Every 3rd patient who comes to a rheumatologist with a complaint of joint inflammation, according to statistics, suffers from infectious arthritis. This disease requires immediate consultation with a doctor, because it can completely and irreversibly destroy a joint in a couple of days, and every 12th of those who are unlucky enough to get the disease die every year from its complications. But if you go to the hospital in a timely manner, 70% of patients get off with a “mild fright” - modern medicine allows you to save joints from deformation in most cases.
Let's look at the symptoms and treatment of infectious arthritis.
Infectious arthritis - what is it?
Infectious arthritis is characterized by an inflammatory process occurring inside the joint. This may be caused by bacteria, viruses, parasites or fungi.
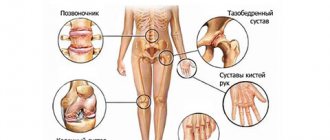
This type of arthritis can affect absolutely any joint.
. A characteristic feature of the disease is that in addition to local manifestations (swelling, pain and joint immobility), there are also general symptoms (fever, chills, signs of intoxication).
Infectious arthritis refers to a group of diseases caused by various types of infectious agents that penetrate specifically into the structure of the tissues that form the joint.
According to existing statistics in the field of rheumatology and traumatology, arthritis of this type is diagnosed in every third patient.
The most common site of infectious arthritis is the joints of the upper and lower extremities
.
Classification
The origin and symptoms of infectious arthritis of different clinical forms have both similarities and differences. Let's look at the most common forms.
Acute purulent
Acute purulent arthritis of the knee joint
This form of the disease develops when a pyogenic infection (Pseudomonas aeruginosa, staphylococci, streptococci, etc.) gets into the joint. Infection can be primary in wounds and secondary - when infection spreads from surrounding tissues or distant foci of infection. People suffering from rheumatoid arthritis, especially women, are at risk.
The disease begins acutely and progresses severely. Fever, headache, chills appear. The affected joint swells and the skin over it turns red. The pain is so severe that the patient cannot move the limb and tries to give it a position that causes the least pain.
Without timely assistance, the articular surfaces quickly collapse, limiting the mobility of the limb. With adequate treatment, complete recovery occurs.
Septic
It develops against the background of already existing sepsis - a generalized infectious process. The infection enters the joint cavity through the hematogenous route - through the bloodstream. The disease can occur in the form of:
- bacterial-metastatic form with symptoms of acute purulent arthritis
- the patient’s condition can be extremely severe; the prognosis of the disease depends on timely treatment; - toxic-allergic form
- the course is not always acute, often occurs subacutely with multiple lesions of the joints of a migrating (alternating) nature; the process is non-purulent in nature and ends with recovery against the background of cure of sepsis.
Tuberculous
Arthritis in this case also occurs in the form of bacterial-metastatic and toxic-allergic forms. In the first case, the spine and large joints of the limbs are mainly affected, and the disease is called osteoarticular tuberculosis. It initially proceeds chronically with increasing pain during movement and general malaise. The main changes are visible on x-rays in the form of damage to the joint bone tissue from the appearance of a spot with loss of calcium in the bone to bone destruction. If left untreated, it leads to disability.
The toxic-allergic form, first described by Ponce at the beginning of the 20th century, is very similar to rheumatoid arthritis with a chronic onset and damage to the small joints of the hands and feet. Their destruction and disability are also possible. Damage to large joints sometimes occurs without consequences and resolves with anti-tuberculosis therapy.
Chondroprotectors: what are they, how to choose, how effective are they?
Joint pain at rest
Gonorrheal
Damage to joints by gonococcal infection can have bacterial-metastatic and toxic-allergic forms. In both cases, large joints are affected, most often one knee (ankle, wrist). The disease is acute, with high fever, intoxication and severe joint pain. The knee swells, turns red, and is impossible to touch because of the pain.
With timely treatment, the disease has a favorable outcome. If left untreated, complete immobility of the limb quickly sets in.
Borreliosis
Borreliosis or Lyme disease is an infection caused by spiral-shaped bacteria called Borrelia spirochetes. It is transmitted by ticks and occurs in a succession of stages:
- 1-2 weeks after a tick bite, an increase in body temperature, intoxication, muscle stiffness and the appearance of redness on the body at the site of the tick bite - erythema, surrounded by concentric rings, spreading to large areas of the body. With timely administration of antibacterial therapy, the disease can end at this stage.
- It develops 1–3 months after the onset of the disease and manifests itself in the form of lesions of the nervous system (meningitis, neuritis with acute pain) and the heart (heart block, myocarditis, etc.).
