The parasite of humans, cats and dogs, Giardia duodenalis (also known as Giardia lamblia), is distributed throughout the world, and giardiasis, caused by G. duodenalis, is the most common intestinal parasitic disease. The largest number of reported cases occur in children aged 1 to 9 years and adults aged 35 to 44 years. Most cases occur between early summer and early fall and are associated with recreational water sports (such as swimming) and outdoor activities. Humans are the main reservoir of Giardia. The parasite is also found in many animal species, although the role of zoonotic transmission is still unclear.
What is Giardia?
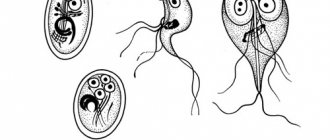
Giardia is a flagellated protozoan that comes in two forms: trophozoites and cysts. The infectious and environmentally resistant form is the cyst. Once ingested by a child, each cyst produces two trophozoites in the small intestine. The separated trophozoites pass through the intestine and form smooth, oval, thin-walled infectious cysts that are excreted in the feces. The duration of removal of a cyst usually has a finite period, but can last for months. Studies have shown that ingestion of 10 to 100 cysts of fecal origin is sufficient for infection. Giardia cysts become infectious immediately after excretion in feces and remain viable for at least 3 months in water at 4°C. Although freezing does not completely eliminate the infectivity of Giardia cysts, heating, drying, or immersing them in seawater renders them nonviable.
“Trouble-sadness-chagrin”, or the dangers of Giardia infection
Giardia waste products contribute to the development of chronic diseases of the gastrointestinal tract, disruption of some components of the immune system, which leads to frequent relapses of skin diseases and allergization of the patient's body. In the gallbladder, where bile is concentrated, Giardia does not live, but has an irritating effect on the biliary tract, causing dyskinesia - impaired motility of the gallbladder and biliary tract. Recently, the influence of Giardia on the pancreas has been shown - Giardia, having a toxic effect, disrupts its exocrine function - the formation of enzymes. If Giardia remains in the body for a long time, then waste products accumulate and chronic intoxication of the body occurs, which can affect any of its organs and systems.
The acute form of the disease is more common in children and lasts 5-7 days, similar to acute gastroenteritis.
The chronic form of infection is observed in adults and school-age children, lasts up to several months and has clinical manifestations.
In 28% of cases of giardiasis in adults, it is asymptomatic, without pronounced clinical manifestations from the gastrointestinal tract. It can occur latently, manifested by a deterioration in the quality of life, a violation of the autonomic nervous system (giardia is called the “parasite of melancholy and sadness”), and the development of allergic and dermatological diseases.
How does Giardia infection occur?
Giardia infection can occur directly through the fecal-oral route or indirectly through ingestion of contaminated water or food. Water contaminated with Giardia cysts appears to be the main reservoir and means of spread of the parasite. Most outbreaks of waterborne giardiasis have been associated with the consumption of untreated or improperly treated surface water. Transmission of giardiasis from person to person often occurs in child care institutions and in families where there are children with diarrhea. Human immune defense is dependent on B cells, with secretory immunoglobulin A playing a major role in immunity. Children with humoral immunodeficiencies, such as X-linked agammaglobulinemia and hypogammaglobulinemia, who develop giardiasis are predisposed to chronic disease.
G. duodenalis infection is more common in certain high-risk groups, including children, staff and visitors of child care facilities, patients and staff of institutions for people with developmental disabilities, people who drink contaminated drinking water or water from lakes, rivers or insufficiently treated swimming pools, travelers to endemic areas of the world, close contacts of people with Giardia, people taking antibiotics, and people in contact with domestic and wild animals (eg dogs, cats, cattle, deer and beavers).
Analysis transcript
Giardia test results are interpreted depending on the method used.
Microscopic analysis of stool for Giardia
- Positive result – Giardia cysts were found in the stool.
Meaning. Carriage of the parasite G. Lamblia. Acute or chronic giardiasis.
- Negative result – no Giardia cysts were detected.
Meaning. The patient is not infected with Giardia.
G. lamblia antigen test
- Positive result – antigen detected.
Meaning. Carriage of the parasite G. Lamblia. Acute or chronic giardiasis.
- Negative result – no antigen detected.
Meaning. The patient is not infected with Giardia.
Blood test for Giardia decoding
The ratio of antibodies to Giardia antigens in the blood plasma is determined.
- Negative result – 0.85 OPD. Lack of lamblia in the body.
- Positive result – ≥ 1 OPD. Giardiasis or parasitic carriage.
- Doubtful – 0.85-1 OPD. Requires re-examination.
If, during a comprehensive study, a stool test for Giardia reveals cysts of the parasite, and there are no specific immunoglobulins in the blood, this indicates a lack of immunity and is an unfavorable prognostic sign in terms of the effectiveness of treatment. Such a patient requires individual treatment methods.
What are the symptoms and signs of giardiasis?
