- home
- Urology
- Kidney cyst
A kidney cyst is a benign, thin-walled, voluminous formation that develops from the kidney parenchyma and usually contains serous fluid. A kidney cyst is a spherical cavity. Most often, patients are diagnosed with single renal cysts, up to 3 cm in diameter, located subcapsularly in the renal parenchyma. Cysts occur with approximately the same frequency in both the right and left kidneys. Large single cysts, renal sinus cysts, and multiple renal cysts are quite rare.
Kidney cyst symptoms
The degree of kidney damage varies from negligible with small solitary cysts to total with polycystic kidney disease, often leading to severe renal failure and hemodialysis.
Is a cyst on the kidney dangerous?
Large cysts often cause pain in the kidney area due to compression of both the kidney itself and adjacent organs. One of the signs of a kidney cyst is erythrocyturia (the appearance of red blood cells in a urine test). Patients with large or multiple kidney cysts often develop secondary hypertension (high blood pressure).
Therefore, accurate diagnosis and, most importantly, timely treatment of kidney cysts allows you to prevent complications and achieve maximum results.
Causes
The formation of a cystic cavity in the kidney occurs as a result of increased growth of connective tissue or epithelial cells. As a result, there is a lack of oxygen, which affects the functioning of the organ parenchyma. As a result, cells and tissues that are better adapted to anaerobic functioning begin to grow rapidly, thereby displacing cells of normal tissue.
The main reasons for the development of kidney cysts include:
- chronic and acute diseases of an infectious-inflammatory nature;
- diseases of the cardiovascular system;
- age-related changes in the human body;
- abnormal structure of kidney tissue;
- hormonal disorders.
There are parapelvic renal cyst, renal parenchymal cyst, simple renal cyst, and renal sinus cyst. Nephrologists say that the presence of obesity, diabetes mellitus or arterial hypertension can lead to their increased growth. People who have any of the above are at particular risk.
Kidney cysts classification
Depending on the structural features (according to computed tomography with intravenous enhancement) and the likelihood of tumor degeneration, kidney cysts are divided into 5 classes ( Bosniak classification of kidney cysts ).
| Class | 1 |
| Characteristics (according to MSCT data with intravenous contrast) | Thin-walled kidney cysts with homogeneous contents, the density corresponding to water and not accumulating contrast. |
| Treatment tactics | Does not require treatment or observation. It is advisable to have an ultrasound of the kidneys once a year. |
| Class | 2 |
| Characteristics (according to MSCT data with intravenous contrast) | The cysts contain single thin septa and small calcifications; Small areas of thickened and calcified wall or septum are allowed. Elements of the cyst do not accumulate contrast. |
| Treatment tactics | Does not require treatment or observation. It is advisable to have an ultrasound of the kidneys once a year. |
| Class | 2f |
| Characteristics (according to MSCT data with intravenous contrast) | The cysts contain multiple thin septa; Calcification and thickening of the cyst walls or septa are allowed. Cyst elements do not accumulate contrast |
| Treatment tactics | Ultrasound of the kidneys 1-2 times a year. |
| Class | 3 |
| Characteristics (according to MSCT data with intravenous contrast) | Renal cysts with unclear contours, uneven thickened walls or septa that accumulate contrast |
| Treatment tactics | Surgery. |
| Class | 4 |
| Characteristics (according to MSCT data with intravenous contrast) | Obviously malignant cysts that have all the characteristics of category 3, but with a soft tissue component that accumulates contrast |
| Treatment tactics | Surgery. |
As can be seen from the table, in most cases with kidney cysts, it is sufficient to monitor the size and structure of the cyst using an annual control ultrasound.
Treatment at the Yusupov Hospital
If patients with sinus cysts of the kidneys do not experience discomfort and bloody impurities in the urine, surgical intervention is not advisable. In such cases, it is sufficient to undergo a regular medical examination - at least once every six months.
Indications for surgical removal of a kidney sinus cyst are indicated in the presence of the following conditions:
- cyst rupture;
- cyst suppuration;
- suspicion of malignancy of the cystic formation;
- presence of blood in the urine;
- arterial hypertension provoked by an intrasinus renal cyst.
