Myofascial syndrome. Fragment of Dr. Vlasenko’s interview with the Neuromir-TV channel
There is an expression: “The spine is the key to health.” We won’t deny this, but we shouldn’t hold the spine responsible for all back pain either. After all, anatomically, the back also consists of ribs, shoulder blades, various ligaments and many muscles. And even without the help of the spine, they are capable of causing truly hellish torment, which can really be mistaken for symptoms of a herniated disc or radicular syndrome.
Take muscle spasms, for example. It is believed that muscles make up about 45% of our body. Therefore, it is not surprising that muscle spasms can occur literally anywhere and at the same time cause severe pain. By the way, any woman who has given birth will confirm this. After all, pain and contractions during childbirth are nothing more than a spasm of the muscles of the uterus. The uterus consists of muscles that are the strongest in a woman's body. Another striking example of muscle pain is muscle tension headache. Here, as you can see, already in the name itself there is an indication of the cause of pain - muscle tension.
I give these examples only so that you, dear reader, take a look at the question “Why does my back hurt?” from a new point of view. Although, in fact, there is nothing new in it, you just might not have known before that the culprits of back pain are most often not displaced vertebrae and discs, but muscle spasms. And to be completely precise - spasms of individual fibers in the muscles of the back, neck or lower back. By the way, this is convincingly evidenced by both statistical data and modern scientific research.
“What about osteochondrosis and disc herniation?” - you ask. And no one canceled them. Only the role of osteochondrosis and hernias in the occurrence of pain is greatly exaggerated. There is convincing evidence of this. See for yourself:
If the patient complains of back pain, an MRI is performed and osteochondrosis or disc herniation is detected. The patient is treated and the pain goes away. But, if you do a second MRI, it turns out that both osteochondrosis and the disc herniation remain in the same place. So why did my back hurt? The explanation for this is quite simple - they were not the culprits of the pain. And if we look at the statistics again, we find out that the cause of back pain in 75–85% of cases is muscle spasms. And a hernia and osteochondrosis may be present, but never bother a person!
Muscle pain. What is myofascial syndrome?
Let's start with the word "syndrome". It is almost synonymous with the word “disease.” The only difference is that the symptoms of the disease have a common mechanism of development and a common origin. But the symptoms that make up the syndrome have only a common development mechanism, and their origin is different. It's easier to understand with an example. All symptoms of salmonellosis have a common origin - they are caused by Salmonella bacteria. Therefore, salmonellosis is a disease. But the symptoms of myofascial syndrome have different origins: impaired neuromuscular conduction, overload, fatigue, stress, metabolic disorders, sedentary lifestyle, bad habits, injuries, etc. That is why myofascial syndrome is called “syndrome”.
Now - “myofascial”. This word consists of two words: “myo” - muscle and “fascia” - the muscular sheath that covers every muscle in our body. Muscles and fascia are inseparable from each other: they work together and get sick together. And they should also be treated together. Let’s agree right away: for simplicity, we will not say “muscles and fascia,” but simply “muscles.” But, in fairness, let’s start with the fascia.
Fascia is a muscular sheath that sometimes shortens, similar to how clothes shrink when washed improperly. This happens for various reasons, for example, from a sedentary lifestyle or from injury. As a result of such shortening, the fascial sheath becomes tight, it compresses the muscle - and the muscle, under the influence of this tightness, has to reflexively contract. As soon as muscle compression reaches a certain force, the muscle automatically pinches the nerve endings, veins and arteries that pass through it. But the most important thing is that the tightened muscle can no longer contract normally. Consequently, the tight muscle will work worse and weaken.
This pathological process is called musculofascial shortening . Under the onslaught of this pathology, the body will adapt to increasing pathological changes and maintain independent defense as long as it has enough strength. All this time, healthy muscles will take on the load, compensating for all the shortcomings. However, even healthy muscles will not be able to withstand the overload indefinitely, so they will also begin to weaken and shrink. Thus, the pathological process, spreading from one muscle to another, will gradually cover the entire musculature of the back and limbs. First, this will change your posture, then it will overload the spine, leading to the formation of intervertebral hernias and protrusions. And finally, having exhausted the possibility of compensation, the body will give “SOS” signals - the occurrence of pain. This is what myofascial syndrome looks like.
We are used to thinking that pain occurs because a person lifted a heavy object, “rested” his neck, or sharply bent over. But that's not true. The listed circumstances only transfer the disease into the open phase.
Common mistakes when treating back pain
Many people, when they first feel pain in the back or in another part of the body, make desperate attempts to “treat” it with exercises. This happens under the influence of the prevailing opinion about “pumping up” the muscle corset. This point of view is rather naive. It does not take into account that a sore muscle requires treatment, not stress. It wouldn’t occur to anyone to treat pain at the time of a sprained or broken leg by running - “limp, but run.”
Treatment and rehabilitation should not be confused. The difference between these two concepts is huge. Treatment is the fight against the disease, and rehabilitation is making up for lost time while the person was sick. Replacing the treatment process with rehabilitation is a very short-sighted step. After all, rehabilitation exercises are not just physical education. They are called restorative precisely because they should be performed at the last - restorative stage of treatment, after the disease has subsided. But under no circumstances during acute or subacute periods, when the disease is at its peak! Otherwise, there is a great danger of overstraining the body’s compensatory forces, which are already at their limit.