The incubation period of the disease usually lasts from 1 to 2 weeks, averaging 7 days. Infection with G. duodenalis can cause a wide range of clinical manifestations. Children usually present with short-term, acute, watery diarrhea with or without low-grade fever, nausea, anorexia, and abdominal pain. In other cases, the infection follows a longer, intermittent course, characterized by foul-smelling stools associated with flatulence, bloating, and anorexia. Malabsorption combined with anorexia can lead to significant weight loss, stunted growth, and malnutrition in children. The stool may initially be large and watery, but later become greasy and foul-smelling. There is no blood, mucus, or leukocytes in the stool. Varying degrees of malabsorption may occur, and abnormal bowel movements may alternate with periods of constipation and normal bowel movements. Post-infectious lactose intolerance can occur in 20% - 40% of patients. This syndrome may take several weeks to resolve and may contribute to malnutrition in children. Malnutrition and repeated episodes of Giardia infection in the early years of life are associated with cognitive decline in late childhood. In addition, a proportion of children will develop chronic gastrointestinal symptoms such as post-infectious irritable bowel syndrome (PI-IBS).
Asymptomatic giardiasis is also common. Extraintestinal invasion can occur when trophozoites migrate into the bile or pancreatic ducts. Extraintestinal manifestations were previously considered uncommon, but recent studies suggest that one third of patients will exhibit long-term extraintestinal symptoms, including ocular, muscular, and metabolic complications. The subsequent development of reactive arthritis may also be associated with giardiasis.
Preparing for analysis
Patients are often interested in how to get tested for Giardia?
It depends on the method of research. When donating blood for immunology, blood is taken from a vein.
Before doing this, it is not recommended to:
- eat food within 10 hours before the test;
- eat fatty and spicy foods and dishes;
- the day before the test, drink juices, coffee, tea, and alcoholic beverages;
- active physical activity.
A blood test for Giardia in children is performed in the same way as in adults.
Diagnosis of giardiasis
A definitive diagnosis of Giardia infection is made by detecting trophozoites or Giardia cysts in stool samples, intestinal contents, or small intestinal tissue by microscopic examination using staining techniques such as trichrome. Also used are direct fluorescent antibody tests (DFA), detection of soluble stool antigens using enzyme-linked immunosorbent assay (EIA), and the use of molecular methods, including polymerase chain reaction (PCR). EIA or multiplex PCR is the main currently recommended diagnostic methodology. There are currently commercially available multiplex PCR panels for the detection of gastrointestinal pathogens, including Giardia. These tests are highly sensitive (92% to 100%) and specific (96.9% to 100%) and can simultaneously detect multiple GI pathogens.
Identification of both trophozoites and cysts can be made on direct smears of concentrated stool samples. Correctly performed direct examination of stool allows a diagnosis of giardiasis to be made in 70% of patients during a single examination and in 85% during a repeat examination. Identification of Giardia can be difficult due to the periodic release of cysts. Stool samples should be examined within 1 hour of collection. Trophozoites are more likely to be present in unformed stool due to rapid passage through the intestine. Cysts are stable outside the gastrointestinal tract.
If giardiasis is suspected and stool tests are negative, aspiration, biopsy, or both should be performed during endoscopy of the duodenum or upper jejunum. In a fresh specimen, trophozoites can usually be visualized on a direct wet mount. Histological evaluation of duodenal biopsy specimens has low sensitivity for detecting infection, however this diagnostic approach may be necessary in patients with clinical characteristics of Giardia infection but negative stool and duodenal fluid specimens. The commercially available Entero-Test is an alternative method for direct collection of duodenal fluid.
Treatment of giardiasis
Treatment of giardiasis has 2 main goals – eliminating the pathogen and correcting the patient’s well-being.
To implement them, a diet is prescribed that includes avoiding eating fried and smoked foods and reducing the size of portions. Drugs prescribed for the treatment of giardiasis:
- enterosorbents – substances for binding free toxins and waste products of microorganisms;
- probiotics and prebiotics - these drugs restore normal microflora and stimulate its independent growth in the intestines;
- antimicrobial agents from the group of nitroimidazoles and nitrofuran derivatives.
In case of dysfunction of the pancreas and/or gall bladder, enzymes or cholekinetics may be additionally prescribed.
Prevention of giardiasis involves simultaneous treatment of all contacted people (parents, brothers and sisters), strict adherence to personal hygiene rules, washing vegetables and fruits before eating and avoiding drinking raw water.
“SM-Doctor” is an advanced medical institution that offers young patients a full range of diagnostic and treatment services. Thanks to extensive experience working with children, our specialists will help get rid of giardiasis in the shortest possible time and return the child to a full life. Contact professionals for qualified help!
Treatment of the disease
Effective antiparasitic therapy is the main initial method of treating Giardia in children and adults. Patients should receive supportive care with hydration, correction of electrolyte abnormalities, and nutritional supplements. Drugs that reduce intestinal motility (antidiarrheals) should be used with caution in young children. Patients with chronic diarrhea should be monitored for malabsorption leading to wasting.