To remove a small sinus cyst of the left and right kidney, a percutaneous puncture can be performed, during which a sclerosing substance is injected into the cavity of the pathological formation.
The effective and most common method of surgical treatment of sinus cysts at the Yusupov Hospital is laparoscopic surgery.
Large cysts, suspicion of malignant degeneration of the formation, and cysts localized in close proximity to blood vessels require open surgery.
In addition, the open surgery method is used for patients suffering from concomitant diseases, such as urolithiasis.
Treatment of kidney cysts or how to treat a kidney cyst
Since kidney cysts are not tissue formations, it is useless to treat them with medications. Thus, the only option left is surgical treatment of kidney cysts , the options for which are the following (listed in order of increasing complexity and radicality):
- puncture of a kidney cyst under ultrasound control with sclerosis of its wall;
- laparoscopic excision of the walls of a kidney cyst (renal cyst laparoscopy);
- laparoscopic resection of the affected area of the kidney;
Indications for surgical treatment of a kidney cyst are large size (more than 5-7 cm), rapid growth of the cyst, clinical manifestations caused by the cyst (pain in the kidney area, erythrocyturia, increased blood pressure). Also, cysts belonging to categories III and IV according to the Bosniak classification are subject to mandatory surgical treatment.
Puncture and sclerosis of a kidney cyst under ultrasound control is an ideal method for treating thin-walled single cysts.
Prevention
At the moment, doctors have not found a way to specifically prevent the formation of kidney cysts. Based on the fact that the development of cystic formations can be caused by the influence of many factors, preventive measures should be comprehensive. Therefore, all patients need:
- timely treatment of infectious and inflammatory diseases of the genitourinary system;
- avoid situations in which the lumbar region can be injured;
- to live an active lifestyle;
- give up all bad habits.
Cyst in the kidney what to do
The procedure is simple, effective and safe, performed under local anesthesia and requires only minimal observation in the hospital for 24 hours.
Puncture of a cyst involves inserting a thin needle into its cavity under ultrasound control, aspirating the contents (emptying the cyst) and introducing a sclerosing agent, which causes gluing of the cyst walls and prevents re-accumulation of fluid (cyst recurrence).
For recurrent kidney cysts, as well as for multi-chamber or thick-walled cysts (when puncture and sclerotherapy under ultrasound guidance are ineffective), we perform laparoscopic excision of the walls of the kidney cyst (renal cyst laparoscopy) . This operation is performed under general anesthesia through three small punctures in the abdomen.
The advantage of laparoscopic renal cyst excision (renal cyst laparoscopy) is the absence of recurrence. The hospitalization period for this operation is from 3 to 5 days.
If the cyst is suspicious for malignancy (malignancy), then it is often necessary to perform laparoscopic resection of the kidney (or even laparoscopic nephrectomy, that is, removal of the kidney).
By contacting me with a problem such as kidney cysts, you can be sure of correct and timely diagnosis and adequate treatment, including modern high-tech minimally invasive procedures.
How to make an appointment with a specialist
You can make an appointment with a specialist by calling the reception at +7 (495) 775-73-60. Our clinic is located in the center of Moscow at the address: 2nd Tverskoy-Yamskoy lane, building 10, Mayakovskaya metro station.
The doctor will give directions for the necessary tests, carry out diagnostic measures and, if a cyst is present, prescribe the most optimal method of treatment. If an operation is performed, the specialist will give all recommendations for recovery and prescribe medications.
Questions about the article
Love
November 5, 2021 at 02:56 pm
The cyst on the right is 7.2 in size, doesn’t bother me, is surgery necessary? And also, is it possible to sleep on the right side? Yesterday at the ultrasound they said that it is not advisable, it may burst. Is it so?
Anton Evgenievich Rotov
November 6, 2021 at 12:58 pm
The size of the cyst is quite large and may be the basis for surgical treatment. The decision here is made individually, taking into account your age, health status, and level of physical activity. Don’t worry about the position in your sleep, it won’t burst
Boris
October 15, 2021 at 12:00
My 85-year-old mother has a cyst on one kidney, but it is large. Is it necessary and possible to operate?
