Measles belongs to the rash infectious diseases. The causative agent of the disease is an RNA virus from the genus of paramyxoviruses Measles morbillivirus.
Susceptibility to this disease is almost universal, but measles has the character of a childhood disease only because most people get it already in childhood, and thus protect themselves for life. Secondary measles diseases still occur, although very rarely.
Measles is possible at all ages, but infants in the first 4-5 months of life are very little susceptible to measles poison, so diseases at this age are observed only rarely.
Infection occurs easily; it occurs mainly through contact and can be transmitted through healthy persons or objects only for a very short period of time. So, for example, a caretaker, if negligent, can transfer measles from one child to another in a hospital, but measles poison does not remain for a long time on a dress, underwear or other objects, and from a practical point of view one has to take into account only the transfer of infection directly from the sick to the healthy.
Doctor Komarovsky will tell you about this disease in detail.
The spread of the disease is favored, on the one hand, by a long incubation period, lasting 11 days, and on the other hand, by a catarrhal prodromal period, during which recognition of the disease is often impossible.
Finally, its spread is also influenced by the concentration of children susceptible to it in schools, nurseries, shelters, and other institutions. This is where extensive epidemics often begin.
How does measles develop (pathogenesis of the disease)
The entry point for measles viruses is the mucous membrane of the oral cavity, pharynx, upper respiratory tract and conjunctival membrane of the eyes. First of all, viruses infect immune cells - macrophages, reticular and lymphoid cells. An increase in the number of lymphomacrophage elements leads to tissue proliferation and the formation of focal infiltrates. Actively multiplying, the viruses begin to penetrate regional lymph nodes and blood. The incubation period for measles ranges from 8 to 13 days.
Rice. 2. The photo shows measles in children. On the first day of the rash, the rash is localized on the face.
Viremia in measles
Viremia (entry of pathogens into the bloodstream) develops 3–5 days from the beginning of the incubation period. It reaches its maximum at the end of the incubation period and at the beginning of the rash period. During this time, viruses are fixed in the cells of the reticuloendothelial system. The work of immune mechanisms is launched, which leads to a massive release of pathogens. A second wave of viremia develops. Viruses reinfect cells in the mucous membranes of the mouth, pharynx and upper respiratory tract. When the virus is introduced into the central nervous system, measles encephalitis develops. The skin is affected. In some leukocytes, chromosomes are damaged, and the epithelium of the respiratory tract becomes necrotic.
Measles viruses cause hyperplasia of lymphoid tissue. In the adenoids and tonsils, lymph nodes and spleen, appendix and skin, in lung tissue and sputum, giant multinucleated Warthin-Finkeldey cells appear. Detection of these cells is a pathognomonic sign of measles.
On the third day of the rash, the number of viruses in the blood decreases, and on the 4th day their blood disappears completely. Virus-neutralizing antibodies appear in the blood.
Rice. 3. The photo shows giant multinucleated Warthin-Finkelday cells.
Origin of measles rash
Allergic reactions develop to the protein components of pathogens in the patient’s body. The permeability of small vessels increases, their walls are damaged. In organs and tissues (usually the respiratory and digestive systems) in the mucous membranes, catarrhal-necrotic inflammation develops. The upper layers of the skin are affected, on which a papular rash first appears. Subsequently, the epidermal cells undergo necrosis, which is manifested by peeling.
In the oral cavity, the epithelium also undergoes necrotization. It becomes cloudy. Foci of necrosis become similar to small white dots (Belsky-Filatov-Koplik spots). They appear a day before skin rashes. The skin rash appears in stages, starting from the head and then gradually spreading to the entire body.
Rice. 4. In the photo, the symptoms of measles are Belsky-Filatov-Koplik spots.
Development of complications
Measles viruses in the patient’s body suppress both general and local immunity. Under their influence, the number of T-lymphocytes decreases. Anergy develops. Chronic diseases are getting worse. The addition of a secondary infection causes the development of catarrhal-necrotic inflammation in the upper respiratory tract, digestive system and skin.
