An ovarian dermoid cyst (teratoma) is a neoplasm consisting of tissues that are not typical for this organ. The causes of the pathology are associated with the appearance of anomalies during intrauterine development, which contributed to the formation of teratoma. In most cases, the tumor is benign, but there is a possibility of its malignant degeneration. Treatment of dermoid cysts is successfully performed at the Yusupov Hospital, where experienced gynecologists work who will prescribe the necessary diagnostics and adequate therapy. Appointments with specialists can be made by telephone.
Ovarian dermoid cyst: ICD-10 code
The dermoid type of cyst accounts for 20% of all types of ovarian cysts. The pathology is a congenital anomaly and may not show itself for a long period of time. It can be discovered accidentally during a routine examination or diagnosis of pelvic organ disease.
Unlike ordinary cysts, which are characterized by the accumulation of fluid, cell division occurs in dermoid cysts. Such a cyst is a dense epithelial node with a capsule (usually single-chamber), which contains elements of germinal tissue: hair, teeth, bones, glands, etc. The size of the node can reach 15 cm in diameter, which significantly worsens the woman’s health.
According to ICD-10, a dermoid cyst belongs to the class of benign neoplasms (D10-D37). It has code D27 - benign ovarian neoplasm. In 1-3% of cases, malignant degeneration of the tumor occurs, which requires mandatory consultation with an oncologist.
Immature teratomas, in which active cell division is observed, are prone to malignancy. They can grow into neighboring tissues and metastasize. Moreover, more often the oncological process is detected not in the primary tumor, but in metastases.
Ovarian dermoid cyst: causes
The reasons for the development of ovarian dermoid cysts are not fully understood. Doctors cannot name the exact conditions in which teratoma develops. The most common theory is a failure in the development of identical twins, when one twin absorbs the other. Proof of this is the contents of the dermoid cyst: underdeveloped bone and cartilage tissue, epithelium, hair, elements of glands and other organs that are not related to the ovaries.
A dermoid cyst occurs in utero and develops during human growth. Having reached a certain size, it stops growing. In this case, she is called mature. If the process of cell division continues and it is active, then an immature cyst is implied, the presence of which requires consultation with an oncologist.
Among the reasons for the formation of a dermoid cyst, there are provoking factors that negatively affect the course of pregnancy and can cause various fetal abnormalities:
- Viral and bacterial diseases of the body;
- Infectious diseases of the pelvic organs;
- Presence of bad habits (alcoholism, smoking, drug addiction);
- Food and toxic poisoning;
- Effect of radiation;
- Overdose and uncontrolled use of certain medications.
The impact of a negative factor on the body of a pregnant woman does not necessarily guarantee the appearance of teratoma. However, in this case the woman is at risk of developing fetal pathologies.
Diagnostics
Clinically, a dermoid cyst will be detected visually during examination by an oncologist surgeon. After all, a cyst can be seen as a round formation in any part of the body, of various sizes from several millimeters to several centimeters, and moves freely under the skin.
The diagnosis is made on the basis of a preliminary examination using ultrasound of the pelvic organs, laparoscopy with further microscopic examination of the contents and structures of the cyst. Sometimes the cyst is punctured and the tissue is examined under a microscope. Additional research methods are MRI (magnetic resonance imaging) or CT of the pelvic organs.
To obtain complete information about the diagnosis and treatment of dermoid cysts, you must make an appointment with a surgeon or oncologist. Consulting a doctor will help you decide on further examination and treatment tactics.
Ovarian dermoid cyst: symptoms
Signs of pathology will depend on the type of neoplasm (mature or immature) and its size. In many cases, the cyst does not manifest itself for a long period of time, so if the disease is asymptomatic, it is difficult to detect.
A mature cyst will have the following symptoms:
- Abdominal pain;
- Unpleasant sensations during sexual intercourse;
- Increased urination;
- Difficulty in defecation.
It should be noted that with a dermoid cyst, the menstrual cycle is not disrupted. The neoplasm does not affect the woman’s hormonal levels and the process of menstruation.