- Joint damage begins six months (sometimes 2 years) after the onset of the disease in genetically predisposed people and occurs in the form of severe joint pain, a benign recurrent inflammatory process that occurs as an infectious-allergic arthritis with asymmetric damage to 1 - 2 joints (most often the knee) and ending after a few years with recovery in most patients. But in some patients the disease can become chronic with gradual impairment of limb function.
The initial stage of borreliosis is erythema migrans and stage 3 is chronic arthritis of the knee
Viral
Develops against the background of various viral diseases:
- Parvovirus infection caused by parvovirus B19
- the disease occurs with intoxication, fever, skin manifestations in the form of red spots, papules raised above the skin and pinpoint subcutaneous hemorrhages. At the same time, symmetrical damage to the joints occurs. Small joints of the hand, wrist, elbow, knee, and ankle joints may be involved. Symptoms are similar to rheumatoid lesions, but last from 3 months to a year and have a favorable outcome. - Rubella
– arthritis develops more often in adult women against the background of existing symptoms of rubella or before their appearance. Such lesions are rare in children. The periarticular tissues swell, turn red, and severe pain appears, disrupting joint function. The lesion is asymmetrical with the involvement of small joints of the hand, wrist, knee, and elbow joints. Arthritis lasts two to three weeks, after which complete recovery occurs. - Viral hepatitis B and C
- arthritis develops quite often, but has a benign course and ends with complete recovery. Small joints of the hand, elbows, ankles and, less commonly, other joints are affected. Inflammation in the joints usually begins before the appearance of jaundice and ends during its peak.
Causes of infectious arthritis
The most likely cause of infectious arthritis is the metastatic route of joint damage, which involves direct penetration of infection into the joint tissue through the blood or lymph.
Another route of infection can be injury or an open wound, as well as the spread of pathogens from nearby foci of another disease, for example, osteomyelitis.
Arthritis caused by infectious pathogens in childhood is usually provoked by staphylococcus, enterobacteria or Haemophilus influenzae. However, at the same time, other arthritis, quite specific for this age category, may occur, caused by tuberculosis, gonorrhea or syphilis.
Fungal
Most often, fungal infections of the joints develop with actinomycosis, but they also occur with other fungal infections. Pathogenic fungi enter the joint cavity from a nearby bone lesion or from distant lesions (carious teeth) through the bloodstream. The course is chronic, with relapses and the possible addition of a bacterial infection. Very often, fistulas occur - passages through which pus from the joint is released onto the surface of the skin. In the absence of adequate treatment, it leads to a gradual loss of joint function.
Parasitic
The cause of arthritis is usually echinococcosis, which affects the bone tissue of the vertebrae, pelvic bones and long bones of the limbs. A toxic-allergic inflammatory process usually develops in the joints. The joints of the spine, hips, knees and elbows are often involved. The course is benign, but is accompanied by severe joint pain. Recovery occurs when complete treatment of echinococcosis is prescribed.
Infectious-allergic arthritis
Infectious-allergic arthritis occurs when there is an allergy, against the background of which an inflammatory process in the joints develops under unfavorable conditions. The disease occurs in a violent form, accompanied by high fever and severe pain. Redness, swelling, and swelling are observed in the affected area. On different parts of the skin there is a ring-shaped allergic rash. Infectious-allergic arthritis is treated by a rheumatologist and an allergist.
Signs and symptoms of infectious arthritis
The key symptom of infectious arthritis is considered to be an acute manifestation, accompanied by a large number of symptoms.
Among the main signs and symptoms of infectious arthritis, general symptoms include fever, chills, excessive sweating and a constant feeling of weakness. As an additional symptom, children may experience nausea and vomiting.
Considering the local signs of infectious arthritis, it is worth highlighting:
- sharp pain during palpation/performing movements;
- local redness of the skin, swelling, fever.
It is also worth noting that the clinical picture of arthritis of infectious origin directly depends on the causes of its occurrence. Thus, septic arthritis is often localized in large joints, arthritis of gonococcal etiology is accompanied by multiple rashes, and tuberculous arthritis corresponds to a chronic course.
Particular attention should be paid to the symptoms of viral arthritis: short-term course, the possibility of restoration of articular tissues, without negative consequences
.
General information about the disease
Infectious arthritis is inflammation of a joint caused by a local or general infection. The symptoms of the disease and its course largely depend on the infection that caused the infectious process.
