Genital herpes is a viral disease characterized by a rapid transition to a chronic form and frequent relapses. The degree of infection is high, more than 90% of the world's population is infected with herpes simplex virus (HSV) types 1 and 2. Only 20% of them have clinical manifestations. Among STDs, herpes is second only to gonorrhea and spreptococcal urethritis, and among viral infections - only to influenza.
The pathology is transmitted predominantly sexually and affects the skin and mucous membranes: watery, painful papules - blisters - appear on them. Their usual localization in men is in the urethra, folds of the foreskin and on the head of the penis. Accordingly, the formations interfere with normal urination and intimate life, causing pain and other unpleasant symptoms.
Herpes in men is complicated because, due to the specific structure and structure of the urinary and reproductive systems, it is impossible to quickly prevent the development of pathology. Scientists have found a connection between the spread of HSV-2 and prostate cancer.
Pathogenesis
Genital herpes is defined in ICD-10 under code A60.0. According to WHO, men are infected 2 times less often than women. When infected, the virus primarily attacks epithelial cells, affecting large areas of the genitals, passing further into the genitourinary system.
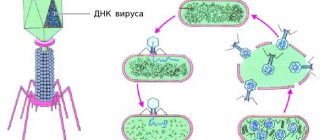
In cells, viruses reproduce by budding; already 10 hours after infection, herpes is ready to create “daughter” virions - full-fledged viral particles. They penetrate various tissues, blood, lymph. The period of subsidence of the virus depends on the level of immunity. Usually it is 14-21 days.
Acellular organisms infect nerve ganglia (clusters, nodes), remaining there for life, since they cannot survive without a cell. Here they do not manifest themselves in any way until so-called trigger situations occur, which serve as an impetus for the activation of pathogenic microflora.
MAKE AN APPOINTMENT WITH A UROLOGIST
Klokov Andrey Nikolaevich
Urologist-andrologist, doctor of the highest category
Make an appointment
Herpetic infection of the genitourinary system in men
N
The uncontrolled widespread increase in the incidence of genital herpes (GG) puts the problem of herpesvirus infection (GI) on a par with the most pressing socially significant health problems. The incidence of HS in Western European countries exceeds 80 cases per 100 thousand population. Currently, according to B. Halioua et al. (1999), there are 86 million people in the world infected with herpes simplex virus type 2 (HSV-II), traditionally associated with HH, although it has been proven that HH can also be caused by HSV type 1.
Our analysis of official statistics data showed that the incidence of HS in Russia for 1993–1999. increased from 8.5 to 16.3 cases per 100 thousand population, and in Moscow - from 11.0 to 74.8. The bulk of patients in Russia turn to doctors on their own: 70-94% of registered patients. The share of active identification of patients with HH by first-level health care providers during all types of preventive examinations in Russia was 22.7-27.8%, in Moscow - 5.4-7.2%. At the same time, obstetricians and gynecologists identify 45.1–54.8%, dermatovenerologists – 39.8–43.8% of the total number of actively identified patients with HS, and urologists account for no more than 5–12%.
While close attention is paid to the study of herpes of the external genitalia and the adverse effects of GI on the reproductive function of women, information about HSV as an etiological factor in diseases of the genitourinary system (GUS) in men is very limited. It should be said that assessing the true role of HSV in the development of pathology of the MPS organs in men, taking into account the frequent mild or asymptomatic course of the infection, often turns out to be a very difficult task.
Herpes is called “many-faced” and “insidious”, meaning the variety of manifestations of the disease and accompanying symptoms due to the peculiarities of the pathogenesis of GI. The main links of pathogenesis
herpes infections are:
1. Infection of the sensory ganglia of the autonomic nervous system and lifelong persistence of HSV in them.
2. Damage to immunocompetent cells, which leads to secondary immunodeficiency, creating conditions for relapse of the disease.
3. HSV tropism for epithelial and nerve cells, causing polymorphism in the clinical manifestations of herpetic infection.
Infection of the genitals occurs through close physical contact with a patient or a virus carrier during genital, oro-genital, genitorectal and oral-anal contact. Only 10% of infected people develop clinical symptoms of primary HH.
The virus begins to multiply at the site of inoculation, where typical blistering rashes appear, and penetrates the bloodstream and lymphatic system. At the early stages of HI, viral particles also penetrate into the nerve endings of the skin or mucous membrane, move centripetally through the axoplasm, reach the peripheral, then segmental and regional sensory ganglia of the central nervous system, where they remain in a latent state in nerve cells for life.
Infection of sensory ganglia is one of the important stages in the pathogenesis of HI. With herpes, the genitals are the sensitive ganglia of the lumbosacral spine, which serve as a reservoir of the virus for its sexual transmission. The spread of HSV in a centrifugal direction during a relapse determines the anatomical fixation of lesions during relapses.
HSV can affect any nerve formations, which will clinically manifest as various neurological symptoms depending on the properties of the nerve formations involved in the infectious process. When sympathetic nodes and peripheral nerves are affected, patients experience symptoms of ganglioneuritis; combined damage to the ganglia and segmental roots of the spinal cord causes clinical manifestations of ganglioradiculoneuritis. Irritation of parasympathetic fibers causes subjective sensations in patients in the form of a burning sensation. The peculiarity of the pain syndrome with recurrent herpes (HR) is that it can periodically occur regardless of skin manifestations, which greatly complicates its interpretation. Neurological symptoms, complicating the course of the disease and worsening the prognosis, occur in every 3rd patient suffering from recurrent genital herpes (RGH).
The literature describes cases of acute urinary retention, the cause of which was sacral myeloradiculitis (Elsberg syndrome), meningitis and radiculomyelopathy, the cause of which was HSV.