Another common misconception is the “repositioning” of vertebrae. An inexperienced patient encountering back pain for the first time most often expects that everything will be “quickly corrected” for him and that will be the end of the matter. How far from the truth he is! After all, by the time pain appears, the balance between most muscles has already been disturbed. And if you compare the spine and muscles with the mast and ropes, it becomes clear that unevenly and asymmetrically tensioned ropes can easily warp the mast.
Usually, when examining patients, the asymmetry of many muscles is clearly visible. For example, the left muscle groups pull on the right ones, the front muscles are more tense than the back ones, and the deep ones are more tense than the superficial ones. It is as a result of this that our “mast” becomes warped. Therefore, if we limit ourselves to “repositioning” the vertebrae without properly relaxing the muscles, then the tense back muscles will “displace” the vertebrae again and again. Therefore, first of all, it is necessary to return the muscles to their normal state, freeing them from tension. And only then “straighten” the vertebrae and “pump up” the muscle corset. But most often, after the muscles relax, the vertebrae themselves “fall” into place, receiving the long-awaited freedom.
Results and discussion
MPS is not a local phenomenon, as follows from studies of the state of the neuromuscular junction, individual muscle fibers of human skeletal muscles and the morphofunctional organization of motor units in the myofascial trigger zone. It is generalized in nature with sequential involvement of trigger zones, caused by neuromuscular dysfunction of the CP of extrafusal muscle fibers.
In fact, the muscle suffers primarily, and not due to morphological or functional disorders of other structures of the peripheral neuromotor apparatus. The conclusion is formed taking into account the following theoretical foundations.
Since normally the electrical activity of the muscle at rest is not recorded, with the exception of the background activity of the CP zone when small intramuscular nerve terminals are stimulated by the tip of the electrode, a thorough analysis of the EMG activity of the CP zone was carried out in order to differentiate it from the pathological spontaneous activity of muscle fibers [14]. The absence of spontaneous pathological activity both in the zone of active and in the zone of latent MTZ is an indication that the innervation of muscle fibers in the muscle under study is not impaired. The introduction of a needle electrode into the MTZ was accompanied by background activity of the CP zone, while in the active trigger zone low-amplitude wave-like noise of the CP with single high-amplitude intermittent spikes predominated. KP noise can objectify MTS, but is not an absolute diagnostic criterion for MBS. The high frequency of recording CP noise in MTS allowed a number of authors [9, 15] to suggest that background activity is generated by altered motor CPs. Experimental studies indicate that CP noise-like potentials represent vigorous pathological PC activity. CP noise and spikes are the result of an excessive increase in the rate of spontaneous release of acetylcholine from the nerve terminal of the motor CP [16], which is destroyed mechanically or biochemically [17].
If we interpret the observed background local changes in EMG as pathological activity of motor CPs, then the pathogenic focus leading to the formation of MTS can be localized in the area of a small number of abnormally functioning motor CPs. In accordance with this, one can expect a positive effect from the administration of botulinum toxin type A (BTA), which blocks abnormal motor CPs, with subsequent branching, growth of new motor terminals and the development of new normal CPs, which is confirmed by a series of studies, which will be discussed below.
The study of motor units (MU) of skeletal muscles through the analysis of their potentials (MU) revealed the presence of MU in the active myofascial trigger zone, the duration of which exceeded the limits acceptable for a healthy muscle ± 30%, while most of the MU was somewhat shortened. This resulted in a decrease in the mean normalized duration compared to the control group mean. Changes in the parameters of the MUAP in MTZ in patients with MPS are characterized by a slight decrease in amplitude, an increase in the number of phases and turns in the potentials and their spike part.
A study of patients with MPS revealed an increase in the average duration of the spike component of the MUAP. It is known that the restructuring of the MU, which increases the concentration of MV in the electrode lead zone (located in the center of the MU) with elimination to the periphery, leads to an increase in the duration of the spike component in the potentials of normal parameters. Even a slight “desynchronization” of the potentials of individual MV MU leads to an increase in the number of turns, reflecting the number of individual MVs involved in the formation of the spike component of the MU [18]. Already at the very early stages of the development of the pathological process in certain areas of the muscle, the concentration of MV in one motor unit increases, which is confirmed by the number of turns of the spike part of the potential in the active MTZ. The average value of the parameter under discussion in the active myofascial trigger zone is increased by 2 times compared to the norm (Fig. 1) .
Rice. 1. Histogram of the distribution of muscle fiber density in the myofascial trigger zone before and at various periods after the administration of botulinum toxin type A.
The dotted line indicates normal values (1.48, SD 0.3).
Fig. 1. Histogram of muscular fiber distribution density in myofascial trigger zone before and within different periods after type A botulinum toxin injection.
The dashed line indicates reference values (1.48, SD 0.3).
A series of studies carried out revealed an increase in the density of MVs of active and latent MTZ. Multiple thinned individual MVs with local shortening of sarcomeres in the form of “contraction nodules” are located between normal MVs in the area of muscle compaction. In the compacted area of the muscle of the myofascial trigger zone, an increase in the number of MVs with “contraction nodes” is observed, which leads to a shortening of the distance between individual MVs. Thus, excessively contracted sarcomeres contribute to the formation of compaction in the contraction zone [5, 12].
Of interest is the identified correlation between changes in the density of MV in the MU and the number of turns of the commissure part of the MU at various stages of the denervation-reinnervation process in a series of studies after the introduction of BTA into the MTZ of the horizontal portion of the upper part of the trapezius muscle (Fig. 2) . The initial mean value of MV density in the MTZ, measured in conventional values, was 2.05, SD 0.26. At the same time, the