The therapeutic efficacy of metronidazole against Giardia has led to the development of other nitroimidazole derivatives such as tinidazole and secnidazole. The advantage of these drugs is that they have a longer half-life than metronidazole, making them suitable for single daily dose treatment. A single dose of 2 g (or an equivalent pediatric dose of 50 mg/kg in a single dose) of tinidazole has demonstrated cure rates of 80% to 100%. Cure rates for patients with giardiasis have been shown to be consistently higher with the use of tinidazole than with other antiparasitic drugs such as metronidazole, nitazoxanide, mebendazole, albendazole, and chloroquine. Tinidazole is approved for use in children aged 3 years and older. The drug is available in tablets that can be crushed into a flavored syrup for patients who are unable to swallow tablets.
Metronidazole was recognized as a therapeutic agent against giardiasis in 1962. Since then, clinicians have used metronidazole and other nitroimidazoles as the mainstay of therapy for giardiasis. Metronidazole is the drug most commonly used to treat giardiasis worldwide. Children have been included in many clinical trials of metronidazole with results similar to those in adults (average effectiveness of 94%) with 5-day and 10-day course regimens. Metronidazole is not available in standard liquid form, but a suspension can be prepared by thoroughly crushing metronidazole tablets using glycerin as a lubricant and suspending the mixture in a flavored syrup.
Side effects of tinidazole are not as common as those of metronidazole. The most common side effects of metronidazole treatment include headache, dizziness, nausea, and a metallic taste in the mouth. Nausea occurs in 5–15% of patients receiving standard multi-day courses. In addition, metronidazole has been associated with reactive pancreatitis, central nervous system toxicity at high doses, and transient reversible neutropenia.
GIARDIASIS IN CHILDREN
Giardiasis is widespread, and the infection of children with Giardia, especially at early and school age, is several times higher than the corresponding indicators in adults. Among children attending children's groups (nurseries, kindergartens, schools), the incidence of Giardia is, according to various authors, up to 33%.
The clinical symptoms of giardiasis consist of several symptom complexes: syndrome of gastrointestinal tract damage and nutritional disorders, intoxication syndrome, including damage to the central nervous and autonomic nervous systems, allergic syndrome (damage to the skin and respiratory organs).
Gastrointestinal syndrome. The main clinical symptoms of giardiasis are diagnosed from the gastrointestinal tract, since giardia parasitizes the human intestine. The clinical picture of the disease is dominated by enteral disorders, the manifestations of which largely depend on the age of the child. Since the localization of Giardia is the small intestine, where absorption of nutrients occurs, some children develop malabsorption syndrome in the form of protein-energy and polyhypovitaminosis deficiency.
Symptoms of intoxication are directly dependent on the massiveness of the invasion, the severity of the disease, and its duration. Intoxication with giardiasis can manifest as hepatolienal syndrome and enlargement of peripheral lymph nodes, tonsils and adenoids. Long-term intoxication with giardiasis can also lead to the appearance of neurological symptoms such as teeth grinding (bruxism), tics. The effect of Giardia waste products can have a depressing effect on the central nervous system and cause rapid fatigue, decreased performance, and emotional tone. It is not for nothing that the discoverer of this pathogenic protozoan, D. F. Lambl, called it “a parasite of melancholy and sadness.”
Allergic manifestations on the skin, as well as from the respiratory, gastrointestinal tract and blood can occur with any form of giardiasis, regardless of the severity and severity of the process. It has long been known that in response to the introduction of a parasite, the level of IgE and the level of eosinophils in the peripheral blood increase [3, 4, 7] - hyperproduction of IgE and eosinophilia are the oldest phylogenetic methods of antiparasitic defense. This is precisely what can explain the fact, well known to clinicians, that parasitosis increases allergic symptoms in children with atopy and other forms of allergic manifestations.
It should be noted that the diagnosis of giardiasis is difficult due to the lack of pathognomonic symptoms, and giardiasis itself either overlaps with other diseases, or all the clinical manifestations of this parasitic infection are explained by other different reasons [4].
Examination for giardiasis is indicated for the following conditions (N.P. Shabalov, Yu.I. Staroverov, 1998) [5]: the presence of diseases of the digestive tract, a tendency towards their chronic course with frequent but moderate exacerbations; neurocirculatory dysfunction, especially in combination with gastrointestinal disorders; persistent blood eosinophilia; allergic manifestations.
According to the literature, immunological methods, for example, determination of antibodies to Giardia in blood serum, have high sensitivity and specificity.
Detection of specific IgM and IgG to Giardia antigens using immunofluorescence analysis (ELISA) is possible from the 12th–14th day of the disease.
After debridement, IgM quickly disappears. Their detection indicates giardiasis; IgG persists for up to 2 months after sanitation.
However, while the pathogenic properties of the parasite have not been sufficiently studied, in particular, giardiasis toxins have not been identified, it seems premature to rely only on the results of an immunological study in diagnosing giardiasis.