In 25% of patients with RGG, increased trauma, dryness and the formation of small painful bleeding cracks on the mucous membranes of the external genitalia due to mechanical irritation appear.
Clinical manifestations of GG in men
Herpes of the external genitalia
In most cases, primary infection of the genitals is asymptomatic, with the subsequent formation of latent carriage of HSV or a recurrent form of genital herpes. In clinically significant cases, primary genital herpes usually manifests itself after 1–10 days of the incubation period and differs from subsequent relapses by a more severe and prolonged (up to 3 weeks) course (Fig. 1).
The likelihood of developing a recurrent form of HH depends on the serological type of HSV: when the genitals are infected with HSV type 1, a relapse within a year occurs in 25% of people who had a primary episode of HH; in HH caused by HSV type 2, relapses occur in 89%.
Clinically, herpes of the external genitalia can occur in typical, atypical and subclinical (asymptomatic) forms.
In men, rashes are usually located in the area of the outer and inner layers of the foreskin, coronary sulcus, and scaphoid fossa. Less commonly, the head and body of the penis and the skin of the scrotum are affected.
Typical form of RGG
characterized by the classic dynamics of lesions (erythema - vesicles - erosive-ulcerative elements - formation of crusts) and local subjective sensations in the form of itching, burning, pain. The lesions are usually limited, less common and localized in the same area of the skin or mucous membrane. Frequent exacerbations of RGG are often accompanied by a deterioration in the general condition of patients, symptoms of intoxication due to viremia appear (headache, chills, malaise, low-grade fever), and the inguinal lymph nodes may enlarge and become painful.
Atypical forms of RGG
, which significantly complicate the diagnosis, may be due to: 1) a change in the development cycle of herpetic elements in the lesion; 2) unusual localization of the lesion and anatomical features of the underlying tissues.
In atypical forms of RGG, one of the stages of development of the inflammatory process in the lesion (erythema, blistering) or one of the components of inflammation (edema, hemorrhage, necrosis) predominates. According to the intensity of clinical manifestations, atypical forms can occur rapidly with manifestation (bullous, ulcerative-necrotic) or subclinically (microcracks), see Fig. 2-4.
Subclinical form of RGG
is detected mainly during virological examination of sexual partners of patients with any sexually transmitted disease, or during examination of married couples with impaired fertility.
Herpetic infection of the pelvic organs
A feature of GG is its multifocality. The pathological process often involves the lower part of the urethra, the mucous membrane of the anus and rectum, which can occur secondary to the occurrence of herpes of the external genitalia, or can occur as an isolated lesion.
According to the characteristics of clinical manifestations, it is advisable to divide herpetic lesions of the pelvic organs in men into:
• herpes of the lower part of the urogenital tract, anal area and rectal ampulla;
• herpes of the upper genital tract (Table 1).
Herpes of the lower part of the urogenital tract, anal area and ampulla of the rectum
manifests itself in two clinical forms:
focal
, characterized by the appearance of vesicular-erosive elements typical of herpes simplex mucous membranes, and
diffuse
, in which the pathological process proceeds as a nonspecific inflammation.
Herpes urethra
The generally accepted classification of urethritis distinguishes between viral urethritis caused by HSV and human papillomavirus (HPV). HSV is more often the cause of prolonged torpid urethritis and recurrent cystitis, as well as exacerbation of chronic prostatitis. The frequency of herpetic urethritis (HU) ranges from 0.3 to 2.9% of all registered non-gonococcal urethritis (Ilyin I.I., 1977; Nahmias A. et al., 1976), which allowed researchers in the 70s to classify HU as rare forms of urethritis. Work in recent years has shown that GU is detected in 42.4–46.6% of cases in men suffering from RGG (Baluyants E.R., 1991; Semenova T.B., 2000).
Subjectively, GU is manifested by pain in the form of burning, sensations of heat, hyperesthesia along the urethra at rest and during urination, and pain at the beginning of urination. The incubation period for the development of HU remains unclear, but is probably several months, less often weeks or days. During a clinical examination, hyperemia and swelling of the urethral sponges are determined, and scanty mucous discharge from the external opening of the urethra periodically appears. The course of HU is subacute or sluggish with periodic remissions and relapses. In the urethral discharge, epithelial cells and mucus usually predominate, and leukocytosis periodically appears. With a mixed infection, urethral discharge becomes more abundant and opaque. With a two-glass sample, the urine in the first portion is transparent, but contains inflammatory products in the form of floating threads and flakes.
The diagnosis of GU is made based on the isolation of HSV from material taken from urethral discharge in cell culture or detection of the HSV antigen by PCR.
The organs of the MPS in men are in a close anatomical and physiological relationship, which does not allow a mechanistic approach to assessing the results of laboratory research. Thus, detection of HSV in urine or urethral discharge allows us to suspect the possibility of involvement of the prostate gland in the infectious process, even if HSV is not detected in prostate juice, but there is clinical evidence of torpid prostatitis.
For dry urethroscopy
on the mucous membrane of the urethra there is usually a soft infiltrate (less often transitional) with fragments of red mucosa, with pronounced large folds and disappearing small ones. Herpetic lesions are represented by small single or merging erosions with polycyclic edges against the background of local vasodilation (focal form of GI), or severe focal hyperemia of the mucous membrane (diffuse form of GI). More often, the anterior and middle third of the urethra are involved in the process. Contraindications to urethroscopy are exacerbation of urethritis and the presence of herpetic eruptions in the glans, scaphoid fossa and inner layer of the foreskin of the penis. Urethroscopy is recommended when external manifestations of herpes have subsided, complaints from the urethra persist, the patient has chronic recurrent urethritis of unknown etiology, and other urogenital infections have been previously excluded.