Causes
Measles is caused by a viral infection and is highly contagious. It is estimated that about 90 percent of unvaccinated people close to those in the contagious phase of measles will also become infected.
Measles is spread in a similar way to colds and flu, that is, by inhaling airborne droplets that an infected person coughs or sneezes on. Although physical contact, coughing and sneezing are the most common ways to spread the infection, you can also get measles simply by breathing contaminated air or touching a contaminated surface and then inhaling droplets.
The measles virus can live for up to two hours on surfaces and in the air.
Signs and symptoms of measles in children and adults
Periods of the disease
During classical measles, four periods are distinguished: catarrhal, period of rash, pigmentation and recovery. The average duration of the disease is about 10 days. Fluctuations range from 8 to 21 days. Each period lasts 3 days. The catarrhal period can extend up to 7 days.
Incubation period
The incubation period (the period from the moment of infection with viruses until the appearance of the first symptoms of the disease) for measles is about 10 days. Fluctuations range from 8 to 13 - 17 days.
Rice. 5. The photo shows the appearance of a measles rash.
Signs and symptoms of measles during the catarrhal period
The disease begins with the development of inflammation of the mucous membranes of the upper respiratory tract and the conjunctiva of the eyes. There is copious mucous discharge from the nose, hoarseness and a dry cough. Body temperature rises to 39°C. Symptoms of intoxication appear: weakness, weakness, general malaise and loss of appetite.
The conjunctiva of the eyes becomes hyperemic, the eyelids swell, and purulent discharge appears from the eyes. There is a decrease in the number of lymphocytes in the blood (lymphopenia).
When a rash appears, catarrhal symptoms weaken and disappear completely after 1 - 2 days. In the oral cavity, against the background of a hyperemic, loose and rough mucous membrane, small (the size of a poppy seed) whitish spots with a red rim along the periphery appear. The rashes are called Belsky-Filatov - Koplik spots. They are usually located on the cheek mucosa in the area of the molars. Pink spots (measles enanthema) appear on the mucous membrane of the soft and hard palate.
By the end of the third day, there is a decrease in body temperature, but during the period of the appearance of measles rash it again rises significantly, and the symptoms of intoxication and damage to the upper respiratory tract intensify.
Rice. 6. In the photo, the symptoms of measles are Belsky-Filatov-Koplik spots on the mucous membrane of the cheeks and measles enanthema in the palate.
Measles rash
The measles rash looks like papules about 2 mm in size, surrounded by an irregularly shaped area of redness. In some places the rash merges and then their configuration is similar to complex figures with wavy (scalloped) edges. The basic background of the skin remains unchanged. Sometimes petechiae (hemorrhages) are observed against the background of a measles rash.
The patient's rash appears on the 4th - 5th day of the disease. Initially, it is localized on the face, neck and behind the ears. Within a day, the rash spreads to the entire torso and covers the upper arms. After another day, the skin of the legs and lower arms becomes covered with a rash, while the rash on the face begins to turn pale.
In severe cases of the disease, the rash is confluent in nature. It covers all skin, including the palms and soles. Numerous hemorrhages and even hemorrhages appear on the skin, the diameter of which exceeds 3 mm (echimosis, in everyday life - bruises). Hemorrhages also appear on the mucous membrane of the eyes and mouth. Puffiness of the face, eyelids, nose and upper lip, redness of the conjunctiva of the eyes, purulent discharge, and rhinorrhea are the main symptoms of measles during this period.
After 3-4 days, a period of fading of the rash begins. Body temperature decreases. Pigmentation appears at the site of the rash - brown spots.
Rice. 7. The photo shows measles in a child, the initial stage. The rash at the beginning of the disease is localized on the face, neck and behind the ears (the first day of the rash).
Rice. 8. The photo shows measles in children. The rash appears on the torso and upper arms (second day of rash).
Rice. 9. In the photo, a child has measles. Measles rash, 2nd day of rash.
Signs and symptoms of measles in children and adults in the pigmentation stage
Pigmentation of the measles rash indicates that the infectious process has entered the stage of ending the period of contagiousness and recovery of the patient.