According to our observations, in children with persistent, long-term giardiasis, antibodies to giardia may not be detected in the blood serum. I.V. Kuimova and T.N. Tkachenko (2002) also found antibodies in less than half of children infected with Giardia [2], which, in our opinion, may indicate the ineffectiveness of humoral defense mechanisms.
Therefore, the absence of specific immunoglobulins in children with repeated detection of Giardia cysts is a poor prognostic sign and requires the doctor to use individual treatment regimens. Quite often, antibodies to Giardia are not detected in children with lymphatic-hypoplastic diathesis.
In modern conditions, the diagnosis of giardiasis is carried out by the routine method of fecal microscopy, but this method is largely subjective, much depends on the correctness of all stages of the study.
Stool samples are not always delivered to the laboratory “warm”, which is explained by the peculiarities of working with children: the child cannot empty his bowels when ordered. This obstacle can be overcome by using preservative solutions such as phenol-formalin mixture - Borrows reagent.
Proper preparation of the specimen for microscopy is also of great importance. The material must be applied to the glass in a thin, transparent layer, otherwise Giardia cysts are very difficult to see in the thickness of the detritus. Microscopy should be carried out immediately after preparation of the drug.
Under in vitro conditions, cysts can change their shape - “shrink”; their shell becomes uneven and merges with detritus, which makes identification much more difficult.
There is another “natural” obstacle that complicates the diagnosis of giardiasis - the “phenomenon of intermittent cystic discharge.” A child infected with giardiasis does not excrete cysts every day - the interval in the excretion of cysts is 8-14 days; to confirm the diagnosis in a laboratory, some persistence must be shown. Repeated multiple microscopy of feces is recommended.
It is known that the creation of unfavorable conditions promotes cyst formation and the release of cysts. It was noted that when choleretic and antigiardiasis drugs are prescribed, cysts are found much more often.
Various drugs are used as means of “provocation”, taking into account the age of the child, the severity of clinical manifestations and the presence of concomitant indications: infusion of corn silk, homeopathic drug cholevit, makmiror, furazolidone, metronidazole. During a single examination, Giardia cysts were detected in 92.5% of children in whom giardiasis was clinically suspected. Thus, following simple rules can improve the diagnosis of giardiasis.
Even greater persistence is required in the treatment of giardiasis. When prescribing antiprotozoal drugs, it should be remembered that therapy for this infection is aimed not so much at complete eradication of Giardia from the intestines, but at reducing the clinical manifestations of intoxication, gastrointestinal and allergic syndromes.
The effectiveness of the use of antigiardiasis drugs to reduce the clinical manifestations of allergic syndrome is quite pronounced. Using Macmiror or metronidazole as initial therapy, we noted clinical improvement within the first 7–10 days. In 85% of children with atopic dermatitis, a weakening of skin manifestations was noted; the phenomena of bronchial obstruction disappeared or decreased in 86% of children: shortness of breath and prolongation of exhalation disappeared, cough softened; the symptoms of allergic conjunctivitis decreased in all children.
A positive effect was observed both when prescribing Macmiror and when prescribing metronidazole. Unlike metronidazole and furazolidone, in the elimination of which the liver participates, Macmiror is almost completely eliminated by the kidneys, and the detoxification reserves of the liver are not affected.
It should be remembered that when prescribing medications effective against Lamblia intestinalis, such as metronidazole and furazolidone, on the second or third day of treatment the child’s well-being may deteriorate in the form of nausea, vomiting, itching, and skin rashes. Under the influence of treatment, the products of massive decay of the parasite are absorbed into the blood and become the cause of increased intoxication and sensitization of the body. The accumulation of parasite decay products in the intestines contributes to changes in the pH of the internal environment and the development of dysbiosis. This reaction is called the Yarisch-Geixheimer reaction; as a rule, it lasts no longer than 5–7 days. To reduce its manifestations during the course of treatment, it is recommended to carry out tubages with osmotic laxatives - 25-30% solution of magnesium sulfate, sorbitol, xylitol 1-2 times a week in children over 5-7 years old. Osmotic laxatives interfere with the absorption of parasite breakdown products and weaken the Jarisch-Geixheimer reaction.
Due to the danger of increased intoxication in the first days of treatment, it is not advisable to use antigiardiasis drugs in short courses. The duration of taking antigiardiasis drugs for 5–7 days does not lead to eradication of the parasite; after discontinuation of the drug, the clinical manifestations of the disease resume, and as a result, such a course may not lead to clinical improvement.
Reducing the manifestations of the Yarisch-Geixheimer reaction is also facilitated by the administration of systemic enzyme therapy drugs, in particular Wobenzyme, which is a complex of highly active enzymes of plant and animal origin. The drug is usually prescribed 3-5 tablets 3 times a day 40 minutes before meals, starting with the second 10-day course of treatment with Macmiror or metronidazole, for the entire period of the main and anti-relapse courses.
It should be noted that, firstly, in conditions of deepening microbiocenotic imbalance of the intestine, increasing endo- and exotoxicosis leads to sensitization of the body and creates the risk of the occurrence and development of food allergies (Fig.). The direct systemic and local participation of multienzyme drugs in the metabolism and absorption of toxins and sensitins significantly improves this situation.
