Prolactin is a protein hormone that performs many functions in the body: from adaptation to difficult conditions to ensuring the possibility of breastfeeding. Because of the latter property, it is also called the milk hormone. A condition in which prolactin levels are elevated is called hyperprolactinemia. The Nizhny Novgorod clinic "Alpha Health Center" offers to conduct a comprehensive examination of the body to identify the causes of changes in the functioning of the endocrine system. Hyperprolactinemia can be a symptom of various diseases. A consultation with an endocrinologist will help to diagnose them in a timely manner and undergo a course of treatment.
Norm prolactin
The normal level of prolactin in the blood is no more than 15 ng/ml, it is secreted in impulses - on average there can be about fourteen emissions per day. It reaches its maximum levels in the morning (somewhere between 5 and 7 am), and after waking up it begins to decline - within a few hours it becomes minimal. These data may change due to various factors. For example, if a woman is breastfeeding, the level of prolactin in her body increases and becomes higher than the generally accepted norm. Among other things, the secretion of this hormone depends on the levels of others, such as estrogens, thyroid hormones, etc. Even the slightest changes in the production of these hormones leads to a sharp jump in prolactin levels. Psychoemotional and physical stress, uncontrolled or exceeding the required dosage of taking certain medications, surgery, previous injuries, and much more can also increase prolactin levels.
There are two types of designations for the content of prolactin in the blood: nanograms/liter - ng/l and international milli-units/liter - mIU/l. The first method is used most often - ng/l. Norms for prolactin levels:
- in adult women this figure should be - 64 - 395 mIU/l or 1* - 29 ng/l
- in men - 78 - 380 mIU/l or 1* - 18 ng/l
But in women, these readings can vary depending on the phase of the menstrual cycle: during the follicular phase they are 252 - 504 mIU/l, during the periovulatory phase - 361 - 619 mIU/l, and in the luteal phase - 299 - 612 mIU/l.
What is prolactin
Prolactin is a hormone whose expression, along with luteinizing and follicle-stimulating hormones, occurs in the pituitary gland. This is a substance of polypeptide nature, the molecule of which consists of one hundred and ninety-eight amino acids and three disulfide bridges. It is secreted into the blood in small quantities. The hormone is released in a strictly defined daily rhythm, with its maximum amount in the blood occurring during sleep. At this time, its concentration is seven times higher than during the day.
Prolactin, by feedback principle, influences its own expression. It acts on the feedback principle on the cells of the hypothalamus and promotes the release of dopamine from them, which from the gray tuberous and paraventricular nuclei of the hypothalamus enters the pituitary gland and binds to receptors on lactotropic cells. Thus, not only the secretion of prolactin, but also gonadotropes is inhibited. When regulatory mechanisms are disrupted, women experience symptoms of increased hormone levels.
Two groups of factors are involved in the regulation of prolactin levels:
- inhibiting this process: GABA, dopamine, gastrin, somatostatin, gastrin-releasing peptide, as well as histidyl-prolyl-diketopiperazine;
- stimulating hormone production: thyroliberin, bombesin, serotonin and vasointestinal peptide, opiates, as well as luliberin and neurotensin.
Its secretion is enhanced by estrogens and thyroliberin. It also increases under the influence of nerve impulses from the nipples. Prolactin helps prepare the mammary glands for lactation, so its concentration in the blood constantly increases during pregnancy and becomes high in the third trimester. This is physiological hyperprolactinemia. When serum levels of the hormone become high outside of pregnancy, we speak of pathological hyperprolactinemia.
Causes of hyperprolactinemia
There are a number of well-known causes of hyperprolactinemia:
By their nature, the causes of hyperprolactinemia are physiological and pathological.
Physiological are considered:
- Pregnancy and the postpartum period (for mothers who do not breastfeed, lasts about one to seven days)
- Lactation
- Nipple stimulation or irritation
- Having sex, being stressed, eating food.
Pathological causes of hyperprolactinemia:
- The most common is a pituitary adenoma - a small tumor lesion of the pituitary gland.
- Pathological changes in the pituitary stalk and hypothalamus (sarcoidosis, neurosyphilis, cysts, mechanical damage, etc.).
- Various surgical operations using general anesthesia.
- Liver diseases (cirrhosis).