Anton Evgenievich Rotov
October 15, 2021 at 04:16 pm
I wouldn't do surgery at this age. Still, it’s not a tumor and doesn’t pose a threat to life.
Panfilova Irina
September 26, 2021 at 10:23 am
Good afternoon. Thanks for the answer! I received a description of the MRI: “MR picture of a complicated cyst of the left kidney, with hemorrhagic contents, with traces of deposition of hemoglobin breakdown products in the area of the cyst capsule, taking into account the reduction in the size of the cyst, one can assume a condition after the rupture of the cyst; areas of contrast accumulation in the cyst wall and along the renal capsule may also be associated with cyst rupture; a neoplastic process is less likely. Cysts of the right kidney (Bosniak2).
Anton Evgenievich Rotov
September 27, 2021 at 08:20
Taking into account the MRI description, observation is possible - control MRI with contrast after 3 months
Panfilova Irina
September 25, 2021 at 10:09 pm
Good evening. An ultrasound showed that the cyst in the left kidney had changed since last year. In the conclusion it is written: complicated cyst of the left kidney Bosniak lll (reduction in size, increase in density and thickening of the wall in dynamics from 01.21. I am 59 years old. Do I need to operate on it?
Anton Evgenievich Rotov
September 26, 2021 at 06:10
Of course it is necessary. Bosniak type 3 cyst is an indication for surgical treatment
Diagnostics
Diagnosis of this disease most often occurs by chance during a preventive medical examination or during the treatment of other nosologies. After identifying a cyst in the right kidney, additional research is necessary. At JSC "Medicine" (clinic of academician Roitberg) - 2nd Tverskoy-Yamskaya lane 10 - the clarifying methods are:
- laboratory blood and urine tests;
- ultrasound examination of the abdominal and pelvic organs;
- MRI of the kidneys, abdominal cavity and pelvic organs.
How to prevent relapse?
Timely seeking medical help can alleviate the course of the disease and significantly reduce the duration of treatment.
To prevent recurrence of the cyst, you must follow a special diet. It is worth limiting the consumption of liquid, salt, fried and spicy foods, and foods high in protein. Smoking and drinking alcohol are also contraindicated.
The diet is not able to cure a patient from an already formed cyst, but in combination with competent treatment and constant medical supervision, it helps the patient feel good and avoid relapses of the disease.
Attention!
This article is posted for informational purposes only and under no circumstances constitutes scientific material or medical advice and should not serve as a substitute for an in-person consultation with a professional physician.
For diagnostics, diagnosis and treatment, contact qualified doctors! Number of reads: 21117 Date of publication: 09/21/2017
Urologists - search service and appointment with urologists in Moscow
The use of ultrasound and CT in the diagnosis of cystic renal formations of categories I and II
Ultrasound scanner HS50
Affordable efficiency.
A versatile ultrasound scanner with compact design and innovative capabilities.
Introduction
A simple (solitary) kidney cyst is a benign, thin-walled, volumetric formation that develops in the kidney parenchyma, clearly separated from the main parenchyma by a fibrous capsule (which is lined with squamous or cuboidal epithelium), usually containing serous fluid. According to various authors, simple renal cyst occurs in 1.8 to 50% of cases [1-4]. With the use of ultrasound and CT in clinical practice, the number of detected solitary renal cysts has increased significantly in the examined patients with urological pathology. Simple kidney cysts are observed more often at the age of 50 years and older, occurring more often in men than in women in a ratio of 3:2 to 2:1.
It is believed that the following classification of simple renal cyst is convenient in clinical practice: 1) congenital or acquired; 2) one-sided or two-sided; 3) single or multiple; 4) serous, hemorrhagic or infected; 5) intraparenchymal, cortical, peripelvic, subcapsular.
Three main theories of the pathogenesis of simple renal cysts are generally accepted.
- Retention-inflammatory. The cyst develops as a result of obstruction of the tubular and urinary tracts, as well as inflammation, including that occurring during intrauterine life.