Bladder herpes
The leading symptoms of herpetic cystitis are the appearance of pain at the end of urination, dysuric phenomena; hematuria is its characteristic manifestation. Patients have a urinary disorder: the frequency, nature of the stream, and the amount of urine change. Herpetic cystitis in men is usually secondary and develops as a complication during exacerbation of chronic herpetic urethritis or prostatitis. During cystoscopy, catarrhal inflammation and isolated erosions are observed.
Herpes of the anal area and rectum
Herpetic lesions of the anal area and rectal ampulla occur in both heterosexual men and homosexuals. The anal area can be affected primarily or secondarily (if the infection spreads in a patient with GI of the external genitalia). The lesion is usually a recurrent crack, which is often a reason for diagnostic errors. Such patients with an erroneous diagnosis of “anal fissure” end up with surgeons.
When the sphincter and mucous membrane of the rectal ampulla are damaged (herpetic proctitis)
patients are bothered by itching, burning sensation and pain in the affected area, small erosions occur in the form of superficial cracks with a fixed localization, bleeding during defecation. The appearance of rashes may be accompanied by sharp bursting pain in the sigmoid region, flatulence and tenesmus, which are symptoms of irritation of the pelvic nerve plexus. Rectoscopy reveals catarrhal inflammation and sometimes erosion. A diagnosis of herpetic proctitis can only be made based on the results of a virological examination of the patient.
Herpes of the upper genital tract
manifested by symptoms of nonspecific inflammation.
Typical
The clinical picture of herpetic lesions of the organs of the upper genitourinary tract is manifested by symptoms of nonspecific inflammation. It is very difficult to establish the real incidence of damage to the internal genital organs in men, since in 40–60% of cases the disease occurs without subjective sensations.
In subclinical form
herpes of the internal genitalia, the patient has no complaints; Clinical examination does not reveal symptoms of inflammation. A dynamic laboratory study of smears of urethral discharge in the prostate secretion periodically reveals an increased number of leukocytes (up to 30–40 or more in the field of view), indicating the presence of an inflammatory process.
Asymptomatic form
Herpes of the internal genitalia (asymptomatic viral shedding) is characterized by the absence of any complaints and objective clinical symptoms of inflammation in patients. During a laboratory examination of the discharge of the urogenital tract, HSV is isolated, while in smears there are no signs of inflammation (leukocytosis).
Prostate herpes
In the modern etiopathogenetic classification of prostatitis, viral prostatitis is regarded as infectious canalicular complications of viral urethritis. According to the classification of Mears (1992) this type of prostatitis is classified as a doubtful or unproven type, according to Blumensaat (1961) - to a specific type, according to O.L. Tiktinsky and V.V. Mikhailechenko (1999) – to infectious.
In the development of viral prostatitis, the urethrogenic route of transmission is most often observed, and the descending (urogenic) route is rare - when viruses penetrate from infected urine during cystitis through the excretory ducts of the prostate gland (PG).
According to various authors, prostatitis is caused or maintained by HSV in 2.9–21.8% of cases (Weidner et al., 1981). Most often, chronic prostatitis with herpetic urethritis and RGG manifests itself in a catarrhal form, while the course of the disease is characterized by a frequent and persistently recurrent nature (O.B. Kapralov, 1988; Bennett et al., 1993).
In clinical practice, the diagnosis of chronic herpetic prostatitis is rarely made by urologists. The reason, apparently, is that virological diagnostic methods are not included in the standard examination of patients with chronic prostatitis. The doctor’s stereotype of thinking comes into play, and patients are traditionally screened for non-viral STDs. Meanwhile, with erased abacterial prostatitis, it can be assumed that the pathogenic agent is a virus.
In the clinical course of prostatitis, functional changes are noted - reproductive changes, pain (with irradiation to the external genitalia, perineum, lower back) and dysuric syndromes. In most cases, exacerbation of chronic prostatitis is preceded by the appearance of herpetic eruptions in the genital area. The appearance of vesicular-erosive elements may coincide with the appearance of complaints from the pancreas. Often in patients with RGG, prostatitis occurs subclinically: in these patients, the diagnosis of prostatitis is made based on the appearance of leukocytosis in the prostate secretion and a decrease in the number of lecithin grains.
It must be remembered that herpetic prostatitis can exist as an isolated form of GI. In this case, there are no symptoms of RGG and HSV is not detected in the urethral discharge. The etiological diagnosis is based on the detection of HSV in the secretion of the pancreas, while there is no pathogenic flora in the secretion and in the third portion of urine.
Ultrasound examination of the prostate gland in the area of the paraurethral zones of the prostate reveals hyperechoic fibrous foci measuring 3–9 mm. In patients with herpetic prostatitis, compared with abacterial prostatitis of unknown etiology, there is a greater severity of fibrous sections in the peripheral zones. Along with this, there is an expansion of the seminal vesicles, indicating a violation of their drainage into the posterior urethra, which suggests damage to the prostatic uterus.
The variety of clinical manifestations of herpes simplex, the presence of atypical, subclinical and asymptomatic forms of the disease, the involvement of many body systems in the infectious process often complicate the diagnosis of this disease.