- Renal failure (after a kidney transplant, prolactin levels become normal).
- Thyroid diseases.
- Ovarian diseases - polycystic ovary syndrome (PCOS).
- Taking certain medications.
Many gynecological diseases cause the development of hyperprolactinemia in women. There are many cases in medical practice when an increase in prolactin levels was observed in patients with endometriosis, adnexitis, uterine fibroids, and inflammatory processes. A third of women who have been diagnosed with polycystic ovary syndrome (PCOS) also have a history of functional hyperprolactinemia. This is due to the fact that high levels of estrogen in PCOS stimulate the production of prolactin and its synthesis.
Hyperprolactinemia
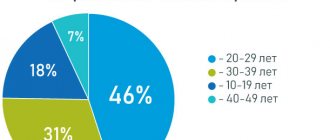
Hyperprolactinemia is increased production of the hormone prolactin in the body. The diagnosis is made on the basis of a clinical blood test. An increase in prolactin levels indicates a disruption in the functioning of parts of the brain caused by stress, physical overload, and various physiological factors. Most often, the pathology is diagnosed in young women, less often in men under the age of 40.
Features of the secretion and function of prolactin
Prolactin is a hormone that supports reproductive function and is responsible for the formation of lactation. The substance is involved in the formation of glandular breast tissue. In men, prolactin is responsible for the synthesis of testosterone and maintains sperm activity.
The role of the hormone in the functioning of other organs:
- adrenal glands – stimulation of the synthesis of active substances that ensure the body’s resistance to increased stress during breastfeeding (aldosterone, epinephrine, androgens);
- pancreas – production of insulin;
- thyroid gland - reducing the secretion of thyrocalcitonitis to increase the mineral content in breast milk;
- immune system - suppression of fetal rejection processes.
The hormone is produced in the pituitary gland. The process is controlled by the hypothalamus. Changes in prolactin levels in women are associated with the menstrual cycle, so hyperprolactinemia in men is diagnosed much less frequently.
Hormone secretion occurs in impulses. In the late follicular phase of the cycle, at least 14 impulses are produced, in the late luteal phase - no more than 9. The level of prolactin also changes during the day. After falling asleep, the concentration of the hormone increases and reaches a maximum after 1.5-2 hours, after which it begins to decrease.
During the menstrual cycle, the amount of prolactin in the blood plasma can range from 5 to 27 ng/ml.
Many factors influence the production of the hormone, so material for analysis is taken at a strictly defined time, not after the procedures.
Causes of pathology
There are many provoking factors.
The main causes of hyperprolactinemia can be identified:
- hypothalamic tumors;
- infectious brain lesions;
- tuberculosis, other pathologies accompanied by granulomatous and infiltrative changes;
- head injuries, hemorrhages;
- empty pituitary sella syndrome;
- pregnancy and the first week of the postpartum period (the main cause of hyperprolactinemia in women);
- emotional stress;
- nipple stimulation, including during breastfeeding;
- chest injuries, such as burns, shingles;
- Cushing's syndrome;
- thyroid diseases;
- disorders of the liver and kidneys;
- taking certain medications, etc.
The cause of hyperprolactinemia in men is often liver cirrhosis. The functional cells of the gland are replaced by connective tissue, as a result of which the rate of removal of prolactin from the body decreases.
Types of hyperprolactinemia
Depending on the cause, there are several forms of the disease.
Physiological hyperprolactinemia
In some cases, this condition is normal:
- During pregnancy. During pregnancy, prolactin levels increase to prepare the female body for lactation. The secretion of the hormone increases from 5-7 weeks of pregnancy. Prolactin levels return to normal after the end of lactation. If a woman does not breastfeed, then the hormonal levels will stabilize within a month;
- During lactation. Prolactin stimulates and controls milk production. When a baby suckles, the hypothalamus receives a signal to synthesize liberins, which, in turn, causes the pituitary gland to increase the secretion of the hormone. Hyperprolactinemia during lactation also suppresses ovulation and reduces the risk of new pregnancy during breastfeeding;
- During sleep. Hyperprolactinemia is observed 1-2 hours after falling asleep;
- During times of stress. A number of patients with fainting and hypotension have increased prolactin;
- During sexual intercourse. The likelihood of orgasm directly depends on the amount of prolactin in the blood;
- During the neonatal period. Hyperprolactinemia is typical for infants in the first week of life.