- Proliferative-neoplastic. The cyst arises as a consequence of excessive proliferation of the renal epithelium (urothelium) with frequent malignant transformation.
- Embryonic. The cyst develops as a result of a defective connection between the filtration and secretory parts of the metanephrons and the excretory tissue of the mesonephric ducts (Wolfian ducts).
Most simple kidney cysts are asymptomatic and are detected incidentally during examination of an adult. In other situations, against the background of abnormalities in the structure of the kidney parenchyma, various diseases and complications develop.
Pain in the lumbar region occurs in 66.3-90.8% of patients, is usually dull in nature and is explained by an increase in intrarenal pressure or tension of the neurovascular plexus along the renal pedicle, or an acute violation of the outflow of urine from the pyelocaliceal system.
The next symptom is hematuria, caused by an increase in venous pressure in the fornical veins, due to twisting or even bending of the vein through the renal artery (when the upper pole is tilted with a cystic formation anteriorly), as well as as a result of hemodynamic disorder (with torsion of the vascular pedicle) due to pathological mobility of the kidney. This symptom, according to various authors, occurs in 18-64.2% of cases.
A palpable tumor-like formation is detected in 7.6-52% of patients, and pyuria when cystic formations are combined with pyelonephritis - in 56.3-78.8%.
Opinions about the effect of simple cysts on the functional state of the kidneys are contradictory. Some authors believe that the presence of a cystic formation is accompanied by a violation of the excretory function of the kidney, while others deny this influence.
Some authors believe that the presence of a cystic formation leads to arterial hypertension, which is caused by increased production of renin. This symptom occurs in 7.1-44% of patients and most often with polycystic kidney disease.
Simple renal cysts can be complicated by infection in 1.48-51% of cases, hemorrhage in 0.44-31%, or rupture of the cyst wall in 0.89-18% of cases.
Against the background of abnormalities in the development of the kidneys, various diseases (chronic pyelonephritis, hydronephrosis, nephrolithiasis) occur twice as often, while the threat of such dangerous complications as chronic renal failure and nephrogenic hypertension increases many times over.
Laboratory research methods (blood and urine tests) in the diagnosis of cystic kidney diseases make it possible to obtain information about the functional state of the kidneys and to identify the presence of an inflammatory process in the urinary system.
With the availability of more informative diagnostic methods, traditional radiological research methods (survey and excretory urography, retrograde pyelography) can no longer meet modern requirements for diagnosing simple kidney cysts. They should be considered as auxiliary methods that make it possible to clarify some anatomical and functional features of the kidneys, to determine the presence or absence of a violation of the outflow of urine from the kidney, and concomitant urological pathological changes.
Due to its high information content, ultrasonography has become one of the leading methods for detecting simple renal cysts. Ultrasound allows you to identify the cystic nature of the space-occupying formation, assess the clarity of the contours, determine the size and location, and clarify the relationship with adjacent organs. In 90% of observations, this method makes it possible to determine further tactics for the patient. In addition, ultrasound is one of the reliable methods for monitoring the safety of diagnostic and therapeutic punctures of kidney cysts. This method is non-invasive, cost-effective, does not cause inconvenience to the patient, is easy to perform, usually does not require patient preparation, does not depend on the functional state of the kidneys, does not pose a risk of radiation, and allows for dynamic monitoring and screening [1-16].
Kidney CT is the most accurate method for diagnosing kidney cysts. It is the method of choice for resolving the issue of a possible oncological process, assessing the state of blood supply to the formation, determining the size, contours, and distribution of the formation inside and outside the kidney. CT makes it possible to obtain a highly informative direct image of the structure of the kidneys and existing tumors, to judge their shape and size in a comparative aspect, and to determine the “density” values of different tissue areas [1-13, 15, 16].
The advantages of CT are manifested when performing the so-called “enhancement technique,” which consists of intravenous administration of water-soluble iodinated contrast agents. Unlike cysts, malignant neoplasms accumulate radiocontrast agent, and the density of the tumor increases by more than 5-15H.