Codes for infectious arthritis according to ICD-10:
- staphylococcal - M00.0;
- pneumococcal - M00.1;
- streptococcal - M00.2;
- caused by other specified bacterial pathogens - M00.8;
- pyogenic unspecified - M00.9;
- tuberculosis – M01.1;
- gonococcal - M01.3;
- viral – M01.5.
The disease is very common and can cause permanent impairment of joint function. A quarter of patients seeking treatment for joint diseases suffer from infectious arthritis.
Stages of development of infectious arthritis
In order to understand how to treat infectious arthritis and what measures will be most effective, it is important to understand at what stage the disease is.
In total, it is customary to distinguish 4 main stages of arthritis:
- Stage 1
– accompanied by the development of osteoporosis (chronically progressive decrease in bone density of the joint), without destructive changes; - Stage 2
– the initial stage of destruction of cartilage tissue, reduction of the joint space, the occurrence of single usurs (destructions on the surface) of the bone; - Stage 3
– significant damage to articular tissues, pronounced reduction in the joint space, the presence of subluxations and deviations (deviations from the norm) of the bones; - Stage 4
– symptoms of stage 3 + complete immobility of the joint.
Dangers
The disease is often severe, with complications.
Stages of the disease
The course of the disease is associated with its clinical form, so the stages of development of the pathological process can have significant differences. Let's consider the stages of development of acute purulent arthritis, developed by the Research Institute named after. Vishnevsky:
- Initial
– purulent process without destruction of intra-articular tissues:- A.
- without damage to periarticular tissues; - V.
– with the development of purulent processes in adjacent tissues. - Expanded
– purulent arthritis with destruction of intra-articular tissues:- A.
- without damage to periarticular tissues; - V.
– with purulent lesions of the surrounding soft tissues. - Launched
– with damage to bone and cartilage tissue:- A.
- without damage to surrounding tissues; - V.
– with purulent lesions of these tissues; - S.
– with the release of pus to the surface of the body (fistulas). - Final
:- in the absence of adequate treatment
- destruction, joint immobility, disability; - with proper treatment
, complete or partial restoration of limb function.
Any form of arthritis has serious complications, so you should not delay treatment.
See how easily the disease can be cured in 10-12 sessions.
Possible complications
Infectious arthritis can cause early and late complications. Early complications include mainly complications of purulent arthritis:
- suppuration of periarticular tissues;
- generalization of infection, sepsis.
Long-term consequences include loss of limb function of varying degrees: from mild to complete immobility.
Complications can only be avoided if you consult a doctor in a timely manner.
Types of arthritis of infectious origin
Considering the etiology of the disease, it can be noted that all infectious arthritis have several varieties, including:
- bacterial;
- viral;
- fungal;
- parasitic
.
At the same time, depending on the identified type of disease, the following subtypes of arthritis are also distinguished:
- septic
(pyogenic/purulent); - gonorrheal
; - syphilic
, etc.
Bacterial (septic) arthritis
About the article
5920
0
Regular issues of "RMZh" No. 20 dated October 25, 2004 p. 1137
Category: Rheumatology
Author: Belov B.S.
For quotation:
Belov B.S. Bacterial (septic) arthritis. RMJ. 2004;20:1137.
Bacterial (septic) arthritis (BA) is a rapidly progressive pathology caused by direct invasion of the joint by pyogenic microorganisms 1 . The disease occurs everywhere. Mostly children and people over 60 years of age are affected. The annual incidence of asthma is 2–10 cases per 100,000 population, and among patients with rheumatoid arthritis (RA) and recipients of valve prostheses, these values reach 30–70 per 100,000. Despite the extensive arsenal of antimicrobial agents developed and introduced into clinical practice and intensive development surgical technology, irreversible loss of joint function develops in 25–50% of patients. The incidence of deaths from asthma has not changed significantly over the past 25 years and is 5–15% [1]. Etiology Theoretically, all known bacteria can cause AD (Table 1). The most common etiological agent of asthma is S. aureus, which accounts for up to 80% of cases of joint infections in patients with RA and diabetes mellitus. This pathogen is also the main one in infectious coxitis and polyarticular variants of asthma. In second place in the frequency of isolation in patients with asthma are streptococci (primarily β-hemolytic streptococcus of group A), which, as a rule, are associated with underlying autoimmune diseases, chronic skin infection and previous trauma. The occurrence of S. pneumoniae as a causative agent of asthma has decreased significantly in recent years. Streptococci of other groups (B, G, C and F - in descending order) are isolated from asthma in patients with immune deficiency, malignant