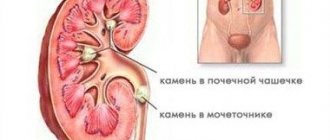
One of the manifestations of urolithiasis is the formation of stones in the bladder. This pathology is accompanied by pain, impaired urination, and blood in the urine. To diagnose the disease, the patient is prescribed an ultrasound examination of the urinary tract, a general urinalysis, cystoscopy, and cystography. Therapeutic measures consist of fragmentation and removal of stones. The contact method (or lithotripsy) or surgical intervention - open cystolithotomy - can be used.
Why do urinary stones form?
The content of the article
Urine usually contains substances that prevent the formation of crystals. If there are few of them or if there is a high concentration of crystalline substances (for example, calcium, oxalate), urinary stones can form.
The formation of urinary stones occurs in the following cases:
- formation of highly concentrated urine (insufficient fluid intake, working in hot conditions);
- with relapse of inflammation of the renal pelvis and bladder;
- misuse of certain medications;
- blocking the flow of urine;
- long-term restriction of physical activity (bedridden patients);
- with genetically determined metabolic disorders.
A combination of several factors may also be diagnosed.
Why do they appear?
The most common reason that contributes to the formation of bladder stones is the presence of bladder outlet obstruction. This is not the name of the disease, but rather a whole list of possible pathologies. Such pathologies sooner or later lead to a violation of the removal of the full volume of urine from the body. As a result, stagnation occurs and urine accumulates. Subsequently, salt crystals form. They are the basis of a future bladder stone.
In addition, there are a number of other reasons that contribute to the formation of stones:
- Diseases of the gastrointestinal tract.
- Trauma, pathology of the skeletal system.
- Inflammatory process in the bladder.
- The connection between the bladder and the central nervous system is damaged. This is called a neurogenic bladder. Occurs with spinal cord injury.
- Constricted urethra. This is also the reason for the excretion of not the full volume of urine.
- The presence of a foreign body in the bladder. For example, there was suture material, a stand, and a catheter left.
- The inner muscular layer is damaged, the mucous membrane protrudes.
- If a woman’s bladder has dropped along with the walls of the vagina. This is called a cystocele.
- Removal of a stone that was located in the kidney through the ureter into the bladder.
- Carrying out surgery to eliminate urinary incontinence. This operation involves tissue transfer.
- If there is a sufficient amount of vitamins and ultraviolet radiation in the body.
- There is an infection that causes the body to lose water.
The formation of stones in the bladder can occur due to impaired metabolism. There are a number of factors that contribute to this. What factors include:
- A person regularly drinks water that contains a lot of salt. Hard water provokes rapid stone formation. People who live in an area with hard tap water must use various methods to soften the water. This could be a filter or a folk method for softening water. Thanks to this, there is a significant reduction in the risk of stone formation in the bladder.
- Poor nutrition. If a person regularly and in large quantities consumes sour, salty, spicy, fried foods, the acidity of the urine increases, resulting in the formation of stones. In addition, it is necessary to eliminate salt from the diet as much as possible and drink enough liquid throughout the day. It is necessary to remember that excluding harmful foods from the daily diet helps to minimize the risk of developing both urolithiasis and any other disease.
- The body does not receive enough fluid. A person drinks little water, urine becomes more concentrated. It liquefies due to a sufficient volume of fluid in the body. Blood viscosity also decreases. In this situation, the body not only gets rid of harmful substances more intensively, but also reduces the likelihood of stone formation. The generally accepted norm for daily fluid intake is two to three liters. This volume may vary depending on the presence of other pathologies of the urinary and cardiovascular systems. Only a qualified specialist can determine the amount of water that needs to be consumed every day.
- Failure to maintain an active lifestyle. Physical activity promotes normal blood circulation in the body. With a sedentary lifestyle, circulation is disrupted, so vital organs and systems receive insufficient amounts of oxygen and other nutrients. Urolithiasis often occurs in bedridden patients. Lack of sufficient physical activity causes disorders in the musculoskeletal system. There is a rapid leaching of calcium from bone tissue. As a result, there is an increase in calcium in the blood, which is excreted by the body in the urine. This means that the formation of stones begins.
- Climate. A hot climate contributes to dehydration. Especially if you don't drink enough liquid. There is an increase in the concentration of salt in the urine, as a result of which stones are formed.
- The kidneys and urinary tract do not work properly. Any injury to this organ leads to urine stagnation. This also causes narrowing of the ureter and upper urinary tract. An infection may also occur. Such a violation should be identified and treated promptly.
- Chronic disease of the digestive and genitourinary system. This happens with pyelonephritis, cystitis, and stomach ulcers. Basically, the presence of any infection can cause metabolic disorders. This means that any inflammation should be treated promptly.
- Bone disease, previous trauma. Osteomyelitis, osteoporosis and other diseases of the skeletal system can cause stones in the bladder. It is necessary to ensure that the musculoskeletal system functions normally.
- Hereditary factors. If a close relative has been diagnosed with urolithiasis, the likelihood of its occurrence increases. The presence of a hereditary predisposition does not guarantee that the disease will appear in any case. If a person follows a healthy diet and leads an active lifestyle, the likelihood of developing bladder stones will be significantly reduced.
- Vitamin deficiency and hypovitaminosis. The formation of stones can occur if vitamin C is present in large quantities in the body. The disease can also develop if there is not enough vitamin A and D.
- If a person suffers from alcoholism or uses excessive amounts of diuretics. Diuretics cause rapid loss of fluid from the body. As a result, the concentration of urine increases and stones form. It must be remembered that the dosage and duration of use of a diuretic drug is determined exclusively by the attending and qualified physician. Self-medication is strictly prohibited.