Diagnostic punctures of kidney cysts should be used when conflicting results are obtained from previous examination methods. In addition, the diagnostic part of the puncture method for a simple kidney cyst naturally turns directly into a therapeutic effect and in the vast majority of cases ends with the introduction of sclerosing substances into the cyst cavity [1, 3, 4, 8, 12].
The first category is a simple solitary renal cyst. On ultrasound, a simple renal cyst appears as an echo-negative formation of a round or oval shape. Characterized by the absence of visualization of the walls and internal structures in the formation, clear, even, continuous contours. There may be a dorsal enhancement effect according to the volume of the cyst (Fig. 1).
Rice. 1.
Echograms of a simple kidney cyst (category I).
A)
The formation has a round shape, clear, even contours. The wall is not visible, internal structures and partitions are absent.
b)
The cyst has echo-negative contents and a clear mirror artifact (dorsal enhancement effect).
A simple renal cyst on CT is visualized as a homogeneous round formation without a visible capsule, clearly demarcated from the normal parenchyma. The formation has a homogeneous, relatively low density, corresponding to the density of water (0...+20N). On CT with intravenous enhancement, the density, size and shape of the formation do not change (Fig. 2).
Rice. 2.
Computed tomograms of multiple simple cysts of a single right kidney (category I).
A)
Before contrasting, three homogeneous round formations with clear, even contours, without a visible capsule, and uniform density characteristic of water are determined.
b)
After administration of a contrast agent, the cysts do not change shape, size or density.
If the cyst is small in size and the CT examination is made in thick sections, then a density averaging effect or a partial volumetric effect may be observed (the phenomenon of partial volume in small formations). If small formations are detected, an additional study is carried out with thin callimation of the X-ray beam (thin sections): the width of the callimation of the X-ray beam is a maximum of 1/2 of the diameter of the cyst.
Observation 1
Patient I., 41 years old, was admitted to the Kemerovo Regional Clinical Hospital with complaints of pain in the lumbar region on the left. The pain has been bothering me for several years. During follow-up 3 years ago, an ultrasound revealed a cyst in the left kidney; upon admission, dynamic growth of the cyst was detected. An objective examination did not reveal diagnostically significant abnormalities in the physical status. General and biochemical blood tests, general urine analysis are within normal limits.
Excretory urography.
The kidneys are located in a typical manner, the right kidney is of normal size, excretory function is preserved on both sides.
On the left, the kidney is increased in size in the projection of the lower pole due to an additional formation up to 50 mm in diameter. No deformation of the pyelocalyceal system was detected. Conclusion:
Space-occupying lesion in the projection of the lower pole of the left kidney.
Ultrasound examination of the kidneys.
The kidneys are located typically.
The contours are smooth, clear, mobility is preserved, the cavity system is not expanded. The ureters are not visualized. No stones were identified. In the projection of the lower pole of the left kidney, extrarenally, an echo-negative formation of a round shape, up to 50 mm in diameter, with clear, even, continuous contours is visualized, the wall is not visible, and there are no internal structures. There is a dorsal enhancement effect. Conclusion:
Category I cyst in the projection of the lower pole of the left kidney. Dynamic growth of the cyst when compared with the previous ultrasound (Fig. 3).
Rice. 3.
Observation 1. Echogram of a simple cyst of the left kidney (category I).
CT scan.
In the lower pole of the left kidney, a homogeneous formation with clear contours, round in shape, homogeneous in echostructure, without signs of a capsule, clearly demarcated from normal parenchyma, with a uniformly reduced image density to +7 HU on the Houndsville scale, diameter 50 mm is determined.
After the introduction of a contrast agent, the formation does not change its shape, size and density. Conclusion:
Category I cyst in the projection of the lower pole of the left kidney (Fig. 4).
Rice. 4.
Observation 1. Computer tomograms of a simple cyst of the left kidney (category I).
A)
Before contrasting.
b)
After administration of contrast agent.
Considering the benign nature of the cyst, the patient underwent a therapeutic and diagnostic puncture under ultrasound guidance, followed by sclerotherapy: under local anesthesia with 0.25% novocaine, a puncture of the left kidney cyst was performed. 50 ml of light serous fluid was removed and sent for cytological examination. 96% alcohol was introduced in a volume of 1/10 of the removed liquid, exposure was 5 minutes, the alcohol was removed.
