Symptoms
Hepatic encephalopathy occurs in several stages, during which the severity of clinical manifestations varies. In general, the disease is accompanied by a wide range of mental and neurological disorders. The main ones are described below.
Sleep disorders
. Patients with hepatic encephalopathy initially experience drowsiness. Subsequently, an inversion (radical change) of the normal rhythm of wakefulness and sleep occurs.
Impaired consciousness
. With this disease, there is usually a decrease in the number of spontaneous actions. The patient rarely fixes his gaze, he exhibits apathy and lethargy, and answers questions briefly. As the condition worsens further, a person suffering from hepatic encephalopathy responds only to intense stimuli.
Personality changes
. Patients may experience a loss of interest in the family and childishness. Moreover, these changes often persist even during the period of remission, which indicates the involvement of the frontal lobes of the brain in the pathological process. With hepatic encephalopathy, patients may be in a state of euphoria or a playful mood.
Intellectual disorders
. Impairments in cognitive functions (memory, attention, etc.) can be mild or severe. In severe cases, confusion occurs.
Speech disorders
. In patients with hepatic encephalopathy, the voice becomes monotonous, and speech becomes slurred and slow. In the future, speech impairment may become even more severe (dysphasia).
Flapping tremor
. With this disease, a characteristic flapping (flexion-extension) movement of the hand is observed with outstretched arms and widely spaced fingers.
Coma
. At first it may resemble a normal dream, but later the patient stops responding to external stimuli completely.
Hepatic encephalopathy - symptoms and treatment
The diagnosis of “hepatic encephalopathy” is established by characteristic clinical manifestations, results of laboratory and instrumental studies and psychometric testing data. Further treatment tactics and prognosis of the disease will depend on the degree (stage) of the disease.
Diagnosis of stages I-IV of manifest (clinically pronounced) hepatic encephalopathy is not difficult, since each stage is characterized by certain symptoms [10]. It is much more difficult to recognize the disease at the initial stage: there are no clinical symptoms during a latent course, laboratory parameters are not changed. Therefore, psychometric tests are most often used to detect minimal hepatic encephalopathy.
Recognizing the hidden course of the disease is very important for two reasons:
- firstly, minimal hepatic encephalopathy is very common (50 to 70% of cases in liver cirrhosis);
- secondly, it can lead to a traumatic situation, especially while driving a car, since at this stage of the disease the patient does not respond adequately to extreme circumstances [10][16][17][18].
Hepatic encephalopathy can be suspected in patients with the following symptoms:
- inattention, memory impairment;
- inhibited thinking;
- decreased reaction speed;
- decreased performance;
- disturbance of visual perception;
- irritability.
Laboratory diagnosis involves determining the level of ammonia in arterial blood: it is elevated in more than 90% of patients with overt hepatic encephalopathy. However, during a latent course of the disease, the ammonia concentration may be normal, so this indicator is not an exclusion criterion when making a diagnosis [18].
| Degree of hepatic encephalopathy | Arterial ammonia levels |
| 0 | Norm |
| I | Up to 1.33 from ULN* |
| II | 1.33-1.67 ULN |
| III | 1.67-2 VGN |
| IV | More than 2 ULN |
| *ULN is the upper limit of normal, equal to 60 µmol/l | |
Psychometric testing is primarily used to diagnose clinically silent hepatic encephalopathy. The sensitivity of the tests is quite high - 70-80%.
Over the past 30 years, dozens of simple, accessible psychometric tests have been developed that can be used in various combinations. They are divided into two groups:
- tests for the speed of cognitive reaction (for example, the number connection test - the most common and well-known in clinical practice);
- fine motor accuracy tests (eg line copying test).
When conducting a number connection test, the patient needs to connect the numbers from 1 to 25 with a line. They are printed randomly on a sheet of paper.
To evaluate the test, the task execution time (in seconds), including time spent correcting errors, is used [18]. The interpretation of the results is given in the table.
| Time | Points | Disease stage |
| Less than 40 s | 0 | No |
| 41-60 s | 1 | 0-I |
| 61-90 s | 2 | I-II |
| 91-120 s | 3 | II |
| More than 120 s | 4 | II-III |
The following psychometric tests are also used in the diagnosis of hepatic encephalopathy:
- handwriting recognition test;
- numbers and symbols test;
- line copy test;
- visual memory test;
- alphabetical elimination test;
- linear maze test;
- dots and circles test;
- test for memorizing a pair of words;
- star construction test;
- sequential subtraction test;
- text retelling test, etc. [16][17][18].
Instrumental diagnostics are carried out using the critical flicker frequency (CFF) method. In 2002, it was first used to diagnose minimal hepatic encephalopathy. The study is carried out using the HepatonormTM hepatoanalyzer. In this device, the patient sees what seems to him to be a constant red glow, but is actually a high-frequency flickering [13][15].
During the FFM test, the frequency of the red light, which is initially 60 Hz and is generated as a high-frequency pulse, causes the patient to feel a constant light, and then changes to flickering over time. It is at this moment that the patient needs to press a button on the device. The hepatoanalyzer records the frequency at which the red beam “began to flicker.”
The study is carried out 8-9 times. The average value of the CFM is used for evaluation. Based on the test result, the stage of hepatic encephalopathy is established: values below 39 Hz correspond to minimal hepatic encephalopathy, 35.9-32 Hz - stage I, 31.9-28 Hz - stage II, below 27.9 Hz - stage III [15].
Hepatic encephalopathy can also be diagnosed using EEG - electroencephalography. However, the validity of the results of this study may be affected by medications or decreased sodium levels in the blood [21].
If intracerebral hemorrhage is suspected or differential diagnosis is necessary, CT and MRI of the brain may be required [21].