- Medications. Stones can be caused by ascorbic acid, sulfonamides and other drugs that disrupt metabolic processes.
What are the symptoms of urolithiasis?
In many patients, the presence of urinary stones is discovered incidentally during examination, for example, ultrasound or x-ray.
The most typical and most painful symptom is renal colic. This is severe pain in the side radiating to the groin, sometimes intermittent, often accompanied by nausea and vomiting. If the stone reaches the ureteral junction, the flow of urine may be blocked. If the pathology is bilateral, acute renal failure may occur.
If the stone gets into the bladder, the pain will disappear, but the problem remains in the bladder. A frequent manifestation of stones in the urinary tract mucosa is also the presence of blood in the urine, sometimes visible to the naked eye.
What should be the correct treatment?
Conservative treatment of stones brings good results for small stones. In this case, measures are taken to alkalize the urine. For this purpose, a special diet and medications are prescribed to maintain the desired alkaline balance.
For large stones, minimally invasive surgical interventions are used. The most effective and safe methods for removing bladder stones:
- Transurethral cystolitholapaxy - crushing the stone using ultrasound, laser or other type of energy, and its subsequent removal through a cystoscope.
- Percutaneous suprapubic litholapaxy (treatment method in childhood) – fast and safe stone crushing.
- Open suprapubic cystolithotomy. It is prescribed only for very large stones, if they cannot be crushed by other methods.
Treatment for bladder stones may differ between men and women, as they are sometimes caused by pathologies unique to one sex. In men, these are diseases of the prostate, and in women, often a neurogenic bladder. In this case, it is additionally necessary to treat the underlying disease that caused the stones, otherwise they may form again in the future.
The many causes and possible complications make kidney stones a serious disease that requires prompt medical attention. At the State Urology Center you can make an appointment with a urologist and get to him even on the day of your visit, and if necessary, get emergency help. All services in the clinic are provided within the framework of compulsory medical insurance, so you do not have to worry about the cost of diagnosis and treatment.
On weekdays you can get an appointment with a urologist on the day of your visit
How to diagnose urinary stones?
To better understand the reasons that led to the formation of urinary stones, the urologist asks patients about their eating habits, drinking patterns, medications, previous illnesses and family illnesses.
Stones containing calcium can be detected using a simple x-ray. In other cases, it is necessary to use a contrast X-ray examination method, when a contrast agent is injected into a vein, then the drug is excreted in the urine.
Another common method for visualizing stones is ultrasound of the kidneys and pelvis. It is ideal for assessing the size and location of a stone.
Urine and blood tests can help explain the causes of bladder formation. Such studies are necessarily prescribed to monitor the treatment and prevention of these conditions.
Kidney ultrasound
Urine and blood examination
Diagnostics
- Questioning the patient and laboratory methods: blood test (increased ESR, leukocytosis) and urine (protein, salts).
- Ultrasound is a highly effective, informative, safe and painless method that has no contraindications.
- Cystoscopy is an auxiliary diagnostic method that reveals the degree of dysfunction and destructive changes.
- CT is a highly accurate study that allows you to obtain a three-dimensional image.
- X-ray - identification of shape, size, structure, localization, detection of complications (pyelonephritis, nephrosclerosis, hydronephrosis).
How to treat urinary stones?
As an emergency treatment for renal colic, medications are used to relieve muscle spasms in the urinary tract. Such drugs relieve pain, but also often help spontaneous passage of stones.
Most urinary stones can be treated with increased fluid intake, dietary measures, and medications. With the right approach, 90% of stones will go away naturally within three to six weeks. But it is important for the urologist to obtain the stone in order to conduct a chemical analysis of it.
Some types of stones (eg, urates, cystines) can be dissolved with special substances. Stones that cause a urinary tract infection or block the flow of urine should be removed. Several methods of such treatment are now available.
- Classic operating solution
. Required in less than 5% of cases. In rare cases, the urologist decides to remove the entire kidney. This is usually the case when kidney function is seriously impaired or the stone is the source of a serious infection. - Endoscopic methods
. Many stones can be removed or at least reduced endoscopically. In this case, special instruments are inserted through the urethra and bladder into the ureters. with their help, the stone can be crushed into smaller pieces, which are then removed naturally. - Wave therapy
. Disintegration of urinary stones is possible using the so-called shock wave (extracorporeal shock wave lithotripsy). The high energy waves travel seamlessly through body tissue and water and impact hard surfaces such as urinary stones. Due to the impact, the stones are destroyed. Small stones can be broken up by non-contact lithotripsy.
Operating method
Wave therapy
Endoscopic method
Bladder stones and their endoscopic treatment. Modern view of the problem
Ivanov V.Yu., Malkhasyan V.A., Semenyakin I.V., Pushkar D.Yu.
Bladder stones have caused suffering to people for centuries. Some doctors of ancient times, such as Hippocrates and Ammonius of Alexandria, were able to diagnose and tried to treat bladder stones [1]. The oldest bladder stone studied by scientists belonged to a boy who lived in Ancient Egypt more than 7,000 years ago [2].