A cytological examination of the fluid did not reveal any cellular elements.
An ultrasound scan performed after 1, 3, 6 and 12 months did not reveal any fluid formations in the left kidney (Fig. 5).
Rice. 5.
Observation 1. Ultrasound of the kidney after 12 months.
No recurrence of the cyst was observed in this patient during dynamic ultrasound for four years.
The second category is benign cystic formations, minimally complicated cysts, but raising some doubts based on the results of radiological diagnostics. Most often these are cysts after hemorrhage or inflammation, having a more complex structure than simple cysts. Therefore, both definitions of cysts - complex (by structure) and complicated (inflammation, hemorrhage) - have diagnostic confirmation. In Russian-language literature, the term “complex cysts” is more often used, since the concept “complicated” is often associated with malignancy. However, the first term also does not quite accurately define the essence of the concept of “complicated cyst”.
The first criterion that forces a formation to be classified as category II is visualization of the cyst wall by ultrasound and/or CT (Fig. 6, 7).
Rice. 6.
Echogram of a complex (cortical) cyst (category II) and a simple cyst of the left kidney.
A thin, smooth wall of the cortical cyst is clearly defined.
Rice. 7.
Computer tomograms of a complex (cortical) cyst (category II) of the left kidney and a pair of pelvic cysts of both kidneys.
A)
Before intravenous contrast (a bulging of the lateral contour of the left kidney is detected, suspicious for a neoplasm).
b)
After contrast (the formation along the lateral contour does not change density and becomes hypodense in relation to the renal parenchyma; parapelvic cysts do not accumulate the contrast agent).
The presence of a septum is a second, no less important and independent sign. Category II cysts are characterized by the presence of single thin, even septa, 1 mm or less thick, adjacent to the walls of the cysts without visible thickening. With contrast-enhanced CT, a previously invisible septum may accumulate contrast agent and become visible.
Observation 2
Patient S., 49 years old, was admitted to the Kemerovo Regional Clinical Hospital with complaints of pain in the lumbar region on the right. Ill for a month. Upon examination, no diagnostically significant deviations in the physical status were revealed. General and biochemical blood tests, general urine analysis are within normal limits.
Ultrasound examination of the kidneys.
The kidneys are located typically.
The contours are smooth, clear, mobility is preserved, the cavity system is not expanded. The ureters are not visualized. No stones were identified. In the right kidney, in the middle segment, extrarenally, an echo-negative formation with a diameter of up to 60 mm is visualized, with clear, even, continuous contours, a clear wall, there is a dorsal enhancement effect, in the cavity of the cyst a solitary septum 1 mm thick is visualized, which is attached to the wall of the cyst without visible thickening. Conclusion:
Cyst of the right kidney of the middle segment of category II (Fig. 8).
Rice. 8.
Observation 2. Echogram of a complex cyst of the right kidney (category II).
CT scan.
In the right kidney, in the middle segment, a homogeneous formation with clear contours, round shape, uniformly reduced density +6 HU on the Houndsville scale, with a diameter of up to 60 mm is determined.
There are no signs of a capsule, the cyst is clearly separated from the normal parenchyma. After the introduction of a contrast agent, the formation does not change its size, shape and density. In the cavity of the formation, a solitary septum is determined, up to 1 mm thick, which accumulates contrast when contrasted. Conclusion:
Cyst of the right kidney of the middle segment of category II (Fig. 9).
Rice. 9.
Observation 2. Computed tomogram of a complex cyst of the right kidney (category II).
For therapeutic purposes, under local anesthesia with 0.25% novocaine, a double therapeutic and diagnostic puncture of the right kidney cyst was performed, followed by sclerotherapy. 60 ml of light serous fluid was removed and sent for cytological examination. 96% alcohol was introduced in a volume of 1/10 of the removed liquid, exposure time was 5 minutes, the alcohol was removed (Fig. 10).
Rice. 10.