Secondly, the plant components of the drug (papain and bromelain) are active in the colon, where the pH of the environment is shifted to the acidic side. This ensures deep proteolysis of proteins and glycoproteins, which apparently deprives opportunistic (and pathogenic) auxotroph microbes of growth factors and food substrates, while unpretentious components of a normal, balanced intestinal microbiocenotic system (for example, sugar-lytic microbes ) do not require proteins for their vital functions.
Thirdly, the immunomodulatory properties of the multienzyme drug, primarily the stimulation of macrophages, make it possible to resist antigenic hyperstimulation with subsequent depletion of local immunity [8].
Having summarized the experience of observing more than 400 patients with giardiasis, we believe that in order to obtain the maximum effect, it is advisable to prescribe an anti-giardiasis drug in two 10-day courses with a 5-day break between them.
During this time, we observed a decrease in clinical manifestations of the gastrointestinal tract in more than 95% of children and a persistent decrease in allergic manifestations (skin, respiratory, etc.) in more than 80% of children.
The course of treatment carried out does not always lead to eradication of the parasite; we detected Giardia cysts in the stool on the 20–25th day of treatment with Macmiror and metronidazole. In control tests, Giardia cysts are detected much more easily than before treatment, even with complete clinical well-being. Apparently, this phenomenon is due to the fact that during the treatment the immunological properties of the body increase, which contributes to the “expulsion” of Giardia.
When cured from giardiasis, there remains a high risk of re-infection, since, firstly, the prevalence of this infection in the population is quite high, and secondly, all researchers unanimously recognize the possibility of re-infection. In many patients, we observed a return of clinical manifestations over the coming weeks and months.
On the other hand, the absence of labia cysts in the stool cannot serve as a criterion for successful treatment. The main indicator of recovery is the disappearance of clinical symptoms: cessation of abdominal pain, restoration of body weight, cleansing of the tongue, elimination of skin manifestations, normalization of stool and liver size.
An increase in liver size is one of the most dynamic symptoms of giardiasis intoxication. In the vast majority of patients, the painless and elastic edge of the liver protrudes from under the edge of the costal arch by 1 - 4 cm. On the 5-7th day from the start of treatment, the size of the liver usually normalizes (i.e., the edge of the liver is palpated along the edge of the costal arch). If during treatment it was not possible to achieve eradication of the parasite, an increase in liver size occurs 9–14 days after the end of treatment. In this case, repeated anti-relapse courses are indicated: a single dose of metronidazole in an age-appropriate dosage at night, in the morning a tube with an osmotic laxative. As a rule, at least 4–6 anti-relapse courses are carried out. Over this period of time, it is possible to achieve a stable reduction in allergic manifestations in more than 90% of patients.
Children in whom Giardia cysts are repeatedly detected by coproscopy, and immunological testing (ELISA) does not reveal antibodies to Giardia (i.e., humoral protection against the parasite is ineffective), constitute a special group that requires immunocorrection, which we carried out with the drug Wobenzym. Our choice was also due to the fact that many patients with giardiasis - both children and adults - had various manifestations of maldigestion syndrome - digestive disorders in the small intestine.
We observed 27 children aged 1 year and older. The clinical picture was dominated by: maldigestion and malabsorption syndrome with retardation in physical development in all children, severe abdominal pain syndrome in 23 children. All children received traditional drugs Macmiror and metronidazole in two repeated courses of 10 days and anti-relapse courses with tinidazole. Starting from the second 10-day course of Macmiror, 20 children were prescribed Wobenzym for 2-3 months. Children received the drug at the rate of 1 tablet per 5 kg of body weight per day. In the group of children who received Wobenzym for 2-3 months, body weight restoration occurred in 17 children, abdominal pain syndrome decreased in 16 out of 17. The number of anti-relapse courses with tinidazole was reduced to 2. In the group of children who received treatment only with antigiardiasis drugs for that During the same period, pain decreased in 4 out of 6, and complete restoration of body weight occurred in 3 children. In this group, 4 anti-relapse courses with tinidazole were required. The use of Wobenzym made it possible to more quickly restore body weight, reduce pain, and reduce the number of anti-relapse courses with tinidazole [1].
To consolidate the positive effect of treatment, medicinal herbs with regenerating, epithelizing, anti-inflammatory, choleretic and enveloping effects are widely used. In the summer, resort therapy is indicated: sea bathing, sun and air baths. When clinical remission of the disease was achieved, the children continued to be monitored and, when typical symptoms of the disease reappeared, received anti-relapse courses of Macmiror. This procedure for managing patients with giardiasis made it possible to lengthen clinical remission in children under 6 years of age with atopic dermatitis and respiratory allergies.
For questions regarding literature, please contact the editor.