Diagnosis of herpes
The diagnosis of recurrent genital herpes with typical clinical manifestations of the disease does not present any difficulties and can be made visually when examining the patient. Significant difficulties arise with atypical forms of HH or with herpetic lesions of the OMT. A carefully collected anamnesis is important in these cases. Complaints of itching, burning, scanty mucous discharge from the urethra, sanguineous discharge from the rectum, indications of pain, the recurrent nature of the OMT disease, as well as the resistance of the disease to previous antibiotic therapy. In addition, patients often note a tendency to colds, fear of drafts, periodic general weakness, malaise, low-grade fever, and depression. Patients with HH often experience pain, which patients do not always associate with exacerbations of herpes. Recurrent herpes, regardless of the location of manifestation of the pathological process, is characterized by a wave-like course, when painful states are replaced by periods of well-being, even without specific therapy.
The diagnosis of HSV infection is complicated by the fact that HSV is often in association with other microorganisms: chlamydia, strepto- and staphylococci, fungal flora, etc. A mixed infection of HSV with gonococcus, treponema pallidum, HIV cannot be ruled out, which indicates the need for careful patient examinations.
Existing methods for laboratory diagnosis of herpes simplex are fundamentally divided into two groups:
1) isolation and identification of HSV in cell culture or detection of the pathogen antigen from infected material through cytological, immunofluorescent studies, enzyme-linked immunosorbent assay (ELISA), PCR;
2) detection of virus-specific antibodies in blood serum.
The frequency of HSV isolation from different biological environments varies. When examining more than 200 patients with an established diagnosis of RH, suffering from chronic diseases of the urinary tract, HSV was isolated from urethral discharge in 22% of cases, prostate juice - 23%, sperm - 15%, urine - 26%. HSV may not be detected in everyone, but in 1–2 out of 3–4 biological materials obtained from the patient. Therefore, to reduce the likelihood of a false negative diagnosis, it is necessary to examine the maximum number of samples from one patient. A negative result of a single virological test cannot completely exclude the diagnosis of genital herpes. If an HSV infection is suspected, it is necessary to conduct a repeated virological examination of the discharge of the genitourinary system (once every 7 days, 2–4 times a month), and in some cases, use several examination methods.
The detection of IgM and/or a fourfold increase in the titers of specific immunoglobulins G (IgG) in paired blood sera obtained from the patient with an interval of 10–12 days is of diagnostic importance in primary HI. Recurrent herpes usually occurs against the background of high IgG levels, indicating constant antigenic stimulation of the patient's body. The appearance of IgM in a patient suffering from RGG indicates an exacerbation of the disease.
Treatment of genital herpes
General principles of treatment of herpes simplex
Modern medicine does not have treatment methods that can eliminate HSV from the body. Therefore, the goal of treatment is to suppress the reproduction of HSV during an exacerbation, the formation of an adequate immune response and its long-term preservation in order to block the reactivation of HSV in areas of persistence.
Currently, there are two main directions in the treatment of herpes simplex:
1. Antiviral therapy
, the main place in which is given to acyclovir (ACV) drugs, which are used to stop relapses of herpes, prevent and treat complications of HSV infection.
2. Complex treatment method
, which aims to increase inter-relapse periods, includes immunotherapy (specific and non-specific) in combination with antiviral treatment.
Correction of disorders of nonspecific and specific immunity is one of the main directions in the complex therapy of herpes simplex.
Synthetic interferon inducers (IFN) have a pronounced immunomodulatory effect in the treatment and prevention of complications of herpes simplex. Among them is the domestic drug Poludan
.
To date, convincing clinical data have been obtained on the high effectiveness of Poludan for the treatment of various clinical forms of recurrent herpes. Poludan has a general immunostimulating effect, which makes it possible to use it in secondary immunodeficiency conditions caused not only by herpesvirus infections. In these cases, poludanum is injected subcutaneously into the forearm: 200 mcg (1 bottle) is dissolved ex tempore in 1 ml of distilled water, administered daily, for a course of 10 injections.
One of the advantages of the IFN inducer tilorone
(Amiksin)
is the oral route of administration, which allows patients to independently carry out preventive courses of anti-relapse therapy recommended by their doctor. The mechanism of action of Amiksin includes: induction of interferons of types a, b, g, immunocorrection and direct antiviral effect. Amiksin has a mild immunomodulatory effect, stimulates bone marrow stem cells, enhances antibody formation, and reduces the degree of immunosuppression.
Amiksin is included in the complex treatment of RGG according to the following regimen: 250 mg once a day for 2 days, then 125 mg every other day for 3–4 weeks. According to the same scheme, Amiksin can be recommended to patients between courses of vaccine therapy to prolong the achieved effect.
Antiviral activity of the IFN inducer – Arbidol
due to its immunomodulatory and antioxidant properties. Arbidol can be included in the complex treatment of RH (0.2 g 2 times a day with meals for 10–14 days) and used between courses of vaccine therapy to prevent relapses of herpes (0.2 g 1 time a day with meals for 2–3 weeks).
To stimulate the T- and B-links of cellular immunity in patients with recurrent herpes, Taktivin, Timalin, Timogen, Myelopid and other immunomodulators can be used.
Specific immunotherapy consists of the use of domestic herpetic vaccine
(polyvalent, tissue, killed). The therapeutic effect of the vaccine is associated with the stimulation of specific reactions of antiviral immunity, restoration of the functional activity of immunocompetent cells and specific desensitization of the body.
Taking into account the peculiarities of the pathogenesis of herpes simplex, the most appropriate way to achieve a therapeutic effect is the combined use of drugs with different mechanisms of antiviral action, which prevents the emergence of resistant strains of HSV. The use of interferons and their inducers in combination with a herpetic vaccine and immunomodulators allows for a comprehensive solution to the treatment of herpes simplex.
Local treatment of GI organs of MPS in men
Achieving a therapeutic effect in the treatment of herpetic lesions of the MPS organs in men is impossible without local treatment
.