Observation 2. Therapeutic and diagnostic puncture under ultrasound control. The tip of the needle is clearly visible.
A cytological examination of the fluid did not reveal any cellular elements. Dynamic ultrasound after 1, 3, 6 and 12 months did not reveal any fluid formations in the right kidney (Fig. 11).
Rice. eleven.
Observation 2. Ultrasound of the kidney after 12 months.
No recurrence of the cyst was noted during follow-up for four years.
The next diagnostic sign that allows the formation to be classified as category II is the nature of calcium deposits (features of calcification). Before the existence of CT, the main method for determining calcifications was X-ray, which is effective in 4-11%. In addition, detection of calcifications during X-ray examination does not allow determining the nature of the formation (cyst, echinococcosis, abscess, tuberculosis, angiomyolipoma, tumor). Currently, the main method for diagnosing calcifications is CT. The presence of calcifications in a cyst is always an alarming sign of possible malignancy. But despite this, small linear calcifications can occur in the wall or septum of benign cysts. The size and shape of calcifications are especially important in differential diagnosis.
If all other radiological signs obtained from ultrasound and CT define the cyst as a benign formation, then the presence of a single calcification in the solitary septum in the form of a thin linear focus (without the presence of areas of tissue density in the formation) does not contradict the definition of this cyst as complex, but does not malignant, and allow us to classify it as category II (Fig. 12, 13).
Rice. 12.
Echogram of a complex cyst of the right kidney (category II).
The echo-negative formation is round in shape, with smooth contours, a clear wall and a dorsal enhancement effect. A single septum with calcification is visualized in the cyst cavity.
Rice. 13.
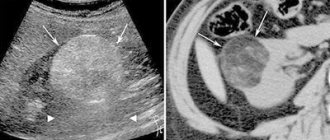
Computed tomogram of the right kidney with contrast.
Complex cyst of the right kidney (category II). The formation (arrow) has a round shape, smooth contours, and a clear wall. The density of formation corresponds to the density of water. A single septum with linear calcification in it is visible in the cavity of the formation.
Single calcifications in the form of linear lesions can also be located in the cyst near the wall. If all other signs of a simple renal cyst are preserved on ultrasound and CT, then the formation can be considered benign (Fig. 14, 15).
Rice. 14.
Echograms of complex renal cysts (category II).
A)
Several calcifications are visualized near the wall.
b)
A single large calcification is visualized near the wall.
V)
Several parietal calcifications of linear shape are visualized.
Rice. 15.
Computer tomograms of a complex cyst of the right kidney (category II).
A)
Before intravenous contrast, the formation is practically not detected, only dotted calcification is visible.
b)
After contrasting, an irregularly shaped cyst is identified, with single wall calcification.
Category II also includes formations of increased density during CT scanning (in particular, hemorrhagic cysts). An ultrasound scan in such patients confirms the fluid nature of the formation. But here, performing CT with intravenous “amplification” is of particular importance. Hemorrhagic cysts are characterized by thickened walls, increased echogenicity on ultrasound, and increased density on CT. Cysts (unlike tumors) do not accumulate contrast agent and do not change their density (Fig. 16).
Rice. 16.
Computer tomograms of a complex (hemorrhagic) cyst (category II) and a simple cyst of the left kidney.
A)
Before intravenous contrast, a round homogeneous formation with clear contours, soft tissue density of a complex hemorrhagic cyst and a simple cyst is determined.
b)
After contrast, both cysts do not change their size, shape and density.
Literature
- Alyaev Yu.G., Amosov A.V., Gazimiev M.A. Ultrasound methods of functional diagnostics in urological practice. M.: Publishing house. R. Valent., 2001.
- Akhmetov N.R. Surgical treatment of solitary renal cysts: dissertation. ...cand. honey. Sci. Ufa, 2000.
- Gromov A.I. Diagnostic approach to accidentally detected small pathological formations in the kidneys // Modern radiation diagnostics in a multidisciplinary medical institution. St. Petersburg, 2004. pp. 87-88.
- Palmer P.E. Guide to Ultrasound Diagnostics. WHO Geneva. M.: Medicine, 2000.