An immature cyst is also characterized by pain in the lower abdomen, as well as general malaise. It is associated with tumor progression. As a result, a woman may suddenly lose weight and experience general symptoms of cancer intoxication.
A dermoid cyst has a stalk that attaches it to the ovary and through which blood channels pass. The presence of a leg is accompanied by the risk of torsion. This is a serious complication that can lead to necrosis of the node and the development of peritonitis. In this case, acute abdominal pain occurs, body temperature rises, and nausea and vomiting may occur.
Symptoms
This pathology, like other benign formations, may not manifest itself for a long time. A dermoid cyst on the eyelid can be detected upon careful examination as a slightly elongated or rounded elastic “ball” localized under the skin. Symptoms of formation usually appear when it becomes inflamed, suppurates, increases in size, and begins to put pressure on nearby tissues and organs.
A cyst on the eyelid is characterized by the following:
- Usually has a round shape;
- Elastic and dense to the touch;
- Painless on palpation;
- Does not adhere to the skin;
- The skin over the dermoid cyst on the eyelid is of a normal color, without ulcerations, rashes, etc.;
- It does not increase in size for a long time.
The clinical manifestations of a dermoid cyst on the eyelid are usually determined by its size and the age of the patient. Dermoids, which are small in size, do not affect health and do not cause damage to the eye structures. With small sizes, this is just a cosmetic defect. However, as the formation begins to grow, it begins to interfere with clear vision. In addition, the risk of its inflammation and malignancy (the appearance of malignant properties) increases, which becomes the reason for its mandatory removal.
Ovarian dermoid cyst: treatment
The only effective treatment for teratoma is surgical removal. The extent of the operation will depend on the size of the tumor and accompanying circumstances. Most often, treatment is performed laparoscopically.
In case of a benign course of the disease, the cyst is removed along with the ovary and the upper part of the uterus. If it is necessary to preserve reproductive function, the decision to remove the ovary is made individually.
Laparoscopy of ovarian dermoid cyst has positive reviews from both doctors and patients. The operation is quick and the woman can go home the same day. The decision on short-term medical examination is made individually. The operation has a short recovery period and is performed without an abdominal incision. After it is carried out, there are no scars left that would have a negative aesthetic appearance.
In the case of oncological degeneration of the tumor, the appendages are removed along with the uterus. Additionally, a course of chemotherapy is drawn up. Radiation therapy in this case is ineffective.
At the Yusupov Hospital you can undergo a full course of treatment for dermoid cysts, including examinations using the latest equipment. Treatment is prescribed strictly individually based on diagnostic results by experienced gynecologists and oncologists (in case of a malignant process). This approach ensures maximum effectiveness of the prescribed therapeutic measures.
Treatment in preparation for the ART program
The presence of an ovarian cyst, as a rule, is a contraindication to the use of assisted reproductive technologies. It is recommended to start the program upon completion of treatment.
Follicular and luteal cysts are subject to observation or conservative treatment. Tactics are determined taking into account the medical history, the size of the tumor, and the presence of symptoms. Conservative therapy involves the use of hormonal agents. If there is no effect, large functional cysts are removed.
Organic types of cysts are subject to surgical treatment. In preparation for ART, operations are performed as planned using low-traumatic laparoscopic techniques. The implementation of the program begins after the completion of the rehabilitation period.
Prevention and prognosis
Mature teratomas have a favorable prognosis. Due to the presence of a stalk of the tumor, it is recommended to remove it even if it does not cause discomfort. Otherwise, there is a risk of sudden torsion of the leg with subsequent inflammation. In addition, with a teratoma, a woman is at risk of complicated pregnancy.
Immature dermoid cysts have a poor prognosis. They undergo long-term treatment followed by constant monitoring of the condition.
There is no specific prevention that would guarantee the absence of the development of ovarian dermoid cysts. The main actions are aimed at reducing the risk of abnormal pregnancy in order to prevent the development of a pathological process in the fetus. They include a healthy lifestyle before and during pregnancy, a balanced diet, the absence of bad habits, and a responsible attitude towards your health.