If there are rashes on the skin and mucous membranes during RHG, patients are prescribed local antiviral drugs for external use: Zovirax (cream), Acyclovir-acri (ointment), Gevisosh (ointment), Viru-merz (gel), Epigen (aerosol), etc. P.
Local immunostimulating therapy is important in the treatment of HS. For this purpose, you can use Poludan
. Poludan for RGG is used in the form of applications to the lesion, for which 200 mcg of the drug (1 bottle) is dissolved in 4 ml of water, moistened with a cotton swab and applied to the lesion for 5–7 minutes. The procedure is repeated 2-3 times a day for 2-4 days.
In the treatment of herpetic urethritis, Poludan is used as instillation into the urethra (400 mcg diluted in 10 ml of water). The procedure is repeated once a day, every day for 5–7 days. You can use cycloferon liniment (according to the same scheme).
For herpetic proctitis, a pronounced therapeutic effect is observed when patients are prescribed Poludan solution in the form of microenemas (400 mcg diluted in 10 ml of water, 10 microenemas per course of treatment).
Along with local medicinal treatment, patients with chronic herpetic diseases undergo OMT traditional local manipulations: bougienage of the urethra, massage of the prostate, followed by total instillation of Poludan solution or cycloferon liniment. To achieve a more pronounced anti-inflammatory, absorbable and analgesic effect in such patients, it is advisable to include low-frequency laser therapy in the course of treatment. In this case, it is advisable to combine the intracavitary introduction of a fiber light guide into the urethra or rectum into the area of projection of the pancreas with laser reflexology.
Complex treatment of men suffering from herpes MPS, including general antiviral and immunostimulating therapy in combination with local treatment, leads to regression of clinical signs of chronic urethritis and prostatitis (reduction or resolution of pain and dysuria syndromes), normalization of laboratory parameters, persistent positive dynamics of the course of RGG in 85 –90% of cases.
Conclusion
Among viral diseases, herpes infection occupies one of the leading places, which is determined by the widespread distribution of HSV, 90% of its infection of the human population, the lifelong persistence of the virus in the body, the polymorphism of the clinical manifestations of herpes, and its resistance to existing treatment methods.
Currently, the pathogenic effect of HSV on the development of chronic genitourinary diseases in women, the course of pregnancy and childbirth, and the health of the fetus and newborn is not in doubt.
The role of HSV in the development of pathological processes in the male body is clearly underestimated. At the same time, according to domestic and foreign researchers, in men suffering from chronic inflammatory diseases of the pelvic organs, it is possible to detect HSV in the discharge of the genitourinary system in 50–60% of cases. It has been proven that HSV is an agent that disrupts spermatogenesis and has the ability to infect sperm. This is of particular importance for men of reproductive age and opens up new aspects in the interpretation and solution of the problem of infertile marriages. Literature:
1. Barinsky I.F., Shubladze A.K., Kasparov A.A., Grebenyuk V.N. Herpes. Etiology, diagnosis, treatment // M. – 1986. – 272 pp.
2. Borisenko K.K. // Genital herpes. In the book. Unknown epidemic: genital herpes. Pharmagraphics. – 1997. – p. 75–83.
3. Bragina E.E. // Patterns of disturbances in human spermatogenesis in some genetic and infectious diseases. – Author's abstract. diss. ... doctor of biological sciences – M. – 2001. – 54 S.
4. Genital infection caused by the herpes simplex virus (review information).// J. STDs. – 1994. – є 3. – p. 5–8.
5. Semenova T.B. Simple herpes. Clinic, diagnosis, treatment, prevention. // Author's abstract. diss. ... MD – 2000. – M. – 48 S.
Tiloron –
Amiksin (trade name)
(LENS–Pharm)
Causes and risk factors
In some cases, doctors diagnose pathology in newborns. In this case, the virus is transmitted when the fetus passes through the birth canal. However, the most common cause is infection from a sexual partner during intimacy. In this case, risk factors for developing the disease include unprotected sexual intercourse, especially with frequent changes of sexual partners.
After the virus enters the body, antibodies begin to be produced, so after a short but fairly bright period of activation, herpes subsides. It is instantly activated in case of trigger situations:
- Hypothermia;
- Bacterial, fungal and viral infections;
- Traumatization of the genitourinary system;
- Surgery on the penis, testicles, prostate gland;
- Decreased immunity;
- Chronic pathologies of the genitourinary system;
- Autoimmune diseases;
- Hormonal imbalances.
Even due to climate change or lack of vitamins, genital herpes can remind itself.
Therapeutic measures
The key to the problem of genital herpes is the correct approach to treating the disease and preventing its relapses. Regardless of the location of the rash and the frequency of exacerbations, comprehensive treatment is always necessary. The most common mistake is to limit therapy exclusively to local antiviral agents. Local therapy does not cure, but only eliminates skin manifestations of the infection. Since the herpes simplex virus lives inside the body, it needs to be affected from the inside, i.e. systematically.
The modern arsenal of antiherpetic drugs makes it possible to effectively combat not only the exacerbations of genital herpes themselves, but also the complications that can arise from it. Treatment of simple genital herpes is based on general approaches. First of all, therapy should be comprehensive, with the obligatory prescription of antiviral drugs. The basic therapy is combination antiviral therapy, a combination of acyclic nucleosides with interferon. This combination is required due to the fact that acyclic nucleosides (acyclovir, valacyclovir, famciclovir) disrupt the reproduction of the herpes simplex virus, and interferons destroy active forms of infection in the body.
A well-studied interferon for systemic use is the drug Viferon Suppositories. It is a complex of recombinant alpha-2b interferon and antioxidants (vitamins E and C). For faster relief of skin manifestations, Viferon Gel or Viferon Ointment can be prescribed. In case of psychosomatic complications, the patient is recommended to receive specialized help from a psychologist, neurologist and other specialists. Currently, there are individual counseling programs aimed at psychological rehabilitation of patients with herpes simplex.