Insufficient intake of vitamins A, B6, magnesium, in combination with a low-protein diet, is one of the pathogenetic factors in the formation of stones in the urinary tract [3]. Therefore, the improvement in the quality of nutrition that has occurred in the last century and the use of modern antibacterial therapy has led to a significant decrease in the number of patients with bladder stones in developed countries, where they currently account for about 5% of all stones in the urinary system [4]. These changes also led to the fact that bladder outlet obstruction and urinary infection became the dominant etiological factor in the formation of bladder stones. At the same time, A. Trinchieri et al. in their study demonstrated that changes in socioeconomic factors lead not only to changes in the incidence of urolithiasis, but also cause changes in the physical properties and chemical composition of stones, including those in the bladder [5]. Significant changes in the treatment of patients with bladder stones occurred about 50 years ago in parallel with the development of endourology, and since then the tactics have remained unchanged. Currently, endoscopic removal of bladder stones is the most common treatment option [6]. Clinical manifestations in the presence of bladder stones are well known, but perhaps the changes described above also changed the clinical picture of this disease.
Unfortunately, there are only a few modern studies on this issue, which is undoubtedly due to the sharp decrease in the number of these patients in developed countries. The purpose of our study was to obtain current characteristics of patients suffering from bladder stones, as well as to evaluate the results of endoscopic treatment in a modern urology department.
MATERIALS AND METHODS
Our prospective study included 79 patients who underwent endoscopic removal of bladder stones during 2021 in the urology departments of the University Hospital of Moscow State Medical University. The following information was collected about patients: gender, age, clinical manifestations, intercurrent diseases, body mass index (BMI), radiological data studies on the size and number of stones, the type of surgical interventions associated with lithotripsy, complications of surgical treatment and length of hospitalization.
Ultrasound examination of the bladder and plain urography were used to confirm the presence of a bladder stone and determine its size.
All operations were performed under spinal anesthesia by different surgeons. Endoscopic equipment from Storz and Olimpus was used. When the stone size was up to 1.5 cm, mechanical lithotripsy was mainly used. For larger stones, combined mechanical and laser Ho:Yag lithotripsy with the Lumenis® laser was used.
Statistical data processing was performed in Microsoft Excel®. Descriptive statistics for quantitative data with a symmetric distribution are presented as the arithmetic mean with normal deviation, for data with an asymmetric distribution as a median with an interquartile range. Qualitative data are presented as absolute and relative values. To determine the statistical significance of the data, a confidence interval for the proportion was calculated.
RESULTS
The mean age of the patients was 67.7±11.9 years (min. 28 years, max. 88 years. CI: 65.2-70.4 years). Of the 79 patients, 76 (96.2%, CI: 89.4%-98.7%) were men, three (3.8%, CI: 1.3%-98.7%) were women. Detailed characteristics of the patients included in the study are presented in Table 1.
Table 1. Characteristics of patients included in the study
| Indicators | Quantity (share) | 95% confidence interval |
| Total | 79 | 79 |
| Floor | ||
| Husband. | 76 (96,2%) | 89,4%-98,7% |
| Women's | 3 (3,8%) | 1,3%-10,6% |
| Age | 67,7±11,87 | |
| Duration of the disease | ||
| less than 1 year | 15 (81%) | 11 %-29% |
| more than 1 year | 84 (19%) | 71%-88,1% |
| Etiology | ||
| BPH | 53 (67,1%) | 51,1 %-76,4% |
| Sclerosis ShMP | 7 (8,9%) | 4,4%-17,4% |
| PCa | 6 (7,6%) | 3,5%-15,6% |
| Neurogenic MP | 4 (5,1%) | 2%-12,3% |
| Mesh prosthesis | 3 (3,8%) | 1,3%-10,6% |
| Urethral stricture | 3 (3,8%) | 1,3%-10,6% |
| MP diverticulum | 2 (2,5%) | 0,7%-8,8% |
| Long-term drainage of MP | 1 (1,3%) | 0,2%-6,8% |
| Previous urinary tract surgeries | 27 (34,2%) | 24,7%-45,2% |
| Recurrent MP stones | 10 (12,7%) | 7%-21,8% |
| Maximum stone size, mm | 22,8±9,065 | 19,76-24,4 |
| Multiple stones | 23 (29,1%) | 20,3%-29,9% |
| Availability of cystostomy drainage | 10 (12,7%) | 7%-21,8% |
| Body Mass Index (BMI) | 28,7±5,8 | 27,13-30,28 |
| Accompanying illnesses | ||
| No | 25 (35,2%) | 25,1%-46,8% |
| IHD | 27 (34,2%) | 24,7%-45,2% |
| Hypertonic disease | 33 (41%) | 30,8%-52,1% |
| History of stroke | 2 (2,5%) | 0,07%-8,8% |
| Heart failure | 8 (10,1%) | 5,2%-18,7% |
| Heart rhythm disturbance | 6 (7,6%) | 3,5%-15,6% |
| History of ICD | 10 (12,7%) | 7%-21,8% |
| Alzheimer's disease | 1 (1,3%) | 0,2%-6,8% |
| Stomach ulcer | 2 (2,5%) | 0,7%-8,8% |
The most common complaints were: frequent urination in 51 (64.6%, CI: 53.6%-74.2%) patients, difficulty urinating in 49 (62%, CI: 51%-71.9), painful urination was noted 39 (40.5%, CI: 30.4%-51.5%), hematuria was observed in 30 (38%, CI: 28.1%-49%). The duration of complaints for more than a year was noted in 64 patients (81%, CI: 71%-88.1%). Details of the clinical manifestations of the disease in patients included in the study are shown in Table 2.