Pathological hyperprolactinemia
The causes of the pathology are dysfunction of the hypothalamic-pituitary system. The two parts of the brain responsible for the synthesis of prolactin lose communication with each other. As a result, secretion increases many times over.
Anatomical hyperprolactinemia
The disease most often develops against the background of the growth of a pituitary tumor - prolactinoma. Hyperprolactinemia is also caused by hormonally inactive brain tumors, for example, metastases, syphilis, tuberculosis and others. One of the causes of anatomical pathology is head trauma.
Functional hyperprolactinemia
Possible reasons:
- diseases of the endocrine system: adrenal glands, ovaries, thyroid gland;
- times kidney or lung;
- chronic renal failure, prostatitis;
- menopause
Pharmacological hyperprolactinemia
Prolactin levels increase from taking medications that inhibit the production of dopamine, a neurotransmitter that affects the function of the pituitary gland. For example, some neuroleptics, oral contraceptives, antiemetics and sedatives, antihistamines, and amphetamines have this effect.
Idiopathic hyperprolactinemia
A condition of unknown etiology. Examination of the patient shows an increase in prolactin levels, but the cause cannot be determined. In the case of idiopathic hyperprolactinemia, the doctor consistently excludes all possible factors affecting the functioning of the pituitary gland and hypothalamus, and conducts thorough studies to detect tumors at an early stage of development.
Symptoms of hyperprolactinemia
The main symptom of hyperprolactinemia in women is menstrual irregularity. The hormone actively affects the function of the ovaries, pituitary gland and hypothalamus. Almost every third patient with hyperprolactinemia is diagnosed with a pituitary adenoma at various stages of development. One of the symptoms of the disease is decreased libido.
Other signs of hyperprolactinemia in women:
- excessive male pattern hair growth;
- acne, skin problems;
- rapid weight gain;
- osteoporosis;
- galactorrhea;
- frigidity, hypolipidemia.
In men, increased levels of prolactin cause pathologies of the genital organs and functions, gynecomastia. There is a decline in sexual desire, and the size of the prostate changes.
The doctor may notice the first signs of hyperprolactinemia during a routine examination of the patient. The most characteristic symptom is the release of milk from the mammary glands when pressure is applied in the absence of lactation (galactorrhea).
Diagnosis of hyperprolactinemia
A blood test can determine elevated levels of prolactin. The material is collected on a certain day of the menstrual cycle on an empty stomach. The study is repeated several times to exclude physiological factors for increasing prolactin levels. The normal level of the hormone in a woman’s blood is no more than 27 ng/ml, and a man’s is no more than 20 ng/ml (the numbers are approximate and may differ in different laboratories).
Additional diagnostics are aimed at establishing the causes and associated pathologies:
- consultation with a gynecologist or andrologist;
- Ultrasound of the mammary glands and pelvic organs;
- blood test for thyroid hormones;
- blood sugar test;
- consultation with an ophthalmologist to assess visual fields;
- computed tomography or magnetic resonance imaging of the head with a focus on the sella turcica.
During the appointment, the patient must inform the doctor about all medications that he is taking long-term or permanently. The information will help you adjust your examination plan and further treatment.
Treatment of hyperprolactinemia
Treatment of hyperprolactinemia in women is aimed at reducing hormone levels and restoring regular menstruation. It is necessary to suppress the production of prolactin to normal levels. The dosage of medications is calculated by the doctor depending on the severity of the symptoms of hyperprolactinemia, the gender and age of the patient, and his general condition. At the same time, medications are prescribed to treat concomitant pathologies. If hyperprolactinemia is caused by thyroid dysfunction, a thorough diagnosis is carried out and appropriate therapy is planned.
Treatment tactics depend on the cause and manifestation of the pathology:
- Drug-induced hyperprolactinemia resolves when the medication is stopped. If the patient cannot completely do without medications, it is necessary to select an alternative or ask for the opinion of a medical council to assess the risks;
- Hyperprolactinemia with hypogonadism and osteoporosis is successfully treated with hormonal medications. Depending on the test results, the patient is prescribed drugs based on testosterone or estrogen;
- Treatment of hyperprolactinemia of tumor origin is aimed at reducing the size of the tumor and normalizing hormonal balance. It is important to prevent recurrence of adenoma. In some cases, the dosage of dopamine agonists is selected for the patient. If there is no improvement while taking medications, or if the adenoma enlarges, surgical treatment is indicated. The tumor is removed. The use of radiation therapy and chemotherapy is not indicated.