Pigmentation of the rash, like rashes, occurs in stages. It is caused by the penetration of red blood cells into the skin during a rash and the subsequent breakdown of hemosiderin, a pigment that is formed as a result of the breakdown of hemoglobin.
The process begins on the 7th - 8th day of the disease and lasts up to 7 - 10 days. Pityriasis-like peeling is observed in areas of the rash. Body temperature gradually normalizes.
The general condition of the patient is returning to normal slowly. The phenomena of asthenia and immunosuppression persist for a long time.
Rice. 10. The photo shows a measles rash in the pigmentation stage.
Signs and symptoms of measles in children of the first year of life
Measles in children of the first year of life has its own characteristics:
- catarrhal period is often absent,
- an increase in body temperature and the appearance of a rash occur simultaneously,
- bowel dysfunction is often observed,
- bacterial complications are recorded in 2/3 of children.
Rice. 11. The photo shows symptoms of measles: enlarged lymph nodes and conjunctivitis.
Preventive measures
Prevention of measles in children includes several important points.
- Vaccination. The most effective protection is a vaccine. It can be single-component or multi-component (MMR, or measles, mumps, rubella). The vaccination is carried out at 1 year, then again at 6 years. Up to 10% of vaccinated children may develop a mild form of infection with a minor rash and fever. At this point, children are considered not contagious. Due to the massive refusal of vaccinations in Russia, cases of measles have become more frequent. According to statistics, 80% of children who suffered from this disease were not vaccinated.
- Taking immunoglobulin, or passive immunization. If it is known that the child had contact with a carrier of measles or was in an outbreak of the disease, immunoglobulin can be used, which provides immunity from infection for one month.
- Quarantine. In the children's group where a case of measles was recorded, anti-epidemic measures and daily preventive examination of children are carried out. A child is considered contagious several days before the first symptoms appear, as well as for 5 days after the first skin rash appears. Staying in a children's group is prohibited. Quarantine is carried out only for unvaccinated children under 17 years of age.
Recurrence of measles occurs in extremely rare cases. After an illness, immunity is lifelong. After vaccination, stable immunity remains for 15 years.
Complications (consequences) of measles
The cause of measles complications is the effect of the virus on the patient’s immune system. In the peripheral blood, the number of T-lymphocytes sharply decreases. Allergization of the body to the protein components of viruses contributes to the development of inflammation, which leads to increased permeability of small vessels and damage to their walls. In the mucous membranes of organs and tissues (usually the respiratory and digestive systems), catarrhal-necrotic inflammation develops.
- The layering of a secondary (viral-bacterial) infection leads to the development of a number of purulent-necrotic inflammatory processes in the nose, larynx, trachea, bronchi and lung tissue.
- Stomatitis and colitis develop.
- With the disease, conjunctivitis always develops. The cornea of the eye is often affected.
- During the period of pigmentation, inflammation of the middle ear often occurs.
- Under unfavorable sanitary and hygienic conditions, pustular lesions of the skin caused by streptococci and staphylococci develop.
- Microcirculation disorders in the brain lead to hypoxia and encephalopathy develops. Measles encephalopathy is more often recorded in young children. More severe complications of measles are encephalitis and meningoencephalitis. Pathology develops on days 5–7 of the disease. The course of the disease is severe, with a high mortality rate (up to 10%). Surviving children (about 40%) often have mental disorders and epilepsy.
- Damage to the optic and auditory nerves always results in serious consequences. Damage to the spinal cord leads to pelvic disorders.
- Very rarely, myocarditis, hepatitis and glomerulonephritis develop as a result of measles infection.
Rice. 12. The photo shows measles in children. The addition of a secondary infection leads to the development of bacterial conjunctivitis. The conjunctiva of the eyes becomes hyperemic, the eyelids swell, and purulent discharge appears from the eyes.
Diagnostics
When measles occurs in its typical form, it is not difficult to diagnose the disease. The presence of clear signs of measles described above will rule out other diseases. To make a diagnosis of an atypical form of the disease, the patient should undergo a number of additional tests:
- general blood and urine tests;
- blood test for the presence of the virus or nasopharyngeal smears (virological method);
- blood test for antibodies and increasing their titer (serological method);
- carrying out a hemagglutination inhibition reaction, which can indicate the presence of an infectious lesion.