neoplasms, as well as infectious pathologies of the digestive and urogenital tract. Gram-negative bacilli are the cause of asthma in elderly patients, drug addicts who inject drugs intravenously, as well as in patients with immunodeficiency. Anaerobes as causative agents of asthma are more often found in recipients of joint prostheses, people with deep infections of soft tissues and patients with diabetes mellitus. The most significant etiological agents of asthma among children are S. aureus and Str. pyogenes. The role of H. influenzae, previously quite common in asthma in children, has significantly decreased in recent years due to the widespread introduction of a specific vaccine. At the same time, a number of researchers have noted an increase in the incidence of the gram-negative bacillus K. kingae in asthma, which is a normal inhabitant of the oral cavity in children under 2 years of age [6]. Table 2 summarizes data on the most common pathogens of asthma depending on the categories of patients. Pathogenesis Normally, articular tissues are sterile, which is ensured by the successful functioning of phagocytes of the synovial membrane and synovial fluid (SF). For the development of asthma, the presence of a number of “risk factors” is necessary, depending both on the state of the macroorganism (primarily anti-infective immunity and joint status) and the pathogenic microbe (virulence, exposure, inoculum volume, etc.). The main factors predisposing to the development of asthma are presented in Table 3. One of the most significant aspects of the occurrence of asthma is the weakening of the natural defenses of the macroorganism, due to concomitant diseases, immunosuppression, and the age of the patients. Of no small importance is the background articular pathology, the therapy performed, as well as possible complications of the latter. In particular, in RA, the likelihood of asthma increases due to the prescription of glucocorticosteroids (including intra-articular), cytotoxic immunosuppressants, as well as monoclonal antibodies to tumor necrosis factor - ? (infliximab). Penetration of the pathogen into the joint can occur in several ways. 1. Hematogenous dissemination with transient or persistent bacteremia, as a consequence of distant primary foci of infection (pneumonia, pyelonephritis, pyoderma, etc.). 2. Lymphogenic spread from foci of infection close to the joint. 3. Iatrogenic route during arthrocentesis or arthroscopy. 4. Penetrating injuries caused by plant thorns and other contaminated objects. Invasion of the bacterium into the joint is accompanied by an active inflammatory cellular response and the release of cells involved in inflammation into the joint cavity. Subsequently, under the influence of bacterial waste products, the immune response is stimulated and various inflammatory mediators are released. The accumulation of pro-inflammatory cytokines and phagocyte autolysis products – proteases – entails inhibition of cartilage synthesis and its degradation, followed by destruction of cartilage and bone tissue and the formation of bone ankylosis. Clinical picture As a rule, asthma is characterized by an acute onset with intense pain, swelling, skin hyperemia and hyperthermia of the affected joint. In most cases (60–80%) there is fever. However, body temperature can be low-grade and even normal, which is more common with damage to the hip and sacroiliac joints, against the background of active anti-inflammatory therapy for the underlying disease, as well as in elderly patients. In 80–90% of cases, a single joint is affected (usually the knee or hip) (Fig. 1). The development of an infectious process in the joints of the hands is mainly of traumatic origin (penetrating puncture wounds or bites). The oligo- or polyarticular type of lesion is more often observed with the development of asthma in patients with RA, systemic lesions of connective tissue, as well as in drug addicts who inject drugs intravenously. In addition, in “intravenous” drug addicts, asthma is characterized by a slower onset, a long course and frequent damage to the syndesmosis of the body (sacroiliac and sternoclavicular joints, pubic fusion). In young children, the only manifestation of bacterial coxitis may be sharp pain when moving with fixation of the hip joint in a position of flexion and external rotation. Unlike gonococcal arthritis, BA is not characterized by damage to periarticular soft tissues. Diagnostics When analyzing peripheral blood in patients with asthma, leukocytosis is detected with a shift in the leukocyte formula to the left and a significant increase in ESR. The basis for diagnosing BA is a detailed analysis of the fluid obtained by puncture aspiration from the affected joint (in this case, it is necessary to remove the effusion to the maximum extent possible). A definite diagnosis of AD requires identification of bacteria in the SF. It is inoculated on media for aerobic and anaerobic microbes and should be performed immediately after collection (at the patient’s bedside). In order to obtain preliminary information about the pathogen and prescribe empirical antibacterial