Dopamine agonist drugs:
- Cabergoline. The advantage of the drug is its prolonged action - you can take the medicine once every few days;
- Bromocriptine. One of the first drugs for the treatment of hyperprolactinemia. Bromocriptine drugs have many side effects and are therefore prescribed with great caution;
- Quinagolide. It is rarely prescribed and has strict indications.
During the entire period of treatment, the level of prolactin in the blood is monitored. The patient should undergo regular blood tests and brain imaging. In the presence of macroprolactinomas, observation by an ophthalmologist is mandatory to reduce the risk of damage to the optic chiasm.
Possible side effects of dopamine agonist therapy:
- indigestion;
- headache, drowsiness or insomnia;
- postural hypotension.
Reducing the dosage of medications or completely stopping them is possible no earlier than 2 years after starting treatment. Therapy is stopped after long-term stabilization of prolactin levels at normal levels, with a decrease or complete absence of tumors according to MRI.
Treatment prognosis is favorable provided early diagnosis and proper treatment. After restoring hormonal balance, women are advised not to plan a pregnancy for the first 12 months.
Hyperprolactinemia and pregnancy
An increase in prolactin levels in the blood suppresses ovulation. Pregnancy is possible only with slight hyperprolactinemia. In other cases, it is impossible to conceive a child without prior treatment.
In the absence of therapy, more severe consequences of hyperprolactinemia develop:
- amenorrhea – complete absence of menstruation;
- anovulation – immaturity of the follicle and infertility;
- insufficiency of the corpus luteum of the ovaries - risk of miscarriage.
All of these complications lead to infertility.
At the same time, hyperprolactinemia, which occurs already during pregnancy, is the norm.
Diagnosis and treatment of hyperprolactinemia in Moscow
The MedEX Personal Medicine Clinic invites you to undergo a consultation with a specialist and all the necessary examinations in one place, which will allow you to quickly and accurately draw up a treatment plan for hyperprolactinemia. Call to select a convenient time to make an appointment.
Symptoms of hyperprolactinemia
As can be seen from all of the above, there are many causes of hyperprolactinemia. But the most common are still benign tumors of the pituitary gland (microprolactinomas), which are rarely large in size - usually they do not reach 1 cm.
Due to the fact that the causes of hyperprolactinemia are very diverse, the symptoms of the pathology can be very different - it all depends on the disease that led to this condition.
The main complaints with which women go to the doctor are menstrual irregularities or complete absence of menstruation. In cases where there is no menstruation, a woman does not ovulate, and this becomes the cause of infertility.
Another fairly common symptom of hyperprolactinemia is galactorrhea, a process in which milk spontaneously secretes from the mammary glands, and this is not associated with breastfeeding.
With a pituitary adenoma, vision can sharply deteriorate - this happens when the tumor begins to grow and put pressure on the optic nerve.
In men, symptoms of hyperprolactinemia manifest themselves in decreased sexual desire (libido), enlarged mammary glands, and discharge of colostrum from the breast. High levels of prolactin can gradually lead to impotence and infertility.
With hyperprolactinemia, osteoporosis, since prolactin helps suppress calcium in bone tissue.
The symptoms of hyperprolactinemia are quite varied, but any of these manifestations is a good enough reason to consult a doctor. It is important to remember that the progression of pathology often leads to infertility in both the female and male population.
Complications
The main and most common adverse consequence of hyperprolactinemia is primary infertility (up to 70%) associated with ovulatory dysfunction in women and oligo-or azoospermia in men. The stimulating effect of the hormone on the mammary glands provokes the development of mastopathy. Elevated lipid levels accelerate the process of atherosclerosis, which increases the risk of myocardial infarction.
More serious complications are caused by the growth of tumor formation. Long-term mechanical impact on the chiasm can cause atrophy of the optic nerves and lead to blindness. Due to compression of adjacent zones of the pituitary gland, other hormonal disorders occur - diabetes insipidus, panhypopituitarism. Rarely, when very large in size, prolactinoma compresses the brain stem or aqueduct and grows into the nasal cavity.