Table 2. Clinical symptoms in patients with bladder stones included in the study
| Indicators | Quantity (share) | 95% confidence interval |
| Difficulty urinating | 49 (62%) | 51%-71,9% |
| Painful urination | 39 (40,5%) | 30,4%-51,5% |
| Frequent urination | 51 (64,6%) | 53,6-74,2 |
| Feeling of incomplete emptying of bladder | 11 (13,9%) | 8%-23,2% |
| Weakening of the urine stream | 12 (15,2%) | 8,9%-24,7% |
| Urgency | 3 (3,8%) | 1,3%-10,6% |
| Urinary incontinence | 1 (1,3%) | 0,2%-6,8% |
| Hematuria | 30 (38%) | 28,1%-49% |
Ten patients (12.7%, CI: 7%-21.8%) had previously undergone cystostomy. 27 patients (34.2%, CI: 24.7%-45.2%) had previously undergone surgery on the upper urinary tract, and 10 (12.7%, CI: 7%-21.8%) patients had previously A stone has already been removed from the bladder. 23 (29.1%, CI: 20.3%-29.9%) were diagnosed with multiple bladder stones. The mean stone size was 22.8±9.07 mm (min: 5 mm, max: 45 mm CI: 19.76-24.4).
The etiological causes of bladder stone formation were: in 53 patients (67.1%, CI: 51.1%-76.4%) - benign prostatic hyperplasia (BPH), in 7 (8.9%, CI: 4. 4%-17.4%) - sclerosis of the bladder neck, 6 (7.6%, CI: 3.5%-15.6%) - prostate cancer, 4 patients (5.1%, CI: 2%-12.3%) neurogenic bladder, 3 (3.8%, CI: 1.3%-10.6%) - urethral stricture, 2 (2.5%, CI: 0.7% -8.8%) — bladder diverticulum, in 1 patient (1.3% CI: 0.2%-6.8%) the cause was prolonged drainage of the bladder. In all three women (3.8%, CI: 1.3%-10.6%) included in the study, the cause of stone formation was protrusion of a mesh prosthesis into the bladder after undergoing pelvic floor surgery.
Only 25 patients (35%, CI: 25.1%-46.8%) had no significant concomitant diseases, 21 patients (26.6%, CI 18.1%-37.2%) had two or more concomitant diseases diseases. The most common comorbidity was hypertension, which was noted in 32 (41%, CI: 30.8%-52.1%) patients. The average BMI was 28.7±5.8 mm. (CI: 27.13-30.28 mm).
In addition to cystolithotripsy (CLT), 52 (65.8%, CI: 54.75%-75.3%) patients underwent transurethral resection of the prostate (TURP), 18 patients (22.8%, CI: 14.9% -33.2%) no additional interventions were performed, and only CLT was performed due to the fact that no anatomical changes were identified that could lead to stone formation. 4 patients (5.1%, CI: 2%-12.3%) underwent transurethral resection of the bladder neck, and two (2.5%, CI: 0.7%-8.8%) underwent internal optical urethrotomy . The average operation time was 67.7±31.77 minutes. (min. - 20, max. - 160 min., mode - 60 min., CI: 57.8-73.6). The majority of patients - 66 people (83.5%, CI: 73.9%-90.1%) - had no intraoperative or postoperative complications. The most common complication was conversion and cystolithostomy, which was performed in 5 patients (6.3%, CI: 2.7%-14%). Detailed characteristics of complications are presented in Table 3. Our Spearman correlation analysis did not reveal a relationship between the probability of conversion and the patient’s age (p = 0.29), patient’s BMI (p = 0.648), but a positive correlation was identified with the size of the stone (p = 0.039 ). According to the Clavien classification of surgical complications, 6 (7.6%, CI: 3.5%-15.6%) patients had grade IIIb complications, 5 (6.3%, CI: 2.7%-14% ) - grade IVa, one (1.3%, CI 0.02%-6.8%) - grade II.
Table 3. Type and complications of surgical intervention in patients included in the study
| Type of operation | Quantity(share) | 95% confidence interval |
| VOUT + CLT | 2 (2,5%) | 0,7%-8,8% |
| TURP+CTL | 52 (65,8%) | 54,75%-75,3% |
| TURSHMP+TSLT | 4 (5,1%) | 2,0%-12,3% |
| TURUSHA + CLT | 2 (2,5%) | 0,7%-8,8% |
| TURMP + CLT | 1 (1,3%) | 0,2%-6,8% |
| CLT | 18 (22,8%) | 14,9%-33,2% |
| Operation duration | 67,7+-31,77 | 57,8-73,6 |
| Complications of the operation | ||
| OZM | 1 (1,3%) | 0,2%-6,8% |
| OKS | 2 (2,5%) | 0,7%-8,8% |
| TUR syndrome | 1 (1,3%) | 0,2%-6,8% |
| Delirium | 1 (1,3%) | 0,2%-6,8% |
| Conversion | 5 (6,3%) | 2,7%-14% |
| Arrhythmia | 1 (1,3%) | 0,2%-6,8% |
| MP perforation | 1 (1,3%) | 0,2%-6,8% |
| No | 66 (83,5%) | 73,9%-90,1% |
The median length of hospitalization was 7 days (interquartile range 2–9 days).
DISCUSSION
In adult patients, bladder stones rarely occur spontaneously and are mainly caused by predisposing factors such as bladder outlet obstruction, urinary tract infection, and a foreign body in the bladder lumen [4]. It follows that the primary etiological cause must be identified and eliminated to avoid relapse. In men, diseases such as BPH, urethral stricture, bladder diverticulum, and neurogenic bladder are associated with the formation of bladder stones.