- Alyaev Yu.G., Krapivin A.A., Grigoriev N.A. Features of diagnosis of kidney tumors up to 4 cm // Med. visual 2003. N2. pp. 33-39.
- Alyaev Yu.G., Krapivin A.A. Kidney resection for cancer. M.: Medicine, 2001.
- Alyaev Yu.G., Krapivin A.A., Al-Agbar N.I. Small kidney tumor // Urology. 2002. N2. pp. 3-7.
- Rublevsky V.P., Rublevsky B.V., Ilyinskaya E.V., Likhachev A.G. Minimally invasive surgery of the retroperitoneal organs using a retroperitoneoscope. Materials of the scientific-practical conference “Current issues of urology”, Kemerovo, InSEPZ. 2002. pp. 129-132.
- Trapeznikova M.F., Glybin P.A., Morozov A.P. and others. Angiogenic factors in renal cell carcinoma // Oncourology. 2008. N4. pp. 82-87.
- Khinman F. Operative urology: Atlas: Transl. from English M.: GEOTAR-MED. 2001.
- Bruyn R., Gordon I. Imaging in cystic renal disease // Arch Dis Child. 2000. V. 83. P. 401-407.
- Brian D. Davison MR Imaging of Renal Masses Interpreted on CT to Be Suspicious // AJR. 2000. V. 174. P. 1017-1022.
- Chung BH, Kim JH, Hong CH Comparison of single and multiple sessions of percutaneous sclerotherapy for simple renal cyst. BJU Int. 2000. V. 85. N 6. P. 626-627.
- Delakas D., Karyotis I., Loumbakis P. Long-term results after percutaneous minimally invasive procedure treatment of symptomatic simple renal cysts // Int Urol Nephrol. 2001. V. 32. N 3. P. 321-326.
- Hashimoto Y., Kimura G., Tsuboi N. Usefulness of power Doppler ultrasound in a patient with renal cell carcinoma in the wall of a simple renal cyst // Hinyokika Kiyo. 2001. V. 47. N 5. P. 325-327.
- Scialpil M., Di Maggio A. Small Renal Masses // AJR. 2000. V. 175. P. 751-755.
Ultrasound scanner HS50
Affordable efficiency.
A versatile ultrasound scanner with compact design and innovative capabilities.
When is surgery needed?
The need for surgical intervention arises in cases where it is not possible to puncture the cyst, and also when the following is observed:
- persistent increase in blood pressure;
- intense pain syndrome;
- noticeable impairment of kidney function;
- risk of transformation into a malignant form;
- the size of the tumor is huge, compression of organs occurs;
- the likelihood that the membranes of the cyst will rupture.
During the operation, both simple removal of the kidney cyst and its partial resection are performed. If the tumor has led to complete dysfunction of the organ, then its complete removal (nephrectomy) is necessary.
Complications from the disease
The likelihood of developing serious consequences with a kidney cyst directly depends on the size of the tumor. Large cysts lead to compression of the ureters and renal vessels, resulting in the following complications:
- reverse flow of urine, as a result of which kidney toxins spread throughout the body, infecting it (as a rule, this complication is characteristic of polycystic disease, in which both kidneys are affected);
- renal failure, which occurs as a result of decreased kidney function and its subsequent death.
Any traumatic impact can lead to rupture of the cyst, which is an emergency condition that requires immediate surgical intervention.
Surgical treatment is also required when suppuration forms in the cyst and the associated abscess, which threatens to infect the entire body of the patient, especially if his immune system is weakened.
Make an appointment
Forecast
The prognosis of a kidney cyst depends on the nature of the formation, its location and size. In most cases, relatively small single-chamber cystic vesicles with slow growth are diagnosed. They are asymptomatic and have favorable prospects. Patients are monitored by nephrologists. Patients are periodically examined for timely detection of possible complications.
In polycystic and multilocular forms of the disease, the prognosis worsens, as the risk of malignancy and the development of chronic renal failure increases. With radical treatment of these types of renal parenchymal cysts, complications and relapses are extremely rare.