therapy, Gram staining of smears is necessary, and the effectiveness of the study is increased by preliminary centrifugation of the fluid. The diagnostic efficiency of this technique is 75% and 50% for infection with gram-positive cocci and gram-negative bacilli, respectively. Visually, SF in BA is purulent in nature, grayish-yellow or bloody in color, intensely turbid, thick, with a large amorphous sediment. When counting leukocytes, the level of cytosis often exceeds that in other inflammatory diseases (RA, gouty arthritis, reactive arthritis) and is >50,000/mm 3 , often more than 100,000/mm 3 with a predominance of neutrophils (>85%). SF also has low glucose levels, less than half of serum concentrations, and high levels of lactic acid. Blood cultures for blood culture give positive results in 50% of cases. X-ray of the joint is one of the first-priority diagnostic measures, since it allows one to exclude concomitant osteomyelitis and determine further tactics for examining and treating the patient. However, it should be noted that distinct changes on radiographs in BA (osteoporosis, narrowing of the joint space, marginal erosions) appear approximately 2 weeks from the onset of the disease. The use of radioisotope scanning techniques with technetium, gallium or indium is especially important in cases where the joint under study is located deep in the tissue or is difficult to reach for palpation (hip, sacroiliac). These methods also help to identify changes inherent in AD at early stages of the process, i.e. during the first two days, when there are still no radiological changes. On computed tomograms, destructive changes in bone tissue are detected much earlier than on plain radiographs. This method is most informative for lesions of the sacroiliac and sternoclavicular joints. Magnetic resonance imaging can detect soft tissue swelling and effusion into the joint cavity, as well as osteomyelitis, in the early stages of the disease. Differential diagnosis Differential diagnosis of BA should be carried out with the following diseases manifested by acute monoarthritis: – acute gouty arthritis; – pseudogout; - rheumatoid arthritis; – viral arthritis; – seronegative spondyloarthritis; – Lyme borreliosis. It should be noted that joint infection is one of the few emergency situations in rheumatology that requires rapid diagnosis and intensive treatment, which avoids irreversible structural changes. Therefore, there is a rule - to regard every acute monoarthritis as infectious until proven otherwise. Prosthetic joint infections The incidence of infection of prosthetic joints is 0.5–2%. Among the pathogens, staphylococci (primarily coagulase-negative), streptococci, gram-negative aerobes and anaerobes predominate (Table 4). Early forms of joint prosthesis infections (up to 3 months after implantation) are caused mainly by epidermal staphylococci and develop due to postoperative contamination or due to contact spread from infected skin, subcutaneous tissues, muscles or postoperative hematoma. Late forms occur during infection with other microbes presented in Table 4 and are caused by hematogenous dissemination. The main risk factors for damage to prosthetic joints include: immunodeficiency states, RA, repeated operations on the joint, long-term surgical intervention, prosthetics of superficial joints (elbow, shoulder, ankle). The onset of the disease can be acute or subacute depending on the virulence of the pathogen. Pain appears (95%), fever (43%), swelling of the joint (38%), outflow of purulent discharge through the drainage (32%). This symptomatology, combined with radiographic signs of destruction of bone tissue near the prosthesis, always indicates infection. Distinguishing a surgical skin infection from a purulent lesion of a joint prosthesis often causes great difficulties. The final diagnosis is made by blood tests, examination of aspirate from the cavity of the artificial joint and/or bone biopsy taken near the area where the cement joins the prosthesis. Treatment Treatment of asthma is complex, including antimicrobial and symptomatic therapy, drainage of infected fluid and physical therapy. Antimicrobial therapy is carried out empirically during the first 1–2 days, taking into account the patient’s age, the clinical picture of the disease and the results of a Gram smear study of the liver, and subsequently, taking into account the isolated pathogen and its sensitivity to antibiotics (Tables 5, 6). Antibiotics should be administered predominantly parenterally; their intra-articular use is inappropriate. The lack of positive dynamics after 2 days dictates the need to change the antibiotic. Continued accelerated ESR is an indication for prolongation of treatment, which averages 3–4 weeks. (sometimes up to 6 weeks), but not less than 2 weeks. after the elimination of all signs of the disease. In addition to antimicrobial therapy, analgesics and non-steroidal anti-inflammatory drugs (diclofenac, ketoprofen, etc.) are prescribed. Drainage of the infected joint is carried out (sometimes several times a day) by closed aspiration through a needle. In order to assess the effectiveness of