Reference and information material
Author of the article
Khaldin Alexey Anatolievich
Dermatovenerologist, clinical immunologist, MD, professor
Loading...
Take other surveys
Kinds
Doctors distinguish between primary and secondary types of the disease.
Primary is the one that is diagnosed for the first time. It is characterized by a bright clinical picture and a rapid course.
Secondary is one that is diagnosed more than once; these are relapses of chronic pathology. The frequency of resumption of symptoms depends on the person’s immunity; symptoms are often blurred and short-lived.
Secondary genital herpes is distinguished by the frequency of exacerbations:
- Mild form – no more than 3 relapses in 12 months;
- Moderate – up to 6 exacerbations in 12 months;
- Severe form – more than 6 relapses per year.
Doctors also classify the disease according to the specific symptoms.
Routes of infection
Although the disease is most often classified as a sexually transmitted disease, it can also be contracted through household objects: by sharing utensils, towels and linen, as well as by kissing. The greatest chance of becoming infected with genital herpes is during its exacerbation. In this case, any contact with the patient may be dangerous and even such a means of protection as a condom, alas, may be powerless against the virus.
FACT:
The highest incidence of genital herpes occurs in people aged 20 to 30 years.
Symptoms of genital herpes
The incubation period of the pathology is from 2 to 14 days, then general and local signs appear progressively, then they decline.
Pathology can be suspected based on the following signs:
- The appearance of vesicles - small bubbles with a diameter of no more than 2 mm, formed in groups up to 2.5 cm in diameter;
- Itching, burning, pain in the affected area;
- Unpleasant sensations during sexual intercourse, urination;
- Local and general increase in body temperature;
- Swelling of the genital organ;
- Malaise;
- Nausea;
- Weakness.
The most common manifest form of genital herpes: severe damage by vesicles, after opening they become covered with crusts, regional lymph nodes are enlarged.
Urologists and andrologists also observe the following forms of pathology:
- Atypical . There is a small number of vesicles, but the penis is swollen and there is severe redness. Cracks appear in the mucosa, which regenerate within 5-7 days.
- Hemorrhagic . The main difference is that instead of a clear liquid in the bubbles, there is a dark red liquid in which blood cells are present. The head of the penis and urethra are very swollen and hot to the touch.
- Abortive . Instead of vesicles there is an itchy spot, a papule, which ulcerates within 5-7 days.
- Subclinical . Swelling in the affected area is accompanied by severe itching, but quickly passes.
Since herpes also affects the nerve ganglia, disturbances of the central nervous and autonomic systems are possible: pinching, pain in muscles and joints, and the spine.
Bubbles in the intimate area
Blisters in the intimate area may be a sign of genital herpes. Today, this pathology is one of the most common pathologies of a viral nature. Herpes in the groin is accompanied by blistering rashes on the mucous membranes and skin. The cause of genital herpes can be two types of microorganisms - herpes simplex virus types 1 and 2 (HSV-1 and HSV-2). More than 90% of the world's inhabitants are carriers of HSV. This infection is a fairly common disease.
Diagnosis of herpes
Since the symptoms are similar to other sexually transmitted infections, urologists conduct an examination only to determine the general condition of the genital organs. The doctor listens to the patient’s complaints and determines, if possible, when and under what circumstances the infection occurred. An examination of the partner is required.
Laboratory blood tests are informative methods:
- PCR (polymerase chain reaction);
- DNA hybridization;
- immunofluorescence reaction;
- identification of specific antibodies to herpes.
Additionally, related problems are identified: inflammatory processes, infections, hormonal imbalances. Urine, contents of vesicles, scrapings and mucus of the urethra, and prostate secretions are subject to examination.
To identify the general condition of the organs of the genitourinary system, doctors prescribe ultrasound, radiography and other instrumental types of examination. They help to detect complications of pathology in a timely manner.
Primary characteristics of infection
Approximately 9 out of 10 people in the world are carriers of some form of herpes virus. At the same time, the virus does not always manifest itself externally. The characteristic rashes, clearly shown in the photo above demonstrating genital herpes in men, are observed only against a background of weakened immunity.
Complications
First of all, the herpes virus causes the appearance of small blisters and accompanying symptoms. If proper therapy is not started in time, an inflammatory process develops against the background of pathogenic microflora:
- balanoposthitis - in the tissues of the head and foreskin of the penis;
- urethritis – in the urethra, urethra;
- cystitis - in the bladder;
- prostatitis – in the prostate gland;
- pyelonephritis – in the structural elements of the kidneys.
Each of the diseases poses a threat to the genitourinary system: urination, reproductive function, erectile function. The development of radiculopathy and viral meningitis is possible due to the involvement of nerve nodes in the pathological process.
How does infertility manifest and how is it treated?
As already mentioned, herpes and infertility in men have a direct connection. The problem with conception due to herpesvirus manifests itself in the form of virusospermia. This is one of the types of pathospermia - pathological changes in the ejaculate, in which various deviations from normal indicators are observed.
The herpes simplex virus is a lifelong carrier. Therefore, infertility treatment is aimed only at achieving stable remission, which will allow pregnancy and the birth of a healthy child. For this purpose, men in whom HSV has been detected in the prostate secretion and diagnosed with viral spermia are prescribed antiherpetic drugs. They are taken according to a suppressive regimen, i.e. there are no relapses only during the course of treatment. To achieve normalization of sperm quality, the medicine is taken for at least 2.5-3 months.