When complications develop, the doctor additionally prescribes other tests. The most common among them are electroencephalography and chest x-ray.
Atypical forms of measles
In addition to the typical course, the disease may have an atypical course.
Atypical (erased) form
An atypical form of measles is observed in children 3–9 months old, since during this period the disease develops against the background of passive immunity, which they receive at birth from their mother. The incubation period for the atypical course is extended, there are no typical signs of the disease, the course is blurred, and the phasing of the rash is disrupted.
Measles in vaccinated children
If for some reason a vaccinated child does not have antibodies against the disease, then when infected with measles viruses, the disease will proceed normally. If a small amount of antibodies remains in the child’s body, then measles will occur in an erased form.
Mitigated measles
Mitigated measles develops when a measles vaccine or immunoglobulin is administered to a person infected with measles viruses during the incubation period. A situation arises when an infected person has acquired immunity to the disease, but its level is insufficient. The developed disease occurs in a mild form.
- The incubation period for mitigated measles is extended and ranges from 21 to 28 days.
- The catarrhal period is short and ends after 1 - 2 days, or is completely absent.
- Symptoms of the disease are mild.
- Body temperature is often absent or rises to low-grade levels. There are no Belsky-Filatov-Koplik spots on the buccal mucosa.
- The rash on the skin is scanty, not abundant, pale in color. It appears simultaneously on all areas of the skin and is often absent on the extremities. Not inclined to merge. The pigmentation of the rash is weak and disappears quickly.
- The disease proceeds without complications.
- Diagnosis of the disease is often difficult. The basis of laboratory diagnosis is serological testing.
"Black" or hemorrhagic measles
In severe cases of the disease, the rash may become hemorrhagic. Numerous hemorrhages and even hemorrhages appear on the skin, the diameter of which exceeds 3 mm (echimosis, in everyday life - bruises). Hemorrhages also appear on the mucous membrane of the eyes and mouth.
Congestive (dyspnoic) form of measles
The congestive or dyspnoic form of the disease is manifested by severe shortness of breath and continuous cough, with scanty physical data. The rash appears late and has a cyanotic tint. Hypoxia gradually increases. Lack of blood circulation in the brain leads to seizures and loss of consciousness. The cause of the congestive or dyspnoic form of measles is considered to be damage to lung tissue by viruses (pulmonary measles).
Reaction to vaccination
When administered a live measles vaccine, 25–50% of children develop a severe reaction resembling mitigated measles. This reaction occurs with elevated body temperature, catarrh of the upper respiratory tract and scant rash. Convulsions and vomiting are rarely observed.
Vaccinated individuals do not pose a danger to others. Children with immunodeficiencies are not allowed to receive vaccinations. The introduction of a live vaccine causes a severe reaction in them.
Course of measles in persons with immunodeficiency
In 80% of cases in people with immunodeficiency, the disease is extremely severe. In 70% of cases in cancer patients and in 40% of cases in HIV-infected people, measles is fatal. In a third of patients with immunodeficiency, there is no rash due to measles; in 60% of cases, the rash is atypical. The complications are severe.
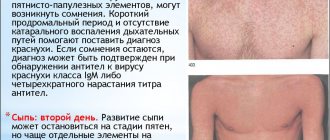
Rice. 13. Figure 22 and 23. The photo shows measles in children. In the photo on the left there is a rash on the face (day 1 of the rash), in the photo on the right there is a rash on the face and torso (day 2 of the rash).
Diagnosis
The diagnosis of measles is not difficult. The peculiar course of the disease, the almost regularly lasting 11 days incubation period, the prodromal stage lasting three days with its sharp catarrhal symptoms, and finally, the characteristic rash - all this makes it possible to make a diagnosis very easily.
But, it goes without saying that there are many cases in which the situation is not so simple.
In some of them, almost no phenomena are observed in the prodromal period, in others, instead of catarrh of the mucous membrane of the respiratory tract and eyes, a disease of the pharynx and tonsillitis develops, which at first is misleading.