T. Yu. Bandurina, Candidate of Medical Sciences, Associate Professor G. Yu. Knorring, Candidate of Medical Sciences MAPO, St. Petersburg
Preventing relapses of giardiasis
There are no known pharmacological agents that effectively prevent relapse of giardiasis. Reinfection often occurs in endemic areas or in situations where hygiene levels are poor or contaminated water (such as private wells) is not properly treated. Re-infection can be prevented by consistent hand hygiene, especially after bowel movements and handling soiled diapers. You should also practice hand hygiene before preparing and eating food. To reduce the risk of disease transmission, children with diarrhea should be removed from childcare settings until the diarrhea stops. Children with giardiasis should not go to recreational water facilities for 2 weeks after the symptoms disappear.
Who is to blame for the disease?
For many years, this disease did not deserve special attention from doctors, although Giardia itself has been known since the middle of the last century. They were first described by the Russian scientist D.F. Lambliy in 1959. Giardia is the name given to pathogenic protozoa that live in the lumen of the small intestine; they are single-celled and equated to the same class as amoebas. These are protozoan pathogens. That is, they cause a disease called giardiasis.
For many years, scientists and doctors believed that giardiasis could only occur in a weakened or very young child, and in healthy children, in adolescence and adulthood, the presence of giardia was not considered a disease, but was thought of as a simple carriage. However, it was later proven that the presence of Giardia in the body is harmful. It’s just that adults and teenagers have a stronger immune system that tries to contain the harmful effects of diabetes, and the body knows how to cope with disturbances in the functioning of organs. Therefore, carriage in this period of time is unacceptable.
Giardiasis is a contagious disease, and the so-called carrier, even in one day, can release a huge number of cysts, which, if hygiene rules are not followed (which children almost cannot observe), will be enough to infect entire classes or groups of kindergartens.
Giardia is a parasite of humans and some animal species; they do not live freely in nature. Each biological species has its own parasitic species of Giardia, which are not dangerous for other species; a child cannot get sick from pets (however, this does not mean that hygiene measures in dealing with them should be neglected).
This is the only type of parasite that lives in the aggressive environment of the small intestine, and for them this is the optimal environment for reproduction. If unfavorable living conditions occur, when they enter the underlying parts of the intestine, Giardia turns into cysts with a dense shell. This allows them to survive unfavorable conditions and find new owners. In the form of cysts in the external environment, they can be stored for years.
Recommendations for the prevention of giardiasis
Because giardia is most often spread through contaminated water and food or contact with an infected person or animal, you should avoid using untreated water sources and wash your hands with soap and water after handling potentially contaminated fecal material or contact with an infected person or animal. Alcohol-based gels are ineffective against Giardia cysts and should not be used as a substitute for hand washing when there is a risk of Giardia infection.
In the hospital, standard precautions include wearing gloves and washing hands after removing gloves.
Before traveling to areas where water may be contaminated or the safety of drinking water is questionable, travelers, tourists, and vacationers should be informed of methods to make the water safe to drink.
These measures include using bottled water, disinfecting the water by heating it to a boil for 1 minute, or using a filter that has been tested and certified to NSF Standard 53 or Standard 58 to reduce cysts and oocysts. Outbreaks of waterborne giardiasis can be prevented by a combination of proper filtration of water sources, chlorination, and maintenance of water distribution systems. Travelers should also be advised of the possibility of transmission of giardiasis through the use of contaminated water for recreational purposes (eg, lakes, rivers, inadequately treated swimming pools). Call a doctor at home Make an appointment with a doctor or call +7 (812) 331-17-74
Sources and mechanism of infection by Giardia cysts
Sources of Giardia infection are:
- drinking water,
- open bodies of water contaminated with untreated sewage,
- unwashed fruits, vegetables,
- dirty hands.
The entry point for parasitic infection is the gastrointestinal tract. The infectious dose is from 100 cysts. The incubation period for the development of infection is up to 25 days.
How does Giardia infection occur?
Giardia cysts from the environment enter the gastrointestinal tract of a person or animal, and they are not affected by the acid of gastric juice, the shell of the cysts dissolves only under the influence of intestinal juice and they pass into vegetative forms that live in the duodenum and jejunum, multiply quickly and damage the mucous membrane of the small intestine. Vegetative forms of Giardia are sucked onto the microvilli of the small intestine, where digestion and absorption of nutrients occurs and thus parasitize, using the nutrients of a sick person. Up to 1 million Giardia can parasitize per 1 cm2.
Treatment of helminthiasis
The principles of deworming are determined by the type of parasite that caused the development of the disease. The main goal of treatment and preventive measures is to reduce the number of helminthic infestations in the intestines and strengthen nonspecific immunity. The following groups of medications can be used to kill worms:
- anti-nematodes – “Vermox”, “Mintezol”;
- anticestoid - Praziquantel, Phenasan;
- anti-trematodes - “Khloksil”, “Azinox”.
Many of the above medications can cause side effects such as anemia and intestinal bleeding. To prevent deterioration of well-being during therapy, it is advisable to use Neopagen, Methyluracil, Ursosan, Colespitol.
Why is Giardia bad?