Treatment of herpes
It is recommended that both sexual partners undergo therapy. Urologists prescribe antiviral drugs during relapse and during remission: there may be one drug, but the dosage is reduced during the lull period.
Ointments, gels and creams that contain an antiviral component, as well as substances that reduce symptoms: painkillers, decongestants, anti-inflammatory, antipruritic, have proven themselves well.
However, in difficult cases, doctors prescribe intravenous or intramuscular administration of antiviral and immune-supporting drugs. And ointments that relieve symptoms are used additionally.
In difficult situations, doctors add plasmapheresis to the treatment program - the elimination of the viral component from the blood plasma. In a centrifuge, the plasma is separated from the total blood composition, purified, and then administered to the patient.
Herpes: questions and answers
Is it possible to treat teeth with herpes?
Dentists say that it is possible to treat teeth with herpes, but they strongly advise against doing so. If it is possible to postpone the procedure, it is better to postpone it for 1-2 weeks, when the blistering rashes completely disappear. If the toothache is mild or moderate, specialists will help relieve it with safe medications, and the therapy itself will begin after the exacerbation of herpes has passed. In critical cases, if you need urgent surgical intervention, you will be helped in any dental clinic, despite the presence of concomitant diseases.
We recommend monitoring the condition of your teeth and undergoing regular preventive examinations so that in the future there is no reason for urgent dental treatment during the period of herpes. We advise the same regarding viral infections. This pathology is difficult to control. Often its symptoms appear at the most inopportune moment. If you are tired of discomfort on your lips, spoiled appearance and constant itching, contact our medical center and get rid of this problem.
Can you drink alcohol if you have herpes?
In this case, alcohol does not have a negative effect directly on the affected area. However, drinking it during an exacerbation of herpes is still not recommended, since alcohol has a bad effect on the body as a whole. When it is consumed, the body begins to spend energy on eliminating alcohol and turns on compensatory mechanisms, which leads to even greater fatigue and a decrease in protective reactions. Medicine has long recognized that there are no safe doses of alcohol. There are no direct contraindications to drinking alcohol during an exacerbation of herpes, however, specialists at our Private Practice clinic strongly do not recommend this for the following reasons:
- Alcohol can worsen existing allergic reactions or provoke new ones in response to one of the medications you are taking.
- Alcohol increases the load on the liver, which at this moment is already working on the biotransformation of drugs and the removal of infectious toxic products.
- The likelihood of developing side effects with any treatment regimen for alcohol intake increases significantly.
- Alcohol further suppresses the immune system, which complicates the treatment of herpes and delays the moment of recovery.
- Alcoholic drinks retain fluid in the body, which slows down the removal of toxins and cleansing of the bloodstream.
Of course, if there is an important reason, drinking alcohol in small quantities is allowed even while treating herpes. In the absence of abuse, the possible risks are minimal. At the same time, we try to convey to each patient the importance of following the prescribed treatment regimen and the need for dedication, since the patient himself is primarily interested in a successful result.
Thus, our medical doctor takes the position that you can drink alcohol if you have herpes, but you shouldn’t do it. Following a correct lifestyle and a competent treatment regimen drawn up by our specialists guarantee the achievement of the desired and quick result.
Is it possible to wet herpes?
The common belief that herpes cannot be wetted is incorrect. The water itself does not have a negative effect on rashes and damaged skin. It does not increase the symptoms of the disease and does not contribute to its progression. On the contrary, it is recommended to keep the skin affected by blisters clean to prevent secondary infection and speed up healing.
You can wash your face if you have blisters on your lip, and you can also take a shower if you have rashes on your body. In this case, you should follow some precautions:
- during an exacerbation, take a shower rather than a bath;
- the water temperature should be comfortable, and prolonged bathing and the use of hot water should be avoided;
- It is better to simply wash off dirt and sweating with water using the palm of your hand, rather than using a washcloth. During the period of exacerbation, the use of hygiene products that contain added dyes and fragrances is also subject to restrictions;
- After swimming, it is better to pat your skin with a towel rather than dry yourself with it. We recommend using two towels, one of which should be in contact with the affected areas of the skin, and the other with healthy areas.
Is it possible to take baths if you have herpes?
We do not recommend taking baths if you have herpes. To maintain hygiene, it is enough to take a shower every day. Hot baths and prolonged swimming can reduce the skin's protective properties and also contribute to the spread of infection to neighboring areas. The exception is short-term therapeutic baths after the acute stage of the disease with the addition of agents with bactericidal properties.
Is it possible to go to the pool with herpes?
Herpetic blisters periodically burst, and the affected area of skin turns into an open wound. This area should be protected from possible infection and any damaging factors. We do not recommend going to the pool if you have herpes, as the likelihood of skin damage increases. The main reasons are the addition of aggressive disinfectants, as well as prolonged exposure to water. In addition, you must remember that during the period of exacerbation of herpes infection you are very contagious and should not attend open groups.
Is it possible to give birth with herpes?
The birth process is quite complex and is accompanied by rupture of blood vessels and bleeding. Open blood flow significantly increases the likelihood of the baby contracting infections that the mother has. When preparing for the upcoming birth, the question becomes relevant: is it possible to give birth with herpes and what is the best method to do this. According to American studies, herpes during pregnancy is transmitted from mother to child in less than 1% of cases. If a woman had relapses of herpes before pregnancy, then the child is reliably protected from infection by maternal antibodies to the virus. The woman chooses the method of delivery together with the gynecologist, and natural childbirth is also possible.
Is it possible to breastfeed if you have herpes?