Then the rash may be uncharacteristic, resemble scarlet fever, etc.
On the other hand, serum or drug rashes can be so similar to a typical measles rash that it is sometimes difficult to decide what is going on. In such cases, the solution to the issue depends on various studies.
Measles in adults
Measles in adults and adolescents is often severe. The intoxication syndrome is significantly expressed. Patients often experience severe headaches and vomiting. Sleep is disturbed. The catarrhal period lasts 4 - 8 days. Catarrhal symptoms of the upper respiratory tract are weakly expressed, Belsky-Filatov-Koplik spots are abundant, often persisting throughout the entire period of the rash. The rash is profuse. Several groups of lymph nodes are enlarged. Sometimes an enlarged spleen is palpable. Complications rarely develop.
Rice. 14. The photo shows measles in adults. A rash is the main symptom of the disease.
Etiology
Measles virus RNA containing a virus of the Paramyxoviridae family, genus Morbillivirus. The morphology of the virus is typical for paramyxoviruses: spherical virions with a lipoprotein envelope and a helical nucleocapsid, represented by one molecule of single-stranded minus RNA, the main nucleocapsid protein N phosphoprotein P and RNA-dependent RNA polymerase.
The outer surface of the virus shell consists of membrane lipids of target cells and glycoproteins (H and F) of the virus, protruding on it in the form of “spikes”.
Glycoprotein H - hemagglutinin, is responsible for the attachment (adsorption) of the virus to the surface of the target cell. The cellular receptor for the measles virus is the complement cofactor, the transmembrane protein CD46, found only on human and monkey cells. It is presented primarily on epithelial cells of the mucous membranes, skin, and neuroglia, which determines the epitheliotropy of the measles virus.
Glycoprotein F - ensures the fusion of the lipid envelope of the virus with the lipids of the target cell wall to form a pore (bridge) necessary for the penetration of the virus nucleocapsid. In addition, it is capable of causing the fusion of affected cells with many intact ones. As a result, symplasts are formed - giant multinucleated non-viable cells in which further accumulation of the virus occurs. Thanks to the mechanism of symplast formation, viruses do not enter the intercellular space, thereby avoiding exposure to virus-neutralizing antibodies.
Adjacent to the inner surface of the virus shell is a matrix or membrane protein, which is called the virion matrix (M). Hemagglutinin H, fusion protein F, membrane protein M, and nucleocapsid protein NP vary in their degree of immunogenicity. Hemagglutinin H is the most immunogenic, membrane protein M is the least immunogenic.
Virions penetrate the target cell without forming endosomes. RNA polymerase is introduced into the cell along with the virus nucleocapsid. Transcription, protein synthesis, and genome replication occur in the cytoplasm. The genome is transcribed by RNA-dependent RNA polymerase into individual mRNAs and the complete plus template for the genomic viral RNA. The newly synthesized genomes interact with the main proteins of the virus, forming nucleocapsids that bind to the M protein and are surrounded by a shell of modified plasmalemma of the target cell. Virions leave the cell by the process of budding.
Infection of T- and B-lymphocytes allows, on the one hand, to explain the development of “immune measles anergy”, on the other hand, the possibility in some cases of infection penetration through the blood-brain barrier with subsequent replication of the virus in the central nervous system with the development of acute encephalitis, meningoencephalitis.
measles virus
Replication of mutant strains of measles virus with a defect in the M protein is accompanied by the accumulation of viral nucleocapsids in infected neurons and glial cells without the formation of symplasts. This leads to long-term persistence of the virus in the central nervous system and can manifest itself in the development of subacute sclerosing panencephalitis 5-10 years after measles with an incidence of 1 in 300 thousand cases.
The measles virus is unstable in the environment and is killed by sunlight and ultraviolet rays within 8-10 minutes. At room temperature it inactivates after 3-4 hours and quickly dies when it dries; at a temperature of 56 degrees it dies after 30 minutes. The virus tolerates low temperatures well for several weeks. Sensitive to the effects of detergents and disinfectants.