treatment, leukocyte counts, Gram staining and SG cultures are performed each time. Open surgical drainage of the infected joint is carried out in the presence of the following indications [7]: – infection of the hip and, possibly, shoulder joint; – vertebral osteomyelitis, accompanied by compression of the spinal cord; – anatomical features that make drainage of the joint difficult (for example, the sternoclavicular joint); – impossibility of removing pus with closed drainage through a needle due to increased viscosity of the contents or adhesions in the joint cavity; – ineffectiveness of closed aspiration (persistence of the pathogen or lack of reduction in leukocytosis in the synovial fluid); – prosthetic joints; – concomitant osteomyelitis requiring surgical drainage; – arthritis that develops as a result of a foreign body entering the joint cavity; – late start of therapy (more than 7 days). During the first two days, the joint is immobilized. Starting from the 3rd day of illness, passive movements in the joint are performed. Loads and/or active movements in the joint are started after the arthralgia disappears. Treatment of an infected prosthetic joint is carried out as follows: 1. Simultaneous arthroplasty with excision of infected tissue, installation of a new prosthesis and a subsequent 6-week course of antibiotic therapy (vancomycin + amikacin; vancomycin + cefepime/ceftazidime; oxacillin + rifampicin). 2. Excision of prosthetic components, contaminated areas of skin and soft tissue, followed by parenteral antimicrobial therapy for 6 weeks. After this, the joint is reimplanted with continued antibiotic therapy for 5 days. Prevention The likelihood of infection of a prosthetic joint increases significantly during bacteremia that occurs during dental and urological procedures. In this regard, experts from the American Academy of Orthopedic Surgery, the American Dental Association and the American Urological Association have developed antibiotic prophylaxis regimens for individuals at high risk of developing joint prosthetic infection [11,12]. All recipients of joint prostheses are subject to prophylaxis during the first two years after surgery, patients with immunosuppression due to the underlying disease (RA, systemic lupus erythematosus) or drug/radiation therapy, as well as patients with aggravating concomitant pathology (previous infection of the joint prosthesis, hemophilia, HIV -infection, insulin-dependent diabetes type I, malignant neoplasms) when they undergo a number of dental interventions, including tooth extraction, periodontal manipulation, installation of implants, etc. The above categories of patients should also receive prophylaxis for various manipulations associated with a possible violation of the integrity of the mucous membrane of the urinary tract (lithotripsy, endoscopy, transrectal prostate biopsy, etc.) Antimicrobial prophylaxis regimens are presented in Table 7.
References 1. Goldenberg DL. Septic arthritis. Lancet. 1998;351(9097):197–202. 2. Weston VC, Jones AC, Bradbury N, Fawthrop F, Doherty M. Clinical features and outcome of septic arthritis in a single UK Health District 1982–1991. Ann Rheum Dis. 1999; 58(4):214–219. 3. Dubost JJ, Soubrier M, De Champs C, Ristori JM, Bussiere JL, Sauvezie B. No changes in the distribution of organisms responsible for septic arthritis over a 20 year period. Ann Rheum Dis. 2002; 61(3):267–269. 4. Kaandorp CJ, Dinant HJ, van de Laar MA, Moens HJ, Prins AP, Dijkmans BA. Incidence and sources of native and prosthetic joint infection: a community based prospective survey. Ann Rheum Dis. 1997; 56(8): 470–475. 5. Shirtliff ME, Mader JT. Acute septic arthritis. Clin Microbiol Rev. 2002; 15(4): 527–544. 6. Lahmann JD, Lahmann SJ Etiology of septic arthritis in children: an update for the 1990s. Pediatr. Emerg. Care. 1999; 15:40–42. 7. Gilliard WR Bacterial (septic) arthritis. In the book. West S.D. Secrets of rheumatology. /Trans. from English M., St. Petersburg – “Binom Publishing House” – “Nevsky Dialect”, 1999. 331–341. 8. Urban JA, Garvin KL Prosthetic joint infections. Curr. Treat. Opt. Infect. Dis. 2003; 5:309–321. 9. Rao N. Septic arthritis. Curr. Treat. Opt. Infect. Dis. 2002; 4: 279–287. 10. Trampuz A., Steckelberg JM Septic arthritis. Curr. Treat. Opt. Infect. Dis. 2003; 5:337–344. 11. Antibiotic prophylaxis for dental patients with total joint replacements. JADA. 2003; 134:895–898. 12. Antibiotic prophylaxis for urological patients with total joint replacements. J Urology 2003; 169(5):1796–1797.
Content is licensed under a Creative Commons Attribution 4.0 International License.
Share the article on social networks
Recommend the article to your colleagues
Diagnosis of infectious arthritis
Before determining how to treat infectious arthritis, it is important to understand what its etiology is.
(causes of occurrence) and
forecasts
. All the information necessary for this can be determined diagnostically.
Diagnosis of infectious arthritis is carried out by specialists in the field of surgery, traumatology and rheumatology. If necessary, you can also consult an infectious disease specialist or venereologist for advice.