According to R. Douenias et al. bladder outlet obstruction may be the cause of the formation of more than 75% of bladder stones [7], which, according to classical recommendations, dictates mandatory surgical treatment of BPH in the presence of bladder stones. In our study, the most common etiological factor was BPH, which was detected in 67% of patients, and the most common operation associated with lithotripsy was TURP, which was performed in 65.8% of patients. A number of studies question the role of bladder outlet obstruction as the sole factor in the formation of bladder stones. So in the work of F. Millan-Rodriguez et al. In 18% of patients with bladder stones, no abnormalities were detected during urodynamic examination [8]. Indirect confirmation of the lack of influence of bladder outlet obstruction on the development of bladder stones is the fact that only 1-2% of patients with BPH have bladder stones [7]. For example, in a study by WK Mebust et al. It was noted that out of 3885 patients who underwent transurethral resection of the prostate gland, only 3% had indications for a combined operation aimed at getting rid of bladder stones [9]. Our study confirms the fact that bladder outlet obstruction is not the only cause of bladder stone formation. In 18 (22.8%) patients included in the study, no anatomical reason for the formation of bladder stones was identified intraoperatively and they underwent only cystolithotripsy.
Probably, the formation of bladder stones occurs due to a combination of factors of bladder outlet obstruction and dysmetabolic disorders. However, in the study by WM Li et al. demonstrates the superior influence of local factors of stone formation over systemic ones in patients with bladder stones. This study analyzed groups of patients with uric acid stones located in the upper urinary tract and bladder. Thus, in the group of patients with stones localized in the bladder, there was a lower level of creatinine and uric acid in the blood plasma and a higher incidence of bladder outlet obstruction compared to patients with stones localized in the upper urinary tract [10].
Patients with a neurogenic bladder are at high risk of developing bladder stones. Thus, according to JH Ku et al., bladder stones were detected in 28% of patients with spinal cord injuries [11]. In our study, neurogenic bladder was the cause of bladder stones in 4 patients (5.1%).
Prolonged drainage of the bladder is also a factor in the formation of bladder stones. In a study by A.A. Khan et al. An analysis of the results of long-term bladder drainage in 260 patients was performed. In 147 (55.5%) of them, signs of drainage encrustation were detected and these patients underwent fibrocystoscopy, during which bladder stones were identified in 66 patients (45%) [12]. Also in the study by J. Ord et al. When observing 457 patients with neurogenic bladder, it was noted that the risk of developing bladder stones in the presence of long-term bladder drainage was 4%, and only 0.2% with intermittent catheterization; the authors found no difference in the incidence of bladder stones in patients with an indwelling urethral catheter and suprapubic cystostomy drainage [13]. In our study, the presence of cystostomy drainage was noted in 10 (12.7%) patients, and in one patient, long-term bladder drainage with a permanent urethral catheter was the leading etiological factor.
An important etiological factor in the formation of bladder stones is urinary tract infection. An increase in urine pH promotes the aggregation of magnesium ammonium phosphate and apatite carbonate crystals. A number of studies link the formation of urinary stones with infection of the urinary tract by urease-producing microorganisms [14,15]. Indirect confirmation of the importance of the infectious process in the formation of bladder stones in our study is the fact that 32.4% of patients had previously undergone surgical interventions on the urinary tract, and 12.7% had recurrent bladder stones.
In women, bladder stones are mainly of a secondary nature and can be caused by pelvic organ prolapse, neurogenic bladder dysfunction, or the presence of a foreign body in the bladder. Recently, the number of operations using mesh synthetic prostheses for urinary incontinence and pelvic organ prolapse has increased significantly. Protrusion of the mesh prosthesis into the bladder is one of the complications of these operations. In a study by I. Levin et al. It was noted that the frequency of intravesical protrusion of a synthetic loop after TVT surgery is 5.1% [16]. The presence of synthetic material in the lumen of the bladder can lead to encrustation and the formation of bladder stones. There are a small number of publications devoted to this issue, presented mainly by descriptions of clinical cases. M. Blewniewski et al. describe protrusion of the mesh prosthesis and the formation of bladder stones after TVT surgery in 6 patients. The patients underwent successful laser lithotripsy and simultaneous extraction of the cystic fragment of the synthetic loop, but the authors do not reflect the results of follow-up of these patients [17]. In our study, in all three women with bladder stones, the etiological factor was protrusion of the mesh prosthesis. The patients also underwent laser cystolithotripsy and transurethral removal of an implant fragment. However, our experience shows that all these women subsequently underwent repeated interventions associated with recurrent protrusion or recurrent stone formation. Therefore, the problem of such bladder stones is very relevant and requires detailed research.
One of the etiological reasons for the formation of bladder stones is the migration of stones from the upper urinary tract. Thus, in a study by FT Hammad et al. 33% of patients with bladder stones had anamnestic indications of renal colic [18]. In our study, only 12.7% of patients had anamnestic indications of the presence of stones in the upper urinary tract, so this factor is not significant in patients living in Moscow.
A typical symptom in the presence of bladder stones is frequent and painful urination, which can occur in 40-50% of patients. 30-40% of patients may experience intermittent urination [19]. One of the characteristic symptoms is terminal hematuria. According to research by V.A. Malkhasyan et al., performed in 2021, bladder stones were diagnosed in 3.7% of patients who sought hospital care in Moscow for hematuria [20]. In our study, hematuria was noted in 30% of patients, and the most common complaints were frequent and difficulty urinating, which were noted in 51% and 49% of patients, respectively.
It is believed that the decrease in the number of patients with bladder stones in developed countries is associated not only with changes in the quality of nutrition, but also with increased patient awareness, availability of medical care and early treatment of bladder outlet obstruction that has occurred. However, our study revealed that in the majority of patients (81%) the duration of the disease was more than one year. This circumstance may indicate inadequate monitoring of patients with chronic bladder outlet obstruction and insufficient regularity of examinations in these patients. Insufficient effective monitoring of patients with bladder outlet obstruction is indicated by the fact that out of 589 patients who underwent TURP in our clinic during the specified period, 52 had bladder stones (8.8% CI 6.7%-11. 4%) of patients, while according to a multicenter European study, only 3% of patients who underwent TURP had bladder stones [9].
