times a day, once every three days. The course of treatment lasts several months.
- Licorice root - to prepare it you need to take 1 tbsp. l. chopped dry licorice root, the same amount of dandelion and burdock leaves. Pour the mixture with 2 cups of boiling water, drink the infusion hot, half a glass 3-4 times a day.
There are also special herbal mixtures used to treat the pancreas. But it is important to take into account that they bring benefits to the body if such preparations are taken regularly and according to the scheme approved by the doctor. Under no circumstances should you practice self-medication with folk remedies for such a terrible diagnosis as pancreatic necrosis.
Toxic (drug-induced) pancreatitis
Drug-induced pancreatitis occurs in less than 5% of cases. The prognosis for this pancreatitis is generally good and the mortality rate is low. The pathogenetic mechanism of drug-induced pancreatitis includes:
- immunological reactions (6-mercaptopurine, aminosalicylates, sulfonamides);
- direct toxic effects (diuretics, sulfonamides);
- accumulation of toxic metabolites (valproic acid, didanosine, pentamidine, tetracycline), ischemia (diuretics, estrogens);
- increased viscosity of pancreatic juice (diuretics and steroids).
Demonstrating interactions between pancreatitis and drugs is usually difficult. Pancreatitis may develop within a few weeks of starting treatment. Rash and eosinophilia may occur. Meanwhile, patients taking valproic acid, pentamidine or didanosine do not develop pancreatitis until many months later due to chronic accumulation of the drug's metabolite.
When restarting treatment, patients should be closely monitored. If symptoms recur, the drug should be discontinued.
What else is important to know about enzyme preparations?
The minimum starting dosage is Creon® 25,000 units, which is stated in Russian recommendations for the treatment of chronic pancreatitis and exocrine pancreatic insufficiency2,5. The number indicates the amount of the enzyme lipase, which helps digest fats. If necessary, the doctor can increase the dosage; in European practice, the required dose per single dose can reach up to 80,000 units8. By comparison, the pancreas of a healthy person produces up to 720,000 of these units during each meal9.
Therapy should be taken seriously, since high-quality “nutrition” of the body is the key to its functioning. How long can a person live without energy from food? With chronic pancreatitis, the body must be supplied with enzymes at every meal, even with a snack. Thus, in accordance with the instructions for the drug Creon®, a full dose is required for a meal (for example, 25,000 units), and half for a snack. Creon® capsules are convenient to use: you can open them and add minimicrospheres to food, thereby selecting the desired dose10. More information about the admission rules can be found here.
Autoimmune pancreatitis
Autoimmune pancreatitis (AIP) is a rare disease that causes fibrotic inflammation of the pancreas. The prevalence of the disease has not been established in detail. AIP is estimated to account for 5-6% of cases of chronic pancreatitis.
Autoimmune pancreatitis is an increasingly recognized disease. Typically, AIP begins with weight loss, jaundice, and diffuse enlargement of the pancreas in imaging studies simulating cancer.
According to international consensus criteria, autoimmune pancreatitis is divided into:
- AIP type 1, or lymphoplasmacytic sclerosing pancreatitis;
- AIP type 2, or idiopathic ductal-centric pancreatitis.
Autoimmune pancreatitis type 1 most often manifests as obstructive jaundice, in 50% of cases. Obstructive jaundice develops due to compression of the distal bile ducts (enlargement of the head of the pancreas) or stricture of the proximal bile ducts.
Obstructive jaundice
Despite intense inflammation, patients do not experience typical abdominal pain or it is mild. Autoimmune pancreatitis type 1 belongs to a spectrum of immunoglobulin (Ig) G4-related diseases that can affect almost all organs of the body (biliary strictures, interstitial nephritis, IgG4-associated glandular exocrinopathy, sialadenitis, retroperitol).
AIP should be suspected in patients with evidence of both pancreatic and hepatobiliary disorders. Elevated serum IgG4 levels are detected in most patients with type 1 AIP.
Typical radiological signs after computed tomography (CT) are:
- diffuse pancreatic parenchyma (sausage-shaped pancreas);
- frame-type rim or focal lesions;
- diffuse pancreatic atrophy.
Endoscopic retrograde cholangiopancreatography (ERCP) reveals diffuse or multifocal narrowing of the pancreatic duct without dilatation. To confirm the diagnosis, it is important to evaluate all tests, but histological examination is considered the standard of diagnosis.