Among the measures used to clarify the diagnosis, it is worth highlighting:
- ultrasound examination of the affected area (ultrasound);
- X-ray examination;
- CT/MRI of the joint.
The disease is diagnosed in people of different ages: from infants to the elderly.
Treatment of infectious arthritis
The primary treatment for arthritis of any type is pain relief
,
antibiotic therapy and
,
of course
,
fever reduction
.
In order to achieve the most effective results, both medicinal and non-medicinal methods can be used as treatment.
All
measures
included in the treatment plan for various types of arthritis
are determined exclusively by the attending physician
, based on the results of a diagnostic examination. In most cases, treatment of infectious joint inflammation is carried out inpatiently.
IMPORTANT! Self-medication can cause the situation to worsen and the consequences to become irreversible.
Physiotherapy as a method of treating infectious arthritis
Physiotherapy
is a unique treatment that can be used both at the treatment stage and for rehabilitation purposes after radical measures.
Among the most effective measures it is customary to highlight:
- magnetic therapy;
- use of amplipulse or sinusoidally modulated currents;
- electrophoresis (introduction of drugs into joint tissues through exposure to electric current);
- laser or ultrasound therapy;
- local exposure to paraffin or ozone.
Massage as a method of treating infectious arthritis
Massage
– a great way to improve/restore blood circulation to the affected joint. Despite its usefulness, you should resort to this method only after consultation with your doctor.
To treat various types of arthritis, the following types of massage can be used:
- local
– concentrated on a specific area of the human body;
- general
– the use of massage techniques is distributed throughout the body.
It is important to note that massage cannot be the only treatment for arthritis.
. Only an integrated approach, involving the use of drug treatment in tandem with physiotherapeutic methods, massage and specialized exercises, can give a chance for complete tissue restoration and elimination of the symptoms of the disease.
Exercise therapy as a method of treating infectious arthritis
Physiotherapy
– a special method of treating arthritis of various types, in particular those caused by infectious diseases.
Various types of exercises and static positions are an effective means of not only treating, but also preventing diseases of joint tissues.
A set of gymnastic exercises allows you to achieve stable remission and minimize pain, swelling and pathological tension of muscle tissue.
Frequently asked questions about the disease
What is the difference between infectious and reactive arthritis?
An infectious inflammatory process develops when an infection enters a joint, and a reactive inflammatory process develops against the background of some kind of general infection in the absence of a pathogen in the joint cavity. Read more about reactive arthritis in this article.
Which doctor treats you?
Nonspecific infectious processes - a surgeon or traumatologist, specific ones - a surgeon and another specialist - an infectious disease specialist, a dermatovenerologist, a phthisiatrician. When transitioning to a chronic course, a rheumatologist.
What is the prognosis for treatment of infectious arthritis?
Depends on the infection that caused the disease. Most acute arthritis ends in recovery. The outcome of specific infections depends on the course of the underlying disease: viral arthritis ends in complete recovery, while tuberculosis arthritis does not always have a favorable outcome.
Infectious arthritis can be severe with unpredictable consequences. Therefore, it is very important to treat it promptly and correctly. They know how to do this.
Bibliography:
- Belov B. S. // Bacterial (septic) arthritis and infection of the prosthetic joint: modern aspects. — [b.m.]: Modern rheumatology., 2010.
- Parvizi J Jacovides C, Antoci V, et all, // Diagnosis of periprosthetic joint infection:. — [b.m.]: J Bone Joint Surg AM, 2012..
- Isaacs J. Oxford textbook of rheumatology. – Oxford University Press, 2013.
- Slobodin G. et al. Acute sacroiliitis //Clinical rheumatology. – 2021. – T. 35. – No. 4. – pp. 851-856.
Themes
Arthritis, Joints, Pain, Treatment without surgery Date of publication: 03/04/2021 Date of update: 03/15/2021
Reader rating
Rating: 5 / 5 (1)
Use of drugs in the treatment of infectious arthritis
Drug therapy in the treatment of arthritis is a fairly effective method that has the desired effect on the patient’s body. In case of timely application of a well-chosen treatment plan, it can be stated that the prescribed therapy is successful
.
As part of treatment, taking into account the causes and characteristics of the course of the disease, various types of antibiotics
, as well as other groups of drugs. Let's look at some of them in detail.
Chondroprotectors in the treatment of infectious arthritis
Chondroprotectors
- This is a group of long-acting drugs, the use of which is necessary for several months.
Prescribing a course of drugs of the presented type allows you to create favorable conditions for the restoration of articular tissues, which significantly affects the patient’s quality of life, due to the restoration of the functionality of the affected joint
.