At the Yusupov Hospital, you can undergo regular gynecological examinations, which will allow you to suspect pathology in time. Gynecologists at the Yusupov Hospital provide consultations to women planning a pregnancy to eliminate possible risks for the mother and unborn child.
Types of epidermal cysts
Doctors distinguish several types of formations. Classification is carried out according to structure, symptoms and the presence of complications.
The most common diagnosis is atheroma. This formation is localized in the face, arms, neck and scrotum. A single atheroma may appear on the skin or several may appear at once.
This type of epidermal cyst, such as atheroma, has a round shape and soft contents. As a rule, this formation is yellow or red in color.
Atheroma does not bother a person; it can remain the same size or rise slightly above the skin.
When an infection occurs, the formation suppurates and leads to inflammation of neighboring tissues.
Treatment
Treatment of cysts can be either conservative or surgical. In the presence of functional neoplasms, a wait-and-see approach can be used, but the patient is under constant medical supervision to avoid the development of complications.
Conservative therapy involves the prescription of hormonal drugs. If the desired treatment results are not observed within 2-3 months, an operation (cystectomy) is performed, during which the cyst is removed, trying to preserve the ovarian tissue as much as possible.
There are two types of cystectomy:
- Laparotomy (traditional). An incision is made in the abdominal wall through which the ovary is accessed. The cyst and pathological tissue areas are removed, then the incision is sutured. This is a traumatic operation with a fairly long recovery period. Therefore, nowadays this method is rarely used, mainly in the presence of huge cysts, adhesions, malignancy or rupture of the tumor.
- Laparoscopic. Surgery is performed through pinpoint incisions in the abdominal wall using a laparoscope. During the operation, carbon dioxide is pumped into the abdominal cavity for the best view. First, the cyst is opened, then its contents are removed, after which the empty capsule is removed. Electrocoagulation of blood vessels (“cauterization” with current) can also be performed. Laparoscopic surgery is less traumatic than classical surgery, the recovery time after it is much shorter, but it is not indicated in all cases. It is carried out for small cysts, the absence of purulent processes and changes in the function of the appendages.
Laser removal of ovarian cysts is a type of laparoscopic surgery. It is carried out using laser beams rather than a scalpel.
In some cases (with particularly large cysts, a high risk of developing cancer, large-scale inflammatory processes in the ovary), cystectomy may not give the desired result. Then the following are carried out:
- Ovarian resection. An operation during which, in addition to removing the cyst, excision of ovarian tissue is also performed.
- Ovariectomy. The cyst is removed along with the ovary.
- Adnexectomy. Not only the ovary, but also the fallopian tube is removed.
Types of cysts
Experts classify cysts based on their structure and the cause of their appearance. There are functional, organic, paraovarian, and endometrioid cysts.
Functional cysts
A functional cyst looks like a bubble with liquid, watery or serous contents. Develops due to improper functioning of the ovary and menstrual irregularities. The peculiarity of a functional cyst is that it exists for a fairly short time (up to 3 months), is not dangerous to health, and in most cases resolves on its own.
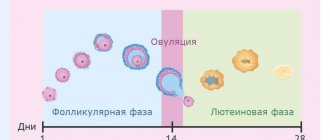
The most common types of functional cysts: luteal and follicular .
A luteal cyst appears after ovulation as a result of stagnation of a large amount of fluid in the corpus luteum.
A follicular cyst occurs if the follicle has not undergone physiological transformations, i.e. for some reason it couldn't break. The follicle remains, continues to grow and turns into a cyst with liquid contents. Usually it does not grow to a large size and resolves on its own, but in rare cases it can reach 10 centimeters or more.
1 Diagnosis of ovarian cyst
2 pelvic ultrasound
3 General blood test
Organic ovarian cysts
An organic ovarian cyst (endometrioid , mucinous , dermoid) is a type of cyst, but in fact it is a tumor-like formation with the potential for malignancy. It is an indication for surgical treatment.