There are many methods of surgical treatment of bladder stones, including extracorporeal shock wave lithotripsy, transurethral and percutaneous cystolithotripsy and cystolithotomy. Each method has its own advantages and disadvantages. The choice of surgical treatment method is determined by the availability of equipment, the qualifications of the surgeon, the condition of the patients (age, comorbid status), and the characteristics of the stone (size and density)[21]. Clinical guidelines of the European Association of Urology consider the presence of bladder stones as an absolute indication for surgical treatment of BPH [22]. Currently, the most common surgery for BPH is TURP [23]. Therefore, transurethral access to a bladder stone is the most attractive and is the most common in our time, as it allows not only to rid the patient of the stone, but also to simultaneously eliminate the cause of bladder outlet obstruction. We did not find any literature indicating the effectiveness and incidence of complications when performing combined TURP and cystolithotripsy. But according to O. Reich et al. the rate of complications with TURP is about 11% [23]. According to the results of S. Mandal et al. the bulk of complications (90%) belonged to groups I, II and III according to the Clavien classification [24]. A number of studies indicate that the incidence of complications with cystolithotripsy ranges from 9-25% [25,26]. In our study, 11 (13.9%) patients had complications III and IV according to the Clavien classification. The most common complication was the need for conversion and cystolithostomy. We confirmed the relationship between the size of the stone and the likelihood of conversion.
Currently, several methods have been proposed that increase the effectiveness of cystolithotripsy - the use of a nephroscope passed into the bladder both transurethrally and through percutaneous access. The use of a nephroscope allows the use of an ultrasonic and pneumatic lithotripter and the removal of large fragments of stones through the nephroscope tube using forceps. So in the study by K. Ener et al. with transurethral use of a nephroscope, the average operation time was 48.2±13.2 minutes, and when performing standard cystolithotripsy through a cystoscope, 68.1±22.7 minutes [27]. In a study by A. Bansal et al. demonstrates that cystolithotripsy performed transurethrally with a nephroscope has an advantage in terms of time spent on surgery compared to standard cystolithotripsy and when using a nephroscope through a percutaneous approach. Upon further observation, the formation of urethral stricture was noted in 3.2% of patients who underwent standard cystolithotripsy, in 7.8% of patients who underwent transurethral cystolithotripsy using a nephroscope, and in patients who underwent percutaneous cystolithotripsy, the development of urethral stricture was not observed [28]. Our clinic has experience in performing similar operations for large bladder stones, but we did not include these operations in this analysis, since they are the subject of our subsequent studies.
CONCLUSION
Bladder stones remain a pressing problem in modern urology. Our study did not reveal significant differences in the socio-demographic and clinical characteristics of patients compared to data published in the world press over the past 30 years. The leading etiological factor of stone formation is infravesical obstruction. However, we noted an almost threefold increase in the proportion of patients with bladder stones operated on for BPH compared with data from a multicenter European study. This fact, along with the fact that most patients were operated on more than a year after the appearance of characteristic complaints, indicates the insufficient effectiveness of outpatient monitoring of patients with bladder outlet obstruction.
Transurethral cystolithotripsy remains the main treatment method for bladder stones with proven high efficacy and safety.
Our analysis reveals a number of important questions that require further research to answer. These issues include the development of bladder stones and their treatment tactics in patients who have undergone pelvic floor plastic surgery using mesh implants; a relatively high incidence of recurrent bladder stones and a higher incidence of patients with bladder stones who had previously undergone urinary tract interventions. Our study suggests that patients with bladder outlet obstruction who have previously undergone urinary tract surgery and have a history of stones in the upper urinary tract are at risk for the formation of bladder stones. Careful outpatient monitoring of these patients will allow for a timely diagnosis and provide them with medical care as soon as possible.
LITERATURE
1. Shelley HS. Cutting for the stone. J Hist Med Allied Sci 1958;13(1):50-67.
2. Riches E. The history of lithotomy and lithotrity Ann R Coll Surg Engl 1968; 43(4):185-199.
3. Ali SH, Rifat UN. Etiological and clinical patterns of childhood urolithiasis in Iraq. Pediatr Nephrol 2005;20(10):1453-1457. doi:10.1007/s00467-005-1971-0.
4. Schwartz BF, Stoller ML. The vesical calculus. Urol Clin North Am 2000;27(2):333-346.
5. Trinchieri A. Epidemiology of urolithiasis. Arch Ital di Urol Androl Organo Uff 1996;68(4):203-249.
6. Papatsoris AG, Varkarakis I, Dellis A, Deliveliotis C. Bladder lithiasis: from open surgery to lithotripsy. Urol Res 2006; 34(3):163-167. doi:10.1007/s00240-006-0045-5.
7. Douenias R, Rich M, Badlani G, Mazor D, Smith A. Predisposing factors in bladder calculi: review of 100 cases. Urology. 1991;37, (3):240-243. doi: 10.1016/0090-4295(91)80293-G.
8. Millan-Rodriguez F, Errando-Smet C, Rousaud-Baron F, Izquierdo-Latorre F, Rousaud-Baron A, Villavicencio-Mavrich H. Urodynamic findings before and after noninvasive management of bladder calculi. BJU Int 2004;93(9):1267-1270. doi: 10.1111/j.1464-410X.2004.04815.x.
9. Mebust WK, Holtgrewe HL, Cockett ATK, Peters PC. Transurethral prostatectomy: immediate and postoperative complications. a cooperative study of 13 participating institutions evaluating 3,885 patients. 1989. J Urol 2002;167(2 Pt 2):999-1003.