The most effective drug of the group of chondroprotectors is considered to be “ Structum”
».
Antispasmodics in the treatment of infectious arthritis
Use of antispasmodics
provides the opportunity to relieve patients from muscle pain that occurs as a result of joint damage.
Among the frequently prescribed ones, it is worth highlighting “ Drotaverine
».
Nonsteroidal anti-inflammatory drugs in the treatment of infectious arthritis
Nonsteroidal anti-inflammatory drugs
(NSAIDs) are excellent helpers in the treatment of arthritis. The action of drugs of this type allows the patient to get rid of pain.
The frequency, duration of use and dosage are determined by the attending physician, based on the existing clinical picture.
One of the most effective drugs of this type is “ Artradol
».
General clinical recommendations
Persons who have had acute infectious arthritis or suffer from chronic infectious arthritis must:
- lead an active healthy lifestyle, quit smoking and alcohol abuse;
- eat properly and fully;
- exclude heavy physical activity and injuries;
- engage in therapeutic exercises, swimming and feasible sports;
- treat infections promptly;
- carry out doctor's orders; in the chronic course of the disease, conduct courses of anti-relapse treatment.
Prevention
Infectious arthritis can be prevented by doing hardening, sports without heavy physical activity, eating right and treating all infections in a timely manner.
We combine proven techniques of the East and innovative methods of Western medicine.
Read more about our unique method of treating arthritis
Surgical method of treatment
In a situation where complex therapy is unable to cope with the existing degree of damage to the joint, radical methods come to the rescue, including surgery.
Surgical treatment of arthritis is used only in severe cases. Among the types of surgical intervention there are such measures as:
- arthroscopy
is a low-traumatic operation that involves the removal of bone processes; - endoprosthetics
– replacement of articular elements with implants; - arthrodesis
– absolute fixation of the joint; - osteotomy
- excision of part of the bone tissue of the affected joint in order to reduce pressure on it; - arthroplasty
is a complete replacement of the affected joint.
Forecasts and prevention of infectious arthritis
Considering the prognosis of the disease, it is worth noting that only one third of patients with arthritis of infectious origin at the end of treatment are faced with unpleasant residual effects, which are expressed by joint immobility.
The most dangerous types of the disease are septic arthritis, because despite fairly favorable prospects, the fatal outcome is 5-15%
.
The risk group for developing infectious arthritis includes people of different ages who have ailments such as:
- rheumatoid arthritis;
- osteoarthritis;
- bad habits;
- weakened immune system;
- obesity of varying degrees.
For the purpose of prevention, it is recommended to follow the basics of dietary nutrition, attend prescribed therapeutic events, promptly treat existing diseases and, of course, monitor the general health of the body.
Recommendations for infectious arthritis
To maintain the effectiveness of therapy, as well as achieve the most favorable results, it is important to follow a number of recommendations for infectious arthritis, including:
- Movement is an integral part of therapy.
- Maximum limitation of sudden movements and forces that create additional stress on the affected joints.
- Improving power sensations.
- Simplifying everyday processes through the use of modern technological solutions.
- Increasing personal safety by installing additional handrails in the apartment, using anti-slip mats, etc.
Features of nutrition during treatment and prevention of infectious arthritis
Therapeutic nutrition for arthritis of various types is aimed primarily at normalizing the immune response, as well as weakening inflammatory processes, in order to restore the range of motion of the affected joint.
Nutritional features depend on:
- stages of disease development;
- presence of concomitant diseases;
- severity of clinical manifestations.
Based on this, we can come to the conclusion that there is no single diet. However, there are a number of general principles for creating a diet, including:
- fractional meals;
- preference for certain types of culinary food processing (boiling/baking/steaming/stewing);
- food intake temperature – no more than 60°C;
- limiting salt and liquid intake;
- giving up bad habits;
- saturating the diet with vitamins.
How is rheumatoid arthritis treated?
At the initial consultation, the rheumatologist will prescribe additional examinations - a blood test, x-ray of the joint, ultrasound or MRI. It is impossible to completely cure the disease, so therapy is aimed at relieving unpleasant symptoms and preventing complications.
- Anti-inflammatory drugs relieve inflammation and pain.
- Immunomodulatory - inhibit immune reactions.
With proper treatment, remission lasts a very long time, and sometimes the disease disappears completely, but treatment will take many years. But it is strictly forbidden to massage or warm up joints affected by rheumatoid arthritis. Such manipulations lead to exacerbations.
For rheumatoid arthritis, massage and warming are contraindicated