An endometrioid cyst occurs as a result of ovarian endometriosis. Like endometriosis in general, it is an incomprehensible, mysterious disease. Presumably, endometrial cells shed during menstruation attach to the ovary and begin to grow, forming inclusions in the form of cysts of various sizes. Endometrioid ovarian cyst is an indication for surgical treatment, with the exception of recurrent variants with a size of less than 3 cm.
a mucinous cyst is filled with mucin, a mucus-like fluid. It often reaches large sizes (several tens of centimeters) and has several chambers.
dermoid cyst is considered a congenital formation (the process of laying organs and tissues in the womb is disrupted). The contents of this type of cyst are very diverse - the so-called ectoderm rudiments (fat, hair, skin, bones, teeth, etc.). When it reaches a large size, it can manifest itself as pain in the abdomen and lower back, problems with urination and defecation. Ovarian dermoid cysts are prone to inflammation, and torsion of the cyst stalk is possible. Often such cysts are an indication for urgent surgery.
A paraovarian cyst appears from the epididymis; cysts of different sizes are found. The main symptom of such a cyst is transparent and thin walls entwined with blood vessels. Formed between the ages of 20 and 40.
Prevalence of ovarian cysts
According to various authors, the incidence of ovarian tumors among all gynecological diseases ranges from 8 to 19%.
Foreign researchers claim that more than 80% of women of the reproductive period had a history of an ovarian cyst at least once. However, only 1/4 of them had any clinical manifestations.
In postmenopausal women, the incidence of ovarian tumors ranges from 3 to 18%, but it is at this age that they need to pay special attention due to the high risk of malignancy.
Skin cysts
Svetlana Belova, Estonian University of Life Sciences, www.vetderm.eu Photos of the author are used in the article
A cyst is a pathological cavity (in our case in the skin) with a wall lined with epithelium. The contents of the cyst depend on the secretory activity of this epithelium. Cysts can be acquired (for example, blockage of the excretory duct of the skin gland) or congenital.
In the skin, there are cysts of sweat and sebaceous glands, follicular cysts and dermoid cysts/sinuses.
A sweat gland cyst is a small (several millimeters) sized cavity with a bluish tint (photo 1). It is filled with clear liquid (sweat) and protrudes above the skin level. It is relatively rare in both dogs and cats. Single sweat cysts, as a rule, do not cause discomfort and do not require treatment.
Multiple cerumen/ceruminal (modified sweat) gland cysts in the external auditory canal and pinna of cats are a relatively common occurrence and are called ceruminal cystomatosis . While the cysts are small in size (they look like dark gray, almost black smooth elevations a few millimeters in diameter), they do not cause any discomfort (photo 2). However, when they reach a certain size and quantity and block the lumen of the ear canal, they cause external otitis media with secondary infections, soreness and itching (photo 3). Cysts can degenerate into adenomas and adenocarcinomas of the sulfur glands. Treatment consists of surgical excision (preferably laser excision).
Sebaceous gland cysts are small (1–3 mm) elevations of a whitish or yellowish hue (photo 4). They are relatively common, especially in dogs. They do not cause discomfort and do not require treatment.
Follicular cysts (FC) are most often formed by the epithelium of the mouth of the hair follicle and are a cavity filled with dead keratinized epithelium - keratin. FC occurs quite often in dogs (predisposed breeds are German Shepherds, Pekingese, Shih Tzu and Boxers) and rarely in cats. Clinically, FC appears as a rounded raised area of grayish skin ranging from a few mm to 6 cm, often with a hairless and comedonal surface (Figure 5). FC is often mistakenly called a sebaceous gland blockage. They can be single or multiple and have a progressive course. Follicular cysts that have reached significant sizes often have a “pore” on the surface of the skin through which a curdled content (keratin) of a grayish tint is released. When drying, keratin forms a kind of cutaneous horn on the surface of the skin (photo 6). Secondary bacterial infection of the FC is also not uncommon (especially after an attempt to squeeze it out!), in which erythema is noticeable and pain and itching appear (photo 7). Main differential diagnosis: abscesses, tumors. Diagnosis is made based on history, clinical presentation, cytological examination of cyst aspirate (keratin, cholesterol crystals +/- signs of infection) or histology. Treatment consists of surgical excision. Retinoids (isotretinoin 1.5–3 mg/kg/day) may be effective in inhibiting the growth of old cysts in dogs and preventing the formation of new ones.
