Victor Borisovich, when does the danger of enterovirus infection most often arise?
Today, enterovirus infection is one of the most pressing infectious problems in St. Petersburg.
The incidence rate increases in summer and autumn, when it is warm enough outside. The infection is relevant primarily for children. It is most often transmitted by water and airborne droplets. And very often, both adults and children bring the infection from the southern regions. Many remember the outbreak in Turkey last year, and in St. Petersburg there are still isolated cases of infection to this day.
Very often problems arise with differential diagnosis. We must understand that the group of enteroviruses is very large; it includes many enteroviruses themselves, viruses of the ECHO group and the Coxsackie group. Often these three types of viruses can cause an infectious disease in combination. Because of this, there is no specific form of the disease that manifests itself in the same way in everyone; the symptoms are mixed.
What kind of “beast” is this and where does it come from?
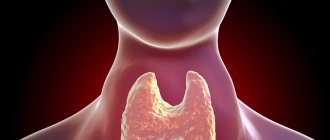
Enteroviruses are a genus of viruses, the name of which implies that their main site of introduction and reproduction is the gastrointestinal tract (from the Greek “entero-” - “associated with the intestines”).
Main two subgroups
- Coxsackie (named after the city of Coxsackie, USA, where it was discovered)
- ECHO (e-enteric, c-cytopathic, h-human, o-orfan, literally: enteric cytopathic orphan viruses, since they were not initially associated with the development of diseases). More than 60 serotypes of viruses are known, but not all are pathogenic.
Enteroviruses are ubiquitous. In countries with warm and humid climates, the incidence remains at the same level throughout the year. In Russia, the peak occurs at the end of summer and autumn, until the coldest weather. Children are more susceptible to infection, although adults can also get sick.
What forms of enterovirus are there? Is it possible to determine them yourself?
Today, the most common clinical forms are:
- "Minor illness" Accompanied by high fever and moderate muscle pain.
- Epidemic polymyalgia. On the contrary, the temperature rises slightly, but muscle aches are pronounced, especially in large muscle masses - in the calf muscles, thigh muscles, lower back and anterior abdominal wall.
- A more striking form is herpangina. It is often confused with bacterial sore throat, and people begin to treat themselves and their children with antibiotics, which only worsens the situation. Although this is a herpetic sore throat, it is still caused by enteroviruses. The fact is that with herpetic diseases there are vesicular (vesicle - a small transparent bubble) rashes in the oropharynx, but they also happen with enteroviruses. Since previously it was not possible to find out the etiology of this disease, it was believed that these were not enteroviruses, but herpetic diseases. Subsequently, enteroviruses were isolated separately, but the name was left the same. Herpangina is a disease that is caused by enteroviruses, and the main clinical manifestations of which are: fever, sore throat and specific rashes on the anterior palatine arches, tonsils, soft palate and posterior wall of the oropharynx.
- The most common clinical form in St. Petersburg is a disease of the “hand-foot-mouth” type. There may be a fairly high temperature, sore throat, rash. But the main difference is a vesicular rash over the body. The rash is usually not abundant - single blisters are found on the arms, legs, torso, abdomen and back. Its main difference from rubella or chickenpox is the appearance of a rash on the palms and soles, which never occurs with chickenpox and rubella. This is one of the main diagnostic signs that allow you to detect enterovirus.
Often, muscle aches are added to the described manifestations, which is why the disease is initially confused with the flu.
Causes
Coxsackie viruses of group A (serotypes 1-22, 24) and group B (serotypes 1-6) are the etiological factor of a number of enteroviral infections.
Morphology and biological properties
Coxsackie enterovirus is a small RNA virion (28 nm) with cube-shaped symmetry and the ability to form crystals inside affected cells. Virion capsid without envelope. The appearance of the Coxsackie virus is shown in the figure below.
Coxsackievirus B4
Based on their antigenic structure, Coxsackie viruses are divided into two large groups: A-26 and B-6 serological types. The virus is highly resistant in environments and on environmental objects. But they are quickly inactivated at temperatures exceeding 50 ° C, they can persist for 2 months at a temperature of 37 ° C, survive for a long time in river/tap water, but especially for a long time in waste water.
Stable in acidic environments (pH 3-5). The activity of enteroviruses remains for several years even when frozen, and when stored in a refrigerator at a temperature of +4-6°C - for several weeks. At the same time, repeated freezing and subsequent thawing does not lead to a decrease in their activity. They quickly die when dried, under ultraviolet irradiation and when exposed to formaldehyde , even in small concentrations. They are destroyed by boiling (at 100 °C - instantly, 60 °C in 6-8 minutes).
Epidemiology
Coxsackie viruses are ubiquitous: their reservoir in nature is water, soil, and food. In the human population, the human body. The main epidemiological feature is the widespread ability to form healthy virus carriers in the human body with a long period of virus release into the external environment (up to 3-6 weeks). Virus carriage in healthy individuals varies between 17-40%. Among children, the percentage of virus excretors reaches 20%, and at the age of under 1 year it is even higher - 32.6%. This feature contributes to the survival of the virus even in conditions of high levels of immunity in the population.
The level of natural immunity increases with age, reaching 90% already at the age of 5-10 years. Among the adult population, antibodies to the most common Coxsackie serotypes are found in 30-80% of the population. At the same time, the seropositivity of the human population is much higher in regions/countries/cities with a low social and hygienic standard of living. Some authors even consider these data as an indicator of the standard of living of the population and even the effectiveness of anti-epidemic protection.