The measles virus is cultivated on primary trypsinized cultures of monkey and human kidney cells. It suppresses the mitotic activity of cellular structures and can also have a mutagenic effect on chromosomes.
Prevention
Measles leaves lifelong immunity. Preventive measures are not carried out among persons who have recovered from the disease or have been vaccinated with live measles vaccine (in case of contact with a person with measles). Separation of contact non-immune persons is carried out from the 7th to the 17th day from the moment of contact with a patient with measles. Persons who have received measles immunoglobulin for prophylactic purposes are subject to separation from the 7th to the 21st day from the moment of contact.
A patient with measles is isolated from others until the 5th day, counting from the moment the rash appears, and in case of complications - until the 10th day. For contact non-immune persons, as a passive immunization, it is possible to administer anti-measles immunoglobulin in a dose of 1.5 - 3 ml no later than the 5th day from the moment of contact (later administration of anti-measles immunoglobulin is not effective). Passive immunity lasts up to 2 weeks.
According to the preventive vaccination calendar, vaccination with live measles vaccine is given to children from 12 months of age subcutaneously, once. However, in 2% of cases, vaccinated people may develop a typical picture of measles when infected.
Stages of rashes
The rash appears 3–5 days after the first signs of the disease. It is found first on the face in front and below the ears and on the sides of the neck as uneven spots, soon mixing with papules. Within 24 to 48 hours, the rash spreads across the trunk and limbs (including the palms and feet) and begins to fade on the face.
- The fourth day of the rash is characterized by regression of the rash elements, similar to the order of their appearance, leaving behind light brown areas of increased pigmentation, disappearing after 5-7 days. At the site of pigmentation, pityriasis-like peeling remains for some time (especially on the face).
Source of infection
The source of measles can only be a sick person. Even if the incubation period has not yet ended and the patient has not shown any symptoms of the disease, he may already pose a threat to the release of the virus and thereby the possibility of infection for others. People who are asymptomatic are also considered contagious. Persons after vaccination do not pose a danger to others, even if their temperature rises or rashes appear.
Treatment
An uncomplicated form of measles requires only symptomatic treatment. The immune system independently fights the disease. To relieve symptoms and avoid complications of the disease, the patient is shown:
- bed rest;
- medications for runny nose and conjunctivitis;
- cough and sore throat remedies;
- antihistamines;
- good nutrition;
- complex of vitamins.
The patient must be isolated immediately after detection of the rash. The room where it is located must be wet cleaned regularly (at least once every two days) using disinfectants - they can be replaced with a solution of vinegar and water. The room itself must be systematically ventilated.
Curtains or blinds should be kept closed—people with measles may be photophobic. Bright sunlight can cause them headaches and severe illness.
If the body temperature is high, antipyretic drugs are prescribed. But it is better not to take them if the temperature does not rise above 38.5 °C. If you do take them, carefully follow the dosage indicated in the instructions (maximum 2 times a day). High concentrations of paracetamol in the blood can lead to irreversible changes in the liver.
Food should be liquid and easily digestible. It is better to replace synthetic vitamins with berries, fruits and vegetables. Natural vitamins are absorbed better and faster by the body, especially during illness. They take part in the fight against the virus and the subsequent restoration of the body.
It is also necessary to drink a lot of warm liquid (not boiling water) - at least 2.5 liters of still water per day. Teas with medicinal herbs have a particularly beneficial effect on the patient’s condition:
- camomile tea;
- infusion of St. John's wort;
- rosehip tea;
- linden infusion.
They contain a huge amount of antioxidants that remove toxins and promote rapid recovery. An infusion of licorice root can relieve a cough; it has expectorant properties. It is necessary to take 150-200 ml of infusions throughout the day (3-4 times).
Despite the fact that measles often goes away without drug treatment, it is absolutely impossible to neglect medical recommendations. You need to see a doctor not only for yourself, but also for those around you. After all, measles is an infectious disease that can quickly reach epidemic proportions. In addition, complications may arise due to improper self-medication.
When treating at home, the patient should be visited by a local doctor every few days. A complicated form of measles requires treatment in a hospital. If a concomitant infection occurs, antibiotics are prescribed.