10. Li WM, Chou YH, Li CC, Liu CC, Huang SP, Wu WJ, et al. Local factors compared with systemic factors in the formation of bladder uric acid stones. Urol Int 2009;82(1): 48-52. doi: 10.1159/000176025.
11. Ku JH, Jung TY, Lee JK, Park WH, Shim HB. Risk factors for urinary stone formation in men with spinal cord injury: a 17-year follow-up study. BJU Int 2006;97(4):790-793. doi: 10.1111/j. 1464-410X.2006.0 5991.x.
12. Khan AA, Mathur S, Feneley R, Timoney AG. Developing a strategy to reduce the high morbidity of patients with long-term urinary catheters: the BioMed catheter research clinic. BJU Int 2007;100(6):1298-1301. doi: 10.1111/j. 1464-410X.2007.07146.x.
13. Ord J, Lunn D, Reynard J. Bladder management and risk of bladder stone formation in spinal cord injured patients. J Urol 2003;170(5):1734-1737. doi: 10.1097/01.ju.0000091780.59573.fa.
14. Schaffer JN, Norsworthy AN, Sun TT, Pearson MM. Proteus mirabilis fimbriae- and urease-dependent clusters assemble in an extracellular niche to initiate bladder stone formation. Proc Natl Acad Sci 2016;113(16):4494-4499. doi: 10.1073/pnas.1601720113.
15. Satoh M, Munakata K, Kitoh K, Takeuchi H, Yoshida O. A newly designed model for infection-induced bladder stone formation in the rat. J Urol 1984;132(6):1247-1249.
16. Levin I, Groutz A, Gold R, Pauzner D, Lessing JB, Gordon D. Surgical complications and medium-term outcome results of tension-free vaginal tape: A prospective study of 313 consecutive patients. Neurourol Urodyn 2004;23(1):7-9. doi: 10.1002/nau.10164. 17. Blewniewski M, Markowski M, Klis R, Rozanski W. Cystolithiasis in women as a distant complication after minimal invasive treatment of stress urinary incontinence. Cent Eur J Urol 2014;67(3):277-281. doi: 10.5173/ceju.2014.03.art13.
18. Hammad FT, Kaya M, Kazim E. Bladder calculi: did the clinical picture change? Urology 2006;67(6):1154-1158. doi: 10.1016/j.urology.2005.12.038.
19. Menon M, Resnick MI. Urinary lithiasis: etiology, diagnosis, and medical management. In: Walsh PC, Retik AB, Vaughan ED, Wein AJ (eds) Campbell's urology. 8th edition. WB Saunders, Philadelphia, 2002. p. 3229.
20. Malkhasyan VA, Ivanov VYU, Khodyreva LA, Dudareva AA, Kupriyanov YuA, Redkovich VI, et al. Analysis of the provision of specialized medical care to patients with gross hematuria in urological hospitals in Moscow. Experimental and Clinical Urology 2016;(4):10-16.
21. Philippou P, Moraitis K, Masood J, Junaid I, Buchholz N. The management of bladder lithiasis in the modern era of endourology. Urology 2012;79(5):980-986. doi: 10.1016/j. urology.2011.09.014.
22. Oelke M, Bachmann A, Descazeaud A, Emberton M, Gravas S, Michel MC, et al. EAU Guidelines on the treatment and follow-up of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. Euro Urol 2013; 64(1):118-140. doi: 10.1016/j.eururo.2013.03.004.
23. Reich O, Gratzke C, Bachmann A, Seitz M, Schlenker B, Hermanek P, et al. Morbidity, mortality and early outcome of transurethral resection of the prostate: a prospective multicenter evaluation of 10,654 patients. J Urol 2008;180(1):246-249. doi: 10.1016/j.juro.2008.03.058.
24. Mandal S, Sankhwar SN, Kathpalia R, Singh MK, Kumar M, Goel A, et al. Grading complications after transurethral resection of prostate using modified Clavien classification system and predicting complications using the Charlson comorbidity index. Int Urol Nephrol 2013;45(2):347-354. doi:10.1007/s11255-013-0399-x.
25. Bhatia V, Biyani CS. Vesical lithiasis: open surgery versus cystolithotripsy versus extracor-poreal shock wave therapy. J Urol 1994;151(3):660-662.
26. Razvi HA, Song TY, Denstedt JD. Management of vesical calculi: comparison of lithotripsy devices. J Endourol 1996;10(6):559-563. doi: 10.1089/end.1996.10.559.
27. Ener K, Agras K, Aldemir M, Okulu E, Kayigil O. The randomized comparison of two different endoscopic techniques in the management of large bladder stones: transurethral use of nephroscope or cystoscope? J Endourol 2009;23(7):1151-1155. doi: 10.1089/end.2008.0647.
28. Bansal A, Kumar M, Sankhwar S, Goel S, Patodia M, Aeron R, et al. Prospective randomized comparison of three endoscopic modalities used in treatment of bladder stones. Riv Urol 2016;83(2):87-92. doi: 10.5301/uro.5000171
The article was published in the journal Experimental and Clinical Urology. Issue No. 3/2017 - pp. 44-50
Magazine
Journal "Experimental and Clinical Urology" Issue No. 3, 2017
Comments
Guest — 01/03/2018 — 02:08:07
My husband is 90 years old. At the age of 80, he was diagnosed with BPH and was prescribed alpha-blockers. He did not tolerate them well. After 5 years, stones were found in the bladder. The urologist (Kineshma) said that live with these stones; he reacted negatively to my persuasion to do lithotripsy or even surgery. She prescribed him cystinal, uralite U, cystone, phytolysin. ,magurlit. With this treatment, the stones only increased in size and only Rovatinex began to drive the stones away. In December, from 14 to 30, I was in the cardiac center of the Regional Hospital in the city of Ivanovo with a diagnosis of SSSU. An electrical pacemaker was implanted with a heart rate of 70 per minute. He was examined by a urologist, who recommended that in case of urinary retention, contact a urologist in Kineshma for a cystolithotomy with cystostomy. There is no need for hospitalization in the urology department of the Regional Clinical Hospital. Is this a way out? My husband is a WWII veteran, Art 17, and has been disabled for 2 years due to a general illness since July 2021. What do you recommend and what is the best way out of this situation?