With giardiasis, the entire body suffers in one way or another, since Giardia has special effects. The incubation period is usually short, lasting on average one to two weeks. Giardia has a special protein on its surface that causes toxic and allergic reactions in the baby's body. They activate the immune system to an excessively sharp response, and the child then begins to develop eczema, dermatitis, and asthma attacks. In addition, Giardia must eat something, which means they will begin to overeat the child and deprive him of nutrients - lactose, glucose, as well as B vitamins and vitamin C. Because of this, children lose weight and their appetite is impaired.
As a result of the massive proliferation of Giardia, toxic substances are released in the intestines that negatively affect the growth and reproduction of beneficial microflora - lactobacilli and bifid flora are replaced by actively growing opportunistic microbes and fungi of the genus Candida. Due to the imbalance of microbial balance, digestion and absorption of nutrients are further disrupted.
Previously, there was an opinion that Giardia lives in the bile ducts, but today this theory has been proven untenable - Giardia is detrimental to the action of bile. Therefore, the role of Giardia as a cause of hepatitis (inflammation of the liver) and the development of cholangitis (inflammation of the bile ducts) has not been proven. However, Giardia negatively affects the process of bile secretion and can contribute to the formation of the biliary tract due to the fact that inflammation occurs in the duodenum and due to the influence of toxins produced when the parasite multiplies.
In addition, a strong allergenic or reflex effect of Giardia is also detected. Giardia, due to its irritating effect on special points of the intestine, begins to change the composition of the blood, causing eosinophilia, the total number of eosinophils increases (from 8 to 10-15) and general leukocytosis. In addition, Giardia disrupts the functioning of the nervous system, manifested in sympathicotonia or vagotonia, or in the cardiovascular system - heart damage (cardiopathy).
As a result of a long stay of a large number of Giardia in the intestines, a decrease in immunity is observed, and chronic self-poisoning is formed (this is called chronic endogenous intoxication syndrome). This leads to damage to many systems and organs of the child, which are then treated by doctors for a long time and persistently.
In an ordinary child, with very strict adherence to all hygiene measures and a strong immune system, Giardia infection can resolve on its own within 5-6 weeks, but this will be possible mainly in adolescence and in no more than a quarter of cases. In children, giardiasis is usually mistaken for various diseases for a long time and it may not be detected for a long time.
Treatment regimen
It is necessary to begin treating giardiasis from the moment the pathology is identified. The basis of diagnosis is a stool test for oocytes, a complete blood count and immunological tests. Treatment of giardiasis in children consists of three main stages:
- Preparatory, aimed at reducing intoxication of the body. For this purpose, children are prescribed choleretic drugs, sorbents, and enzymes. At the same time, it may be necessary to use antispasmodics, as well as medications to strengthen the immune system. Diet plays an important role. Patients will have to give up simple carbohydrates. Sweets, flour products, and whole milk are strictly prohibited.
- Antiparasitic therapeutic therapy. At this stage, the attending physician selects medications individually. In many ways, the choice is determined by the child’s condition, as well as existing contraindications. The doctor describes in detail the dosage regimen, dosage, and duration of the treatment course. The disease in children can be cured with the help of drugs such as Metronidazole, Ornidazole, Macmiror, Furazolidone, Nemozol.
- Recovery stage. Its task is to strengthen the body's defenses and eliminate disorders caused by the pathological activity of Giardia. Children are prescribed multivitamins, as well as prebiotics to restore the gastrointestinal microflora.
A specialist will help you create a treatment menu. The basis of the diet should be vegetables, slimy porridges, dried fruits, and vegetable oils. Pumpkin and pumpkin seeds are considered a particularly valuable product for parasitic infections. To enhance peristalsis, it is recommended to eat greens, vegetable and fruit purees, and fresh fruits.
Compliance with the drinking regime is also important. A sufficient amount of fluid will help you quickly get rid of the symptoms of intoxication. Traditional treatment will help improve the child’s condition and speed up the recovery process. For giardiasis, cucumber tincture and a decoction of dandelion roots are very popular.
To prepare the infusion you will need seeds from an overripe vegetable. They should be mixed with crushed pulp and pour boiling water over it. To prepare a decoction, the crushed dry roots of the plant are poured with boiling water, boiled over a fire and consumed chilled and filtered.
So, the prevention of giardiasis lies in observing the rules of personal and general hygiene. Of course, it is impossible to ensure that a child does not put his hands in his mouth, but parents can teach him to comply with sanitary standards and strengthen the body. The prognosis of the disease is favorable with timely diagnosis. Effective treatment involves the use of antiparasitic drugs, adherence to dietary nutrition and strengthening the immune system.
How and where do people usually become infected with giardiasis?
Giardiasis is a widespread infection, found in all countries of the world and the incidence rate is higher in countries with a low level of sanitary culture. Russia is not in last place on this list; up to 30-40 thousand cases of illness are detected annually, but the real numbers are five times higher. Children, according to statistics, make up about a quarter of the sick, and in kindergartens and schools, according to infectious disease specialists, the incidence reaches 60-70%. Children from two to six years of age usually get sick, although cases of the disease can occur even in infants in the first months of life. It is believed that up to 20% of acute intestinal infections in children are due to giardiasis.