Diagnosis of hyperprolactinemia
Diagnosis of hyperprolactinemia, as in principle of any other disease, begins with collecting anamnesis and complaints. Then laboratory blood tests are prescribed for prolactin and thyroid hormones. A blood sample for prolactin is taken from a vein in the morning and always on an empty stomach. If an increased level of prolactin is detected, in order to avoid erroneous conclusions, the blood test is repeated three more times.
Next, instrumental diagnostics are prescribed, which includes x-rays of the skull in two projections. Such a study is done to assess the condition of a separate area of the brain - the sella turcica, as well as the size of the pituitary gland. The most complete picture and clear picture of the state of affairs is given by CT (computed tomography) and MRI (magnetic resonance imaging) of the brain. These examinations are currently the best methods for diagnosing pituitary gland pathologies. But they make sense only in cases where the diagnosis did not reveal any other causes of hyperprolactinemia, for example, taking medications or PCOS (polycystic ovary syndrome).
If a pituitary adenoma is detected in a patient, a consultation with an ophthalmologist is scheduled.
Some women who have both hyperprolactinemia and infertility may be indicated for laparoscopy, which will help identify the true cause of the pathology.
Treatment
The choice of therapy is determined by the reasons for the occurrence of increased prolactin levels, the general condition of the patient and other factors.
If hyperprolactinemia is caused by taking certain medications, the doctor will consider replacing it with another that does not have this side effect.
If the disease develops as a consequence of pituitary prolactinoma or adenoma, the patient is given drug treatment. Surgery is required in rare cases. Most tumors diagnosed with hyperprolactinemia are benign and do not progress, so there is no need for radiation therapy.
If the disease is accompanied by compression of the optic nerve and visual disturbances, more drastic treatment is selected. An ophthalmologist must be involved in drawing up a therapeutic regimen.
With secondary hyperprolactinemia, the main attention is paid to the root cause of the disorder - the disease that provoked an increase in prolactin secretion. In the idiopathic form of the disease, the patient’s hormonal levels are corrected.
Treatment of hyperprolactinemia
Hyperprolactinemia is treated in two ways - therapeutic and surgical. Drug therapy for hyperprolactinemia is aimed at stabilizing the normal level of prolactin in the blood. To do this, a course of hormonal drugs is prescribed that regulate the menstrual cycle, which, in turn, contributes in many cases to the treatment of infertility in women. Prolactin levels also decrease under the influence of thyroid drugs, which are used in the treatment of hypothyroidism (lack of thyroid hormones).
For those patients who have developed hyperprolactinemia as a result of pituitary hyperplasia or microprolactinemia and do not plan to have children in the future, it is enough to be regularly monitored by a specialist.
The semisynthetic drug bromocriptine (parlodel) has shown good results in the treatment of hyperprolactinemia - it suppresses excessive production of prolactin and activates the release of dopamine. Contraindications to the use of this drug are liver diseases. There are side effects such as general weakness, dizziness, fainting, and nausea.
Courses of treatment consisting of terguride, lisuride, cabergoline have fewer side effects for the body, however, the effectiveness in the treatment of hyperprolactinemia is lower than that of bromocriptine. Among other things, bromocriptine reduces tumor size in macroprolactinoma. This drug is also good because it can be prescribed both during pregnancy (short courses) and while breastfeeding. The only thing is that when treating hyperprolactinemia with Parlodel during pregnancy, it is necessary to constantly monitor an ophthalmologist and a neurologist.
In women suffering from infertility, the underlying disease is first treated, and only then a course of bromocriptine is prescribed in small doses.
Surgical intervention for hyperprolactinemia is done in cases where drug therapy has not had the desired effect, persistent resistance to bromocriptine and sharp progress of the process. Such operations are performed only in a hospital setting by experienced surgeons; their goal is to remove pathologically altered tissues or a tumor (adenoma) of the pituitary gland.
Infertility and hyperprolactinemia
Hyperprolactinemia is characterized by anovulation.
The fact is that this hormone influences the production of gonadotropins - pituitary hormones that regulate the growth and development of follicles, as well as the release of the egg from the ovary (ovulation). If prolactin levels are significantly elevated, FSH and LH are not produced in sufficient quantities, so fertilization does not occur.