Shaderkina Victoria Anatolyevna - 01/17/2018 - 15:45:01
Dear Nina Georgievna! Contact and ask your question on our advisory portal Nethealth.ru.
Kokorev Valery Serafimovich - 12/24/2017 - 23:19:08
Thanks for posting! One question: is it possible to remove a 0.9 mm bladder stone using a litholysis agent such as Cyston? Or is surgical removal necessary? Sincerely, Kokorev V.S.
To post comments you must log in or register
How to prevent the formation of urinary stones?
Once a urinary stone has formed at least once, there is a high probability that the situation will recur if precautions are not taken.
The simplest measure is adequate drinking regimen. Fluid intake should be maintained at 2-3 liters per day.
Drinking regime
If the cause and chemical composition of the stone can be determined, there are other special dietary measures and medications that can significantly reduce the risk of stone formation. In many cases, the cause of urinary tract stones cannot be determined.
If patients experience relapses, they should be regularly evaluated by a urologist or nephrologist, at least once a year.
ONLINE REGISTRATION at the DIANA clinic
You can sign up by calling the toll-free phone number 8-800-707-15-60 or filling out the contact form. In this case, we will contact you ourselves.
If you find an error, please select a piece of text and press Ctrl+Enter
How are stones classified?
The stones differ from each other, given their chemical composition.
- Oxalates. This stone contains calcium salts of oxalic acid. They are distinguished by their dense structure, dark color, and spiky, uneven surface.
- Phosphates. Such stones consist of calcium salts of phosphoric acid. They have a soft and crumbly consistency. Their surface is smooth and slightly rough, the color is white-gray. They are characterized by intensive growth, especially if there is an infection in the body.
- Urats. These crystals of uric acid salts are distinguished by a dense structure, light yellow or brick color, and a smooth or finely dotted surface.
- Carbonates. The formation of such stones occurs when calcium salts of carbonic acid settle. They have a soft structure, light shade, smooth surface. Can be of various shapes.
- Cystine. They consist of the sulfur compound of the amino acid cysteine. Such stones are distinguished by their soft consistency, smooth surface, round shape, and white-yellow color.
- Cholesterol. They can be found quite rarely. These stones contain cholesterol. They are distinguished by a soft crumbly consistency and black color.
In some cases, the stone may be not homogeneous, but mixed.
Prevention
Prevention is necessary to prevent recurrence of stone formation. Basic Rules:
Factors contributing to stone formation
1. Consumption of foods rich in stone-forming substances
2. Diseases and conditions associated with stone formation
- Hyperparathyroidism
- Renal tubular acidosis
- Jejunoileal anastomosis
- Crohn's disease
- Condition after ileal resection
- Malabsorption syndrome
- Sarcoidosis
- Hyperthyroidism
3. Family history of urolithiasis
4. Drugs associated with stone formation
5. Anomalies in the structure of the urinary system associated with stone formation
- Tubular ectasia
- LMS stricture
- Diverticulum/calyx cyst
- Ureteral stricture
- Horseshoe kidney
- Urinary tract infections
Causes
All causes leading to the formation of stones in the urinary system are divided into exogenous (external) and endogenous (internal).
The following can be classified as exogenous:
- prolonged drinking of hard water;
- living in climatic zones where there is a lack of ultraviolet rays;
- large consumption of sour, salty, spicy foods;
- not drinking enough water during the day;
- sedentary lifestyle.
The endogenous ones include the following:
- impaired renal function as a result of chronic diseases;
- genetic predisposition to stone formation;
- infectious diseases accompanied by dehydration;
- severe diseases in which the patient requires long-term immobilization;
- pathology of the gastrointestinal tract (due to disruption of the processes of digestion and absorption);
- metabolic disorders (hyperparathyroidism, gout);
- congenital anomalies of the structure of the kidneys and urinary tract.
Most often with urolithiasis, inflammatory kidney diseases (pyelonephritis, glomerulonephritis), gout, hyperparathyroidism, cholelithiasis, cystitis, prostatitis, pancreatitis, colitis are present.
There are 5 types of stones:
- urate, appear in cases of uric acid metabolism disorders (gout);
- oxalate, appear with an increased content of oxalate salts;
- phosphate, appear due to disturbances in phosphorus metabolism;
- cystine, they appear in hereditary pathologies;
- mixed, a combination of several types of metabolic disorders.
Diet
More information about the diet for kidney stones is written in our separate article.
For patients with urolithiasis, it is recommended to follow the following dietary recommendations:
Be sure to drink about two liters of liquid during the day;
For urate stones, it is necessary to limit:
- meat; fish;
- mushrooms;
- legumes;
- beer.
For oxalate stones:
- chocolate, cocoa;
- beets, lettuce, spinach;
- foods rich in oxalic acid;
For phosphate stones:
- salt;
- carbonated drinks;
- alcohol;
- currants, cranberries;
- dairy products.