Home > Hand injuries
Fractures of the hand bones are the most common fractures among all the bones of the human skeleton. Such fractures occur in the workplace or at home as a result of being hit by or about heavy objects, during a fall, as well as when playing various sports.
Most of these fractures are treated conservatively without surgery, however, some fractures: open, intra-articular, unstable, with angular or rotational displacement, require surgical treatment, that is, fixation of fragments using pins, screws or plates. If left untreated, fractures of the metacarpal bones and phalanges of the fingers heal incorrectly and can lead to limited function and cosmetic appearance of the hand. Improperly healed intra-articular fractures cause post-traumatic osteoarthritis, which can cause pain and limitation of movement in the damaged joint.
It should be remembered that not all displaced fractures cause dysfunction of the hand or finger. Also, in parallel with an unevenly healed fracture, there may be other problems that are not related to the injury.
A malunited fracture of a finger is a more complex problem than any other malunited fracture. After all, good hand function also depends on joint mobility, sensitivity, skin coverage, blood supply, and gliding of flexor and extensor tendons. Any pathology of these structures may limit the options for surgical reconstruction of the finger.
If a broken finger has healed incorrectly, you must first weigh all the possible risks and benefits of surgical intervention, discuss the goals and possibilities of treatment with a hand surgeon.
How to diagnose?
It is usually not difficult to identify dysfunction of the hand associated with improper healing of a fracture. There are often external signs, such as pathological rotation, a hump on the back of the hand, angular deformation of the finger, and others. To clarify the nature of the bone deformation, an x-ray is usually sufficient. It is very important to photograph each finger separately in a clear frontal and lateral view.
Rotational displacement is assessed when clenching the fingers into a fist: whether there is crossing or not. And here difficulties may arise, for example, we assume that the finger is simply not yet developed and therefore does not bend, but in fact there is a slight rotational displacement, which makes it difficult to bend.
So for a complete diagnosis, both analysis of radiographs and examination by a specialist are important. After all, tendon mobility can only be assessed during examination; ultrasound or MRI are not very helpful in assessing the condition of soft tissues when it comes to fingers.
In the case of intra-articular fractures, a computed tomography scan may be ordered to assess displacement.
Wrist fractures
The bones of the wrist, due to their shape, structure and position, are broken quite rarely. The most susceptible bone to fracture is the scaphoid, the large bone at the base of the big toe. Injuries to the lunate and pisiform bones of the wrist also occur. The triquetral bone, as well as the bones of the distal row - polygonal, trapezoid, capitate and hamate - are subject to fractures extremely rarely; usually their fractures are combined with dislocations in the corresponding joints.
Scaphoid fractures
The cause is a fall on a bent hand, a blow with a fist, or a direct injury to the wrist. The following options are possible:
- intra-articular fracture of the scaphoid - the fracture line is located inside the cavity of the wrist joint;
- extra-articular fracture - separation of the tubercle of the scaphoid;
- de Quervain's fracture-dislocation - a simultaneous fracture of the scaphoid and dislocation of its proximal fragment and the lunate from the wrist joint.
Symptoms are pain and swelling at the base of the thumb, inability to move the hand at the wrist joint, or clench the hand into a fist. The diagnosis is established based on the patient’s complaints, data on the nature of the injury, examination and radiography of the hand bones. Sometimes, in the absence of displacement of fragments, the fracture line with all its signs is not determined. In this case, immobilization is still carried out with repeated radiography after 7-10 days, when, due to the activation of regenerative processes, the fracture line becomes clearly visible.
Treatment is immobilization with a plaster cast for a period of 4 weeks, followed by monitoring and prolongation of immobilization in case of insufficient consolidation of the fracture. In case of displacement of fragments and fracture dislocation, closed reduction is ineffective; fixation of fragments of the scaphoid bone with a wire is indicated. Fractures of the scaphoid are often complicated by the development of a false joint or lysis of bone fragments due to damage to the blood vessels supplying them during injury. Therefore, it is important to follow all the doctor’s recommendations and take control photographs in a timely manner to avoid complications and deterioration in the function of the wrist joint. After restoring the integrity of the scaphoid bone, physiotherapeutic treatment and exercise therapy are indicated to restore hand function.