Everyone knows that during an exacerbation of herpes, it is better for the patient to protect himself from any contact with others - shaking hands, using common household items, etc. This is due to the fact that the blistering rash contains a high concentration of the virus and there is a high risk of infecting other people. Considering this, the question arises whether it is possible to breastfeed with herpes, because this process involves the closest possible contact between the child and the young mother.
According to American studies, breastfeeding during exacerbation of herpes virus infection is possible. Specialists at our Private Practice clinic recommend not interrupting breastfeeding even if there is a relapse of a viral infection in the mother, since breast milk is the best nutrition for a newborn. In addition, antibodies to the virus enter the child’s body with mother’s milk, thereby providing the baby with stable antiherpetic immunity.
Is it possible to smear herpes with brilliant green?
Zelenka is not an antiviral agent. Its benefits for herpetic rashes include drying the wound, accelerating cell regeneration and preventing bacterial infection. You can smear herpes with brilliant green, but this should be an addition to the main treatment, and not monotherapy. Our Private Practice clinic offers everyone to undergo a detailed diagnosis of virus carriage, as well as receive an individual treatment regimen to reduce the frequency of relapses.
Is it possible to smear hydrogen peroxide on herpes?
Peroxide is an antiseptic that, when it gets into a wound, causes virtually no pain, unlike iodine and brilliant green. Thanks to this, the remedy has become quite popular, including in the fight against herpetic rashes. In their practice of treating herpes, our doctors do not discourage the use of peroxide externally, but we need to clarify why this should be done. Peroxide is used for its intended purpose (as an antiseptic) and is not an antiviral agent. Free oxygen, which is released from the peroxide when interacting with the virus, has a detrimental effect on the cell wall of the pathogen. An additional benefit is the ability to expel dead organisms and cleanse the wound. However, modern medicine, which is followed by highly qualified specialists at our clinic, suggests using antiviral drugs with proven effectiveness instead of peroxide. We will select an individual treatment regimen for each patient and help avoid relapses.
Is it possible to smear herpes with iodine?
We can confidently answer: only two methods are effective in the fight against viral infections. The first is the use of antiviral drugs, the second is an increase in the immune response. Iodine is an antiseptic and acts as an oxidizing agent. The popularity of its use for herpes is explained by its ability to dry out blisters, destroy cells damaged by the virus and prevent secondary infection. The product can be used to accelerate wound healing and cell regeneration. It is possible to cauterize herpes with iodine, but you need to understand that the procedure is not done to kill the virus, but rather is a way to prevent bacterial infection. It is strictly not recommended to use concentrated iodine solutions to cauterize herpes with iodine if rashes appear in the genital area, since these areas of the skin are very sensitive.
Can you treat herpes with toothpaste?
Toothpaste is one of the popular folk remedies for combating herpetic rashes. If you smear toothpaste on herpes, unfortunately, you will not be able to kill the virus. It lives inside the body, and symptoms of the disease appear only when immunity decreases. The secret to the effectiveness of toothpaste is its fluoride content (other toothpastes are not suitable for such purposes). This element destroys the membranes of damaged cells, accelerates tissue renewal and wound healing, which leads to faster disappearance of symptoms and recovery. Our medical center offers a more modern approach to the treatment of herpes viral diseases. If you believe in the power of toothpaste, try to choose products based on herbal ingredients, as they will additionally have an anti-inflammatory and drying effect.
Is it possible to cauterize herpes?
When characteristic rashes appear, many patients try to immediately cauterize the blisters with iodine, brilliant green or alcohol. However, a virus is an infectious agent that penetrates inside a human cell and, thanks to it, continues to live and multiply. It is possible to cauterize herpes, but it is recommended to do this to prevent the development of a secondary infection, and not to destroy the virus. Our Private Practice clinic advises all patients to use non-alcohol-based antiseptic solutions for these purposes to avoid unnecessary injury and burns to the skin.
What happens after infection?
One of the characteristics that distinguishes viruses from the herpes virus family from other types of viruses is latency. HSV and other herpes viruses have the ability to create small but permanent colonies of viral particles inside the body. These colonies are often completely inactive (or dormant), but they remain in the body for life.
As soon as HSV gains a foothold in the body, it begins to create copies of itself and spread. This can lead to a clinical picture of the infection ranging from mild and unnoticed symptoms to severe illness. In response to this, the immune system mobilizes its forces and limits the spread of HSV. Regardless of the severity of symptoms, the virus remains in the body. To avoid the immune system, HSV “retreats” along the nerve fibers and hides in the nerve ganglia. In the case of genital herpes, the virus is located in the sacral plexus of ganglia, located at the base of the spine. In the ganglia, the virus remains inactive (latent) for an indefinite period of time.
The phenomenon of latency is similar to the sleep cycle. Basically, the virus remains dormant in a safe place, sometimes for a very long time. Unfortunately, various biological events can activate HSV, after which the virus spreads along nerve fibers back to the skin. This may cause the symptoms and signs of genital herpes to reappear.
It is difficult to answer the question of how often the virus can be activated. Previously, it was believed that all cases of HSV activation lead to the development of a clinical picture of the disease. Research then revealed that the virus can become active without causing noticeable symptoms or signs—no itching, no pain, no rash. This phenomenon is called "asymptomatic reactivation."
Asymptomatic reactivation refers to the following situations:
- Some herpetic eruptions may appear in places that are difficult or impossible to see.
- Some herpetic lesions can be mistaken for something else, such as an ingrown hair.
- Some manifestations of herpes cannot be seen with the naked eye.
The fact is that when the herpes virus is activated and moves to the surface of the skin or mucous membranes, it is difficult for even a doctor to notice. In addition, even for a person with symptoms and signs of genital herpes, several days pass before the full clinical picture develops, during which he will not be aware of the reactivation of the virus.