A child can constantly excrete Giardia cysts with feces; this happens when the immune system is weakened and it is impossible to contain the proliferation of parasites due to it, or the excretion of cysts occurs in periods, every 10-14 days. This is due to the cyclical development and seasonality of the disease, since Giardia most often flourishes in the warm season. In addition, they occur more often when consuming dairy and carbohydrate-rich foods. Giardia cysts are excreted in feces and can be stored in soil or water for many months. But live (or they are called vegetative) forms die when leaving the small intestine in half an hour to an hour. That is why giardiasis is extremely difficult to recognize by stool analysis.
The most unpleasant thing for the development of giardiasis is insensitivity to almost all household disinfectants (and household disinfectants, by the way), even chlorine does not kill Giardia cysts. They are resistant to acid and alkali; they can only be destroyed by a very low temperature below -20-25°C, or a very high temperature - that is, the water must be boiled for at least 10 minutes. Giardia cysts cannot tolerate sunlight, ultraviolet radiation and quartz - they die within half an hour.
The route of infection with Giardia is classic for intestinal infections - the fecal-oral route. Simply put, through dirty hands when playing in sandboxes contaminated with animal feces and sewage, infection is possible through shared utensils and toys. Children who bite their nails, pens or suck their fingers almost 100% have Giardia. The second important route of infection is water. And this is not only swimming in reservoirs and swallowing water, but also drinking unboiled tap water.
Factors that contribute to the rapid growth and reproduction of the parasite are considered to be carbohydrate nutrition, lack of protein in food, impaired secretion of bile and its low concentration, a high level of digestion near the intestinal walls, decreased acidity of gastric juice and impaired intestinal microflora. But Giardia does not like the consumption of proteins and acidic drinks.
Infection
Outbreaks of the disease usually occur in the spring and summer. Parasites are spread by the fecal-oral route. They pass not only from person to person. You can get infected from cats, dogs and guinea pigs. A child can easily pick up parasites simply by playing in the sandbox or after contact with an animal.
Infection can occur even during the process of caring for your beloved pets, for example, when washing the litter box. The habit of putting dirty fingers in your mouth and biting your nails can also cause the infection to spread. In order for giardiasis to develop in the body, the penetration of just one individual is sufficient.
Cysts can enter a child’s body in three ways:
- Water. When using tap water for drinking. Also, when swimming in a pond, a child may accidentally swallow water.
- Domestic. Parasites can live on toys, clothes, dishes, towels, door handles, and other household items. Pathogens can easily enter a child's body through unwashed hands. That is why, from early childhood, it is important to instill in children the rules of personal hygiene.
- Food. After eating poorly washed or insufficiently heat-treated foods. Experts recommend not only washing vegetables and fruits before eating, but also pouring boiling water over them.
Infection of a person with Giardia (shown in the photo) may not manifest itself in any way for a long time
Giardiasis is often observed in children who live in private houses with an outdoor toilet. An infected child actively spreads parasites around him. Through feces, Giardia gets onto the skin, and then onto personal items, water and food. Sources of infection are not only patients, but also carriers, as well as some mammals (dogs).
In order to become infected, it is enough to ingest a very small amount of cysts. A person with giardiasis excretes millions of parasites in their feces per day, so one can only imagine the likelihood of infection if hygiene standards are not followed.
Interesting! Experts note that if a child’s diet is dominated by a large amount of sweets and carbohydrates, parasites multiply much faster. If he eats more protein and plant foods, then the pathological process slows down.
It is not necessary that clinical symptoms appear after parasites enter the intestinal tract. A person can become an asymptomatic carrier of the disease. Several factors may influence the development of parasitic infestation:
- state of the immune system;
- presence of problems in the functioning of the biliary system. If there is not enough bile secretion in the small intestine, it will be easier for Giardia to take root;
- acidity level in the stomach. The lack of hydrochloric acid creates ideal conditions for the life of parasites.
When a carrier state develops, cleansing the intestinal tract from pathogens can occur spontaneously, without any treatment. In this case, self-infection should not occur. To do this, a person must properly observe the rules of personal hygiene. If parasites take root in the intestines and actively multiply, this causes digestive problems, inflammation and a lack of nutrients in the body.
Giardiasis can cause painful abdominal cramps. This occurs because pathogens irritate the nerve endings of the organ. Giardia metabolic products can provoke allergic reactions. In addition, these substances poison the body, causing signs of intoxication. An important aspect in the prevention of giardiasis is the fight against household insects: cockroaches, flies, bedbugs.
The risk of developing giardiasis in children increases in the following cases:
- incorrectly composed diet (insufficient consumption of protein foods);
- operations on the abdominal organs;
- weakened immune system;
- disturbances in the functioning of the bile ducts;
- reduced enzymatic activity in the gastrointestinal tract.