Lunate fractures
The cause is a fall on a bent hand or direct injury, a blow to the wrist. It manifests itself as pain and swelling, intensifying with movements in the third, fourth and fifth fingers and with extension of the hand. The diagnosis is established taking into account complaints, the mechanism of injury, an objective examination of the area of damage and the results of an x-ray examination. To treat a lunate fracture, a plaster cast is applied for 4-8 weeks. Recovery usually proceeds without complications.
Fractures of the pisiform bone
The cause is a blow with the edge of the palm or direct injury. It manifests itself as pain and swelling of the wrist on the little finger side, increasing pain when it moves. The diagnosis is made taking into account complaints, anamnesis of injury, examination of the area of damage and radiography of the bones of the hand. For complete consolidation of a fracture of the pisiform bone, 4-5 weeks of immobilization are sufficient. The injury is rarely complicated.
Treatment
So what to do if your finger is not fused correctly?
It is worth contacting a specialist in the treatment of hand pathologies. A regular emergency room or traumatology department in a hospital is unlikely to take on the treatment of the consequences of a wrist fracture, and they will be right.
First, it is necessary to find out whether the patient’s complaints are a consequence of malunion or a lack of rehabilitation. Post-traumatic contractures of the hand joints are almost always first treated by a hand therapist using dynamic orthosis and other techniques for non-surgical joint development.
If the bone of the finger on the hand has really fused incorrectly, then the surgeon, together with the patient, decides on the timing and methods of correcting this deformity. Most fractures of the phalanges and metacarpals can be repaired and fixed with pins.
I prefer to perform such operations with local anesthesia because it is safe and convenient. Directly on the operating table, the patient moves the newly fixed fingers, which makes it possible to verify the correction of the deformity and the stability of the fixation. In the postoperative period, this gives confidence to allow early development of movements.
Usually I don't leave the knitting needles sticking out, but rather bite them under the skin. They are removed after 5-6 weeks through small punctures, also under local anesthesia.
While the fracture is healing after surgery, an individual orthosis is made from thermoplastic, which is much lighter and more comfortable than conventional plaster.
Metacarpal fractures
The long, thin metacarpal bones are often broken by a punch or direct trauma. Muscle traction and movements in the hand until the fracture is immobilized often lead to displacement of bone fragments. There are epiphyseal fractures, when the fracture line is localized in the area of the bone heads, and diaphyseal fractures, when the fracture line is located in the bone body.
First metacarpal fracture
The cause is a blow with a bent first finger, less often a direct blow to the first metacarpal bone.
Fracture of the base of the first metacarpal bone . A typical injury for boxers and MMA fighters. A Bennett fracture is a separation of the base of the first metacarpal bone, which is held by ligaments, with simultaneous dislocation of most of it in the carpometacarpal joint. Rolando's fracture is a comminuted fracture-dislocation of the first metacarpal bone. Both injuries present with pain, deformation and swelling in the “anatomical snuffbox” area - the area under the base of the first finger - with increased pain when moving or trying to make a fist. Diagnosis is carried out taking into account complaints, trauma history, examination of the area of injury and x-ray of the hand. Bennett and Rolando fractures are treated surgically using osteosynthesis - restoring bone integrity by fixing fragments with metal knitting needles, pins or plates.
Fracture of the middle part of the first metacarpal bone . More often it occurs due to a direct blow to the bone. It manifests itself as pain, swelling and deformation in the area of the first metacarpal bone. The diagnosis is established taking into account the patient's complaints, information about the mechanism of injury, examination of the area of the first metacarpal bone and x-ray examination of the bones of the hand. Treatment is plaster immobilization for a period of 4-5 weeks; if the fragments are displaced, preliminary closed reposition is required. If conservative reduction is ineffective, an operation - pin osteosynthesis - is performed to compare the fragments.
An example of Dr. Valeev’s operation to restore after a fracture of the first metacarpal bone:
Before surgery:
After operation:
Fracture of II, III, IV, V metacarpal bones
The cause is a blow with a fist or a fall on fingers clenched into a fist. They can be single, but more often several metacarpal bones are broken, usually the fourth and fifth. It manifests itself as pain, swelling and deformation of the hand, and a hematoma often occurs. Diagnosed on the basis of complaints, history of injury, objective examination and X-ray results of the bones of the hand. To treat a non-displaced fracture, immobilization is performed for a period of 4-5 weeks. If fragments are displaced, closed reduction is indicated, and if it is ineffective, skeletal traction or pin osteosynthesis is indicated.