Table 3. Comparison table for autoimmune pancreatitis types 1 and 2
| Type 1 AIP | Type 2 AIP | |
| Age at which the disease develops | About 60 years old | About 40 years old |
| Male | 75% | 50% |
| Damage to other organs/association with IgG4-related disease | 50% | No |
| Inflammation | Small | High (10-20%) |
| Increased serum IgG4 | Contained in approximately 66% | Set at about 25% |
| Histological data: | ||
| lymphoplasmacytic infiltration | Characterized by | Characterized by |
| storiform fibrosis | Characterized by | Characterized by |
| obliterative phlebitis | Characterized by | Rarely noticeable |
| damage to granulocytic epithelium | There is no | Characterized by |
| periductal inflammation | Characterized by | Characterized by |
| IgG4 cells | ≥10 cells/DPL (in area of significant increase) | |
| Response to steroid treatment | 100% | 100% |
| Risk of relapse | Up to 60% | |
Autoimmune pancreatitis is treated with corticosteroids at a dose of 40 mg/day. 4-6 weeks followed by a reduction of 5 mg per week. Inadequate response or relapse is more common in patients with concomitant IgG4-related sclerosing cholangitis. In this case, 2 mg/kg azathioprine is recommended.
List of sources
- Dibirov M.D., Yuanov A.A. Pancreatic necrosis. Diagnostic and treatment protocol. Educational and methodological manual. Moscow, 2012, p. 366
- Ermolov A.S., Ivanov P.A., Blagovestnov D.A. and others. Diagnosis and treatment of acute pancreatitis. M., 2013, “VIDR”, p. 382
- Mitryakov P.S. Modern methods of treating patients with pancreatic necrosis // International Journal of Experimental Education. – 2021. – No. 9-2. – P. 221-224;
- Acute pancreatitis (Diagnosis and treatment protocols) / S.F. Bagnenko [and others]; St. Petersburg Research Institute of Emergency Medicine named after. I.I. Dzhanelidze. - St. Petersburg, 2004.
- Savelyev V.S., Filimonov M.I., Burnevich S.Z. Pancreatic necrosis. MIA, 2008, p. 259
- Sakhno V.D., Mainulov A.M., Vlasova N.V., Bochkareva I.V. Necrotizing pancreatitis, treatment protocols. Annals of Surgical Hepatology, 2005, vol. 10, no. 1, p. 107 – 112
Hereditary pancreatitis
Genetic pancreatitis may present as acute, recurrent, familial, or childhood-induced pancreatitis of unknown origin that later becomes chronic. The incidence of genetically induced pancreatitis is unknown. Some cases remain unidentified. Idiopathic pancreatitis is most common, especially in young people.
Autosomal dominant hereditary pancreatitis is caused by mutations in the PRSS1 gene. Mutations in the CFTR gene are associated with recessive hereditary pancreatitis. SPINK1 entry mutations may act as a disease-modifying factor along with other genetic and environmental factors.
Patients with PRSS1 or SPINK1 gene mutations (hereditary pancreatitis) increase the risk of exocrine pancreatic dysfunction, diabetes, and pancreatic cancer. According to studies, the risk of pancreatic cancer ranges from 7 to 20%. Smoking doubles the risk of pancreatic cancer.
The American College of Gastroenterology agrees that patients with hereditary pancreatitis should be screened annually for pancreatic cancer by magnetic resonance imaging (MRI) or endosonoscopy starting at age 50.
The principles of treatment of hereditary pancreatitis are the same as for pancreatitis of other etiologies. Quitting bad habits (alcohol, smoking) is crucial, since they significantly increase the risk of exacerbations, complications and progression to the terminal stage of pancreatitis. Younger patients with recurrent severe AP or CP can undergo pancreatectomy with autotransplantation of pancreatic islets.
ONLINE REGISTRATION at the DIANA clinic
You can sign up by calling the toll-free phone number 8-800-707-15-60 or filling out the contact form. In this case, we will contact you ourselves.
If you find an error, please select a piece of text and press Ctrl+Enter
3. Symptoms, diagnosis
The clinical picture in each specific case depends on a number of factors. Thus, the type of course and rate of progression, the presence of concomitant diseases, and the predominant localization of the necrotic process (diffuse throughout the gland, with a predominance of damage to the tail or head of the pancreas) are of significant importance. It is quite problematic to identify a universal, typical symptom complex, but most often the following symptoms are present (at least some part or combination of them):
- severe pain in the left hypochondrium, often encircling or radiating to other areas (the characteristic localization easily leads to incorrect self-diagnosis: many patients remain convinced for a long time that they have heart pain);
- nausea, frequent and profuse painful vomiting;
- changes in skin color - redness or, conversely, pallor, unusual rashes on the skin;
- bloating;
- intense sharp pain even with a light touch to the stomach;
- low-grade or febrile temperature.
There are also a number of additional objective symptoms that allow an experienced gastroenterologist to suspect pancreatic necrosis already during the initial clinical examination.
The decisive diagnostic arguments in favor of pancreatic necrosis are the results of tomographic imaging methods, endoscopy (diagnostic laparoscopy), and laboratory biochemical tests.
About our clinic Chistye Prudy metro station Medintercom page!