The source of infection is a sick person, a recovering person or a virus carrier. Infection with Coxsackie viruses occurs throughout the year, but in the northern hemisphere the peak incidence of EVI occurs in the summer-autumn season. In warm regions and the tropics, the incidence does not have a pronounced seasonality. EVI affects people of all age groups, but incidence rates are inversely proportional to age. About 75% of EVI cases occur in children under 15 years of age, and children under 1 year of age get sick several times more often than older children and adults. Males get sick more often.
The leading mechanism of transmission is fecal-oral. Its implementation is carried out by water, food and household contact. Airborne and transplacental (from mother to fetus) routes are possible. The main condition for the implementation of the infection transmission mechanism is poor sanitary living conditions. The infection rate of children living in unfavorable sanitary conditions can reach 50%.
The most important way for Coxsackie viruses to spread is through contact with another person's contaminated hands and objects, followed by inoculation of the virus through the nose, mouth or eyes, and through contaminated food and water. Those infected are most contagious during the first week of illness.
What treatment is there?
To date, there is no specific therapy for each enterovirus in the world. General antiviral treatment includes interferon-type drugs. These drugs do not stimulate one’s own immunity, but introduce ready-made interferon into the body, in particular interferon Alpha 2B, which has moderate antiviral activity not only against enteroviruses, but also against many other infections.
Interferon inducers that stimulate the immune system should be used strictly under the supervision of a physician, since their effect on the body is quite complex, and the doctor must take into account various factors before prescribing them.
Treatment for manifestations of enterovirus infection will vary depending on the symptoms. If the patient has a high fever and muscle pain, then non-steroidal anti-inflammatory drugs are prescribed. For fever, this is paracetamol, anti-inflammatory - ibuprofen, for sore throat and herpangina - local antiseptic solutions.
Enteroviruses infect the small intestine, as their name suggests, because “entero” is translated from Latin as “small intestine.” If abdominal pain and stool disorders appear, sorbents and probiotics are used, sometimes enzymes, depending on the nature of the digestive disorders.
Pathogenesis
For Coxsackievirus A and B, the entry gates are the mucous membranes of the oral cavity, upper respiratory tract and intestines. Enteroviruses freely overcome the “gastric barrier” and penetrate the cells of the small intestinal mucosa. Subsequently, the process of virus replication occurs in the cells of the intestinal epithelium, lymphoid tissue and mesenteric lymph nodes. The virus then enters the bloodstream and causes primary viremia. The Coxsackie virus exhibits the greatest tropism for cells of the central nervous system/muscle tissue, but a variety of organs are also involved in the pathological process.
Dissemination of the pathogen occurs in the heart, liver, lungs, kidneys, eye vessels, pancreas, where it multiplies and accumulates. Clinical symptoms, severity and outcome of the disease are determined by a number of factors - the biological properties of the virus serotypes, their tropism, the state of the humoral/cellular immunity of the human body. Swelling, inflammation and areas of necrosis develop in the affected organs.
The stages of pathogenesis are shown schematically in the figure:
Stages of pathogenesis of the Coxsackie virus
Persons who have recovered from the disease develop long-lasting (over several years) type-specific immunity.
Create a short algorithm for the treatment of enteroviruses
If we describe the treatment tactics briefly, then:
- First, we determine that it is a viral infection and not a bacterial one - this is the key to successful treatment. At the slightest doubt, consult a doctor.
- We focus on the manifestations of the disease and determine the clinical form.
- We treat with interferon drugs and symptomatic medications.
We must not forget that the disease progresses differently in different people, and sometimes even a doctor finds it difficult to determine one or another clinical form. Therefore, it is important not to trust self-medication, but to contact a specialist in time, who can carry out the necessary tests and procedures, and get the patient back on his feet.
Tests and diagnostics
The diagnosis of a specific nosological form of EVI is made on the basis of complaints, clinical manifestations, data from laboratory and instrumental examinations.
Laboratory tests include: CBC, OAM, analysis for Coxsackie virus (nasopharyngeal swab, vesicle contents, cerebrospinal fluid for enteroviruses using PCR), blood for CSC/PHA.
Additional diagnostic examinations: ECG, biochemical blood test (bilirubin, creatinine, AlAt, AsAt, urea), blood coagulogram, comprehensive ultrasound, MRI.
Prevention of Coxsackie virus
There is still no specific prevention, which is due to the large number of serotypes of the virus. Nonspecific prevention includes:
- compliance with personal hygiene rules (thorough hand washing with disinfectant solution after visiting the toilet/before eating);
- Thorough washing of fruits and vegetables before consumption and rinsing with boiling water;
- using bottled water for drinking;
- swim only in permitted places; do not swallow water while swimming;
- avoiding contact with persons with clinical manifestations of EVI.
When a focus of EVI is identified, in order to localize it, the following is carried out:
- Active identification of patients with EVI and persons in contact with patients and establishment of monitoring of them.
- Isolation and hospitalization of patients (if necessary).
- Disinfection measures - disinfection (final and current).
- Strengthening sanitary supervision over catering, the water supply system, maintenance of the territory, compliance with the regime of organized children's groups and health care facilities.
- In case of an unfavorable epidemiological situation, it is recommended to administer 0.3 ml/kg of gamma globulin to all persons in the foci of infection.