Differential diagnosis
When diagnosing hepatic encephalopathy, it is important to exclude other causes that could cause the same clinical symptoms. Such reasons include neurological, somatic diseases and various intoxications.
Differential diagnosis is complicated by the lack of distinctive symptoms that would be found only in hepatic encephalopathy. The American Association for the Study of Liver Diseases recommends that disorders that also alter the level of consciousness be considered when making a diagnosis. These include:
- metabolic encephalopathy - associated with metabolic or electrolyte disorders, characterized by low levels of sodium and potassium in the blood or hypoglycemia;
- alcoholic encephalopathy - accompanied by intoxication, withdrawal syndrome (abstinence), developing Wernicke encephalopathy is associated with vitamin B1 deficiency;
- drug encephalopathy - caused by taking benzodiazepines, antipsychotics and opioids;
- neuroinfections - occur under the influence of bacteria, viruses, fungi or protozoa;
- intracranial hemorrhage , subdural hematoma , stroke , tumor or brain abscess - develop against the background of congenital or acquired diseases associated with circulatory disorders [10][13][18].
Treatment
Specific drug therapy
. Treatment may use drugs that reduce the flow of ammonia or neutralize it in the liver. An important role is played by the use of drugs that reduce inhibitory processes in the central nervous system.
Medical nutrition
. Frequent split meals may be indicated for patients with hepatic encephalopathy. It is recommended to take small meals several times during the day, as well as before bed. Feelings of hunger are not allowed. A low protein diet may be preferable for this condition. Daily protein intake can be 1.2–1.5 g per kilogram of body weight.
Liver transplantation
. This may be the only way to treat severe forms of hepatic encephalopathy that cannot be treated conservatively. This syndrome in itself is not an indication for transplantation. However, it may be recommended in cases where hepatic encephalopathy significantly reduces the patient's quality of life and does not respond to other types of therapy. Then transplantation is possible even if the liver is in satisfactory condition.
Read also
Ankylosing spondylitis/ankylosing spondylitis
Ankylosing spondylitis (ankylosing spondylitis) is a chronic inflammatory disease of the spine and joints, accompanied by progressive pain, stiffness and limitation of movements at the beginning...
Read more
Restless legs syndrome
Restless legs syndrome - manifests itself as unpleasant sensations in the lower extremities, mainly in the evening and at night, forcing you to make relief movements with your legs, which leads to…
More details
Pelvic pain
Pelvic pain is pain in the muscles that form the pelvic floor and organs located in the small pelvis, caused by microtrauma, chronic deformation of the sacrococcygeal region due to anatomical…
More details
Syringomyelia
Syringomyelia is a disease caused by the formation of spaces in the substance of the spinal cord filled with cerebrospinal fluid. They expand the spinal cord at the level of the lower cervical and thoracic regions...
More details
Sudden memory loss/transient global ischemia
Transient, that is, temporary memory loss occurs in elderly patients and people suffering from migraines. At the same time, memory for past and present events disappears. But the person is conscious, accessible...
More details
Causes of pathology
The appearance of encephalopathy can be provoked by:
- acute liver disease;
- entry of neurotoxins into the circulatory system;
- cirrhosis of the liver.
Factors contributing to the development of the disease: hepatitis of all types (alcoholic, fatty, toxic, viral), oncology, drug or toxic intoxication, other diseases accompanied by hepatocytolysis.
An excessive increase in the microflora of the obligate intestine or the consumption of excess amounts of protein-rich food can trigger the entry of intestinal neurotoxins into the circulatory system. Liver cirrhosis, complicated by hepatic encephalopathy, is accompanied by the formation of scars (replacement of healthy liver tissue with connective tissue), inhibition of all basic liver functions.
The following factors can provoke the death of hepatocytes and toxic damage to brain cells:
- internal bleeding;
- taking hepatotoxic drugs (without medical supervision and adequate supportive therapy);
- constipation, protein dyspepsia;
- surgical interventions or serious injuries;
- peritonitis provoked by ascites;
- bacterial, viral diseases.
Liver failure is accompanied by a list of pathological changes:
- disturbance of homeostasis, CBS;
- changes in oncotic and hydrostatic pressure.
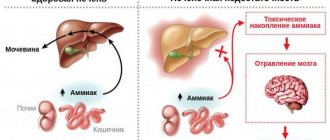
These changes significantly disrupt the normal functioning of astrocyte cells, which account for approximately a third of the weight of brain tissue. Astrocytes are responsible for the normal regulation of the permeability of the cellular barrier, which ensures complete exchange between brain tissues and blood, removing toxins and ensuring the supply of nutrients to brain cells.
In addition to ammonia, toxic damage to astrocytes can cause exposure to false neurotransmitters, magnesium, as well as breakdown products of protein and fatty acids.
Diagnosis of hepatoencephalopathy
If the damage to the liver and brain is alcoholic, the doctor is interested in:
- symptomatic picture;
- establishing the severity of the disease;
- stage of the process.
Based on the data obtained, during a survey and examination, the doctor prescribes additional types of diagnosis of hepatic ecephalopathy.
These include:
- A detailed clinical blood test with determination of the content of erythrocytes, leukocytes, hemoglobin, platelets.
- Biochemistry data with liver tests, bilirubin, alkaline phosphatase, gamma globulin transferase.
- Ultrasound of the parenchymal organs of the abdominal cavity. The specialist is especially interested in the condition of the liver, pancreas, and kidneys.
- Computed tomography is the most informative method of x-ray diagnostics.
- MRI in doubtful cases, as an additional diagnostic method.
- Needle biopsy as the most accurate option for differential diagnosis.