A dermoid cyst (DC) is a congenital anatomical anomaly in which a fully functioning piece of skin with all appendages (hair follicles, sweat and sebaceous glands) is enclosed in a closed cavity. DC becomes noticeable already in puppyhood, most often on the midline of the head (photo 8). It looks like one or more soft, round or oval-shaped bumps that can be infected and have a “pore” on the surface, from which a tuft of hair often sticks out. Treatment is surgical excision. A dermoid cyst may be connected by a tubular tubule to the spine (dermoid sinus), which naturally creates a risk of bacterial infection of the nervous system. Rhodesian Ridgebacks are especially predisposed to this anomaly, in which the presence of a crest is predetermined by a mutation of certain genes inherited as an autosomal dominant trait and is associated with the formation of dermoid sinuses (photo 9). The diagnosis is made on the basis of anamnesis, examination, contrast radiography, magnetic resonance imaging. Treatment is surgical excision (photo 10).
| Photo 1. Sweat gland cyst | Photo 2. Cysts of sulfur/ceruminal glands |
| Photo 3. Ceruminal cystomatosis | Photo 4. Sebaceous cyst |
| Photo 5. Follicular cyst | Photo 6. Dried keratin on the surface of a follicular cyst |
| Photo 7. Infected follicular cyst | Photo 8. Dermoid cyst (photo by D. Graham published with permission of the author) |
| Photo 9. Rhodesian Ridgeback dermoid sinus fistula at the base of the tail (photo by S. Rüfenacht published with permission of the author) | Photo 10. Surgical excision of the dermoid sinus (photo by S. Rüfenacht published with permission of the author) |
Bibliography
1. Salmon Hillbertz N and Andersson G (2006) Autosomal dominant mutation causing the dorsal ridge predisposes for dermoid sinus in Rhodesian ridgeback dogs. Journal of Small Animal Practice 47: 184–188.
2. Salmon Hillbertz N et al (2007) Duplication of FGF3, FGF4, FGF19 and ORAOV1 causes hair ridge and predisposition to dermoid sinus in Ridgeback dogs. Nature Genetics 39: 1318 – 1320.
3. Kiviranta AM, Lappalainen AK, Hagner K, Jokinen T.. Dermoid sinus and spina bifida in three dogs and a cat. J Small Anim Pract. 2011 Jun;52(6):319-24.
4. Fleming JM, Platt SR, Kent M, Freeman AC, Schatzberg SJ. Cervical dermoid sinus in a cat: case presentation and review of the literature. J Feline Med Surg. 2011 Dec;13(12):992-6.
5. Muller and Kirk's Small Animal Dermatology, 7th Ed. Miller W, Griffin C, Campbell C. WB Saunders, 2012.
6. White A, Stern A, Campbell K, Santoro D.. Multiple (disseminated) follicular cysts in five dogs and one cat. Vet Rec. 2013 Sep 21;173(11):269.
SVM No. 6/2013
Rate material
Like Like Congratulations Sympathy Outrageous Funny Thoughtful No words
Causes
The main reasons for the development of ovarian cysts include processes that lead to a slowdown in the outflow and retention of venous blood in the pelvic organs:
- hormonal disorders;
- inflammatory diseases of the pelvic organs.
The risk of neoplasms increases:
- endocrine pathologies (for example, malfunction of the thyroid gland);
- irregular menstrual cycle;
- obesity;
- taking hormonal medications (for contraception or in preparation for IVF);
- chronic inflammatory diseases of the bladder and intestines;
- smoking;
- abortions;
- some medications prescribed for malignant tumors of the mammary glands;
- congenital abnormalities of tissue development;
- too early onset of menstruation (before 11 years);
- stress;
- surgeries on the reproductive organs.
Also, the risk of developing neoplasms increases in patients who have previously been diagnosed with cysts.