In addition, high prolactin interferes with the production of estrogens, which are also involved in the regulation of the menstrual cycle.
Complications of hyperprolactinemia
Do not underestimate the severity and seriousness of the consequences for the human body that hyperprolactinemia can lead to if left untreated. This pathology can lead to the development of pituitary insufficiency, and this, in turn, causes disruption of the endocrine system - a person’s adrenal glands, thyroid gland, etc. begin to fail. Tumor growth quite often leads to deterioration of vision, and after a while - his complete loss. Patients with hyperprolactinemia often develop osteoporosis. And a pituitary tumor without timely treatment can develop from benign to malignant.
So, if you have any symptoms or signs of hyperprolactinemia, you should not postpone a visit to the doctor, otherwise the consequences of this disease can be very disastrous for you.
Diagnostics
To diagnose prolactinemia, the patient undergoes a study of hormones in the blood. Women should perform it on the 5-8th day of the menstrual cycle. Venous blood is taken to test for hyperprolactinemia.
If the study gives a positive result, it is repeated several times. The measure is needed in order to exclude a temporary increase in prolactin caused by physical activity, stress, active sex life and other factors.
If the doctor has suspicions that hyperprolactinemia has a secondary form, that is, it is a consequence of some other disease, he prescribes additional studies. Most often they are aimed at assessing the condition of the liver, adrenal glands, and thyroid gland. To exclude pituitary tumors that provoke increased secretion of prolactin and the development of hyperprolactinemia, MRI or CT is used. They also help diagnose disorders in the functioning of the ovaries, adrenal glands and other organs, often accompanying hyperprolactinemia.
Prevention of hyperprolactinemia
There are no special measures to prevent hyperprolactinemia. This disease does not require special recovery and rehabilitation methods. There is also no special diet or nutrition regimen. The lifestyle of a woman with hyperprolactinemia usually should not change; the most important thing is that she should avoid excessive physical and psycho-emotional stress.
After a course of treatment for hyperprolactinemia, the main difficulty is selecting suitable contraceptive methods for the patient, since the majority of oral contraceptives increase prolactin levels, and this is in no case acceptable. Intrauterine devices can also increase prolactin levels because they irritate the endometrial layer in the uterus. Based on all this, doctors advise women to undergo sterilization (if children are not planned in the future) or prescribe special contraceptives that do not affect prolactin levels.
Etiology of hyperprolactinemia
The following diseases lead to an increase in prolactin:
- Pathologies of the hypothalamus (tumors, infections, injuries);
- Diseases of the pituitary gland (tumors, “empty sella” syndrome);
- Hypothyroidism (decreased functionality of the thyroid gland);
- Use of medications (antidepressants, contraceptives, antiemetics and other substances);
- Uterine fibroids and polycystic ovary syndrome;
- Cirrhosis of the liver;
- Renal failure, chronic form;
- Various injuries to the chest, including herpes viral infection.
In addition, there are causes of hyperprolactinemia that are not associated with diseases - stress and excessive physical activity. These factors can lead to a physiological increase in hormone levels.
Prognosis for hyperprolactinemia
Advances in modern medicine, both in diagnostic methods and in methods of treating hyperprolactinemia, make it possible to achieve positive results in almost all cases. The outcome for the patient is usually favorable: the health status improves, the reproductive functions of the body are restored. To prevent relapse of the disease in the future, regular visits to specialists are necessary to monitor and control the level of prolactin in the blood. It is recommended to have a CT scan and a blood test for hormones once a year, as well as visit an ophthalmologist. If the patient strictly adheres to all the doctor’s recommendations, then hyperprolactinemia will most likely not return.
Primary appointment with an obstetrician-gynecologist: 2200 RUR.
Sign up Online 5% discount when registering from the site
Prevention
To avoid the development of pathology, it is necessary to eliminate factors that contribute to an increase in prolactin production.
If it is necessary to use drug therapy, especially psychotropic drugs, you should pay close attention to their side effects.
The choice of oral contraceptives should always be made by a doctor based on the results of the examination.
In order to promptly diagnose possible relapses, patients with hyperprolactinemia need to be observed by a specialist.