Case study No. 1
A girl whose phalanx of her finger fused incorrectly described her complaints like this:
“If the hand is at rest, there is a pulling sensation in the finger somewhere from the middle of the palm, as if it is heavier than the rest, or as if stiff, this does not bother you, it is just noticeable. When vibrating, shaking a finger, it hurts from slightly to very much, for example, if you touch something with your hand (not hit, but lightly) - get caught on clothes, hand in hand, furniture - it already hurts, I wince, but tolerable. My husband suddenly took my hand - I screamed, there was sharp pain. Holding a weighty object (salad bowl, book) in your hand (4 fingers at the bottom, big at the top) hurts, I immediately grab it with my other hand. I unclench my fist after I bring the bag from the store and have to endure it for a couple of minutes until the pain subsides - although the load seems to be greater on the other fingers, and it didn’t hurt to carry it. At the same time, it hurts to bend and unbend a finger only if you try to do it with effort, further than he can do” (the author’s spelling and punctuation have been preserved).
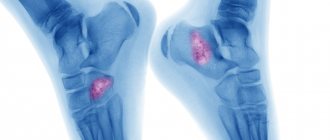
The image clearly shows a displacement along the articular surface of the middle phalanx, which was not eliminated during treatment of the fracture.
In this case, corrective osteotomy is impossible and plastic surgery was performed with an osteochondral graft from the hamate bone (hemi-hamate arthroplasty).
In this operation, a piece of bone with cartilage from the hamate is taken, which is ideal for replacing a defect in the articular surface of the base of the middle phalanx.
This is what the finger looks like after surgery.
Three months later, the girl wrote about him in a completely different way:
“I perform all the actions that I couldn’t do with my hand before the operation because of pain in the finger without any problems, the only slightly painful sensations are when I try to fully bend it and immediately straighten it completely and vice versa, but the pain is not sharp and goes away immediately.
The set of rehabilitation exercises that the doctor showed me at the handclinic began slowly - now I perform it much more actively, the strength in the finger is almost on par with the rest, plus the steering wheel (a good compression trainer), plus briefcases - I use my hand actively, even the muscle of the left forearm is already aligned with the right, otherwise I compared them in August by accident, I was quite surprised at how weak my left arm was in six months after the fracture.
As far as I understand your forecasts, things with the finger are, in principle, as expected.”
Features of the structure of the toes
The toes are based on tubular bones. Each finger is formed by three phalanges, except the thumb, which has only two. Thanks to the movable joints and tendons, the fingers can perform various movements and help a person maintain balance while walking. Even minor damage to the soft and hard tissues of the foot leads to movement restrictions and knocks a person out of the usual rhythm of life.
During a bruise, tissue damage and microtrauma of blood vessels occur. This leads to an increase in edema and the development of an inflammatory reaction. Even a minor injury requires appropriate treatment for a bruised toe. Otherwise, swelling and pain will increase, limiting the patient's physical activity. Often, bruised toes are accompanied by blue discoloration and peeling of the nail plate. In this case, it may require partial or complete removal.
Possible complications
An improperly healed fracture of a finger can lead to unpleasant consequences that will significantly affect the functionality of the hand and the person’s future life.
The most common complications are:
- Vicious union. Leads to limited mobility.
- Osteomyelitis. This is a chronic disease that occurs when an injured area becomes infected. It causes severe pain. It can only be treated with surgery.
- Formation of pseudarthrosis or false joint. In this case, the finger will bend in a place where it should not bend. This happens if the immobilizing bandage was not applied tightly enough or incorrectly. In this case, the fragments are rubbed against each other, and the bone canal is overgrown, leaving a small space between the fragments. This can only be corrected through surgery.
- Formation of a large bone callus. If the fragments were not juxtaposed correctly, a very large bone callus will form at the junction. It not only looks ugly, but also limits the movement of the finger.
- Contractures. Prolonged immobilization can cause the tendons to become shorter, causing the finger to lose some mobility.
- Ankylosis or complete immobility of the joint. This happens if the fracture occurs near a joint. If treated incorrectly, the finger loses some of its functions. There is no cure for this complication.
Read also: Causes and symptoms of synovitis of the knee joint
How to treat bruises and broken toes
Patients with bruises and broken toes require first aid. It is very important to contact a traumatologist in a timely manner and undergo the prescribed examination. This will allow the doctor to select effective treatment for bruised toes as soon as possible and take all necessary measures to prevent complications.
Medical tactics for bruises and fractures of fingers are selected depending on the nature of the injury. With an open fracture, the wound can quickly become infected and fester, and the risk of developing tetanus cannot be ruled out. Experts practice the administration of anti-tetanus serum and antibacterial treatment of open wounds of the toes, especially if they are caused by contact with the ground and working tools.
Immobilization is indicated for almost all toe injuries. It allows you to relieve the sore foot and speed up the patient’s recovery process. Treatment of a fractured finger with bone displacement requires special professionalism when it is necessary to restore the anatomical shape of the phalanx. In this case, the correct fusion of bone tissue in the future depends on the professionalism of the traumatologist.
Even a minor finger injury is accompanied by pain and signs of an inflammatory reaction. To relieve pain, specialists prescribe analgesics in the form of local agents, tablets or injections. Drugs are selected taking into account the severity of the patient's condition.
Local agents with anti-inflammatory, regenerating and analgesic properties are recommended for long-term use. They alleviate the patient’s condition, have an antiseptic effect and promote rapid resorption of hematomas.
Fractured toe: types
A toe fracture can be an open fracture, where soft tissue damage occurs and bone fragments may protrude from the wound. In this situation, there is a direct threat of secondary infection. The patient urgently needs antiseptic treatment. For open fractures of the toes, treatment should not be delayed.
With closed fractures of the fingers, the integrity of the skin is not broken, and displacement of the fragments is usually not observed. But this type of fracture does not exclude the development of infectious and other complications. A closed fracture of the toe is often complicated by a purulent infection, especially when the nail bed is damaged and the nail plate peels off, which becomes an entry point for infectious pathogens.
When a displaced fracture occurs, comparison of bone fragments is required, which will give the finger an anatomically correct shape and restore the impaired functions of the limb.
First aid
A fracture of the little finger on the hand requires professional treatment. If a person experiences symptoms consistent with a broken finger, first aid should be provided.
What you should do:
- calm the person down and give him an analgesic (for example, analgin, ibufen, etc.),
- call an ambulance or a taxi,
- if there is an open wound, carefully treat it with an antiseptic and carefully apply a bandage,
- if heavy bleeding occurs, you should use a tourniquet, remembering exactly the time of application,
- immobilization of the upper limb: apply a bandage using branches, sticks or other available means. The hand should be fixed in the position in which the patient feels the least pain. The splint should rest on the finger at one end, extending 2-3 cm above it, and on the palm at the other. You need to bandage from palm to finger. If it is not possible to apply a splint, bandage the injured finger to the adjacent one,
- Apply ice from time to time
- It is better to keep your hand suspended on a scarf over your shoulder.
Read also: Treatment of a clavicle fracture
Remember that the victim may have a complex comminuted fracture, so all actions should be as careful as possible so as not to aggravate the situation.
Signs of a bruised or broken toe
The symptoms of a bruise and a broken toe are similar: the patient feels pain that does not allow him to step on the foot, and also notices swelling of the soft tissues. Only a qualified specialist can distinguish a fracture or crack from a bruise. An accurate diagnosis is made based on X-ray data and professional examination.
A patient who has suffered a bruised toe should be alert to the following signs:
- pathological mobility of the toes at the site of injury;
- prolonged pain syndrome, which is poorly relieved by classical analgesics;
- increasing swelling and cyanosis of the skin;
- crunching sound (crepitus) when pressing on the injury site;
- unnatural position of the foot or toes.
If such symptoms appear, it is necessary to make an appointment with a traumatologist and conduct an X-ray examination to make sure that there is no fracture of the toe. Do not self-medicate under any circumstances, even if you are sure that the injury you received is harmless. Our Clinic also employs pediatric traumatologists, and you can show your child to a specialist at any time or seek medical help from an experienced doctor yourself.
With a marginal fracture of the big toe, which often occurs while running, the swelling spreads to the entire foot, and the skin becomes noticeably blue. The patient experiences severe pain and cannot step on his leg; he often takes a forced position, which allows him to spare the limb as much as possible. Signs of a big toe fracture can be supplemented by pathological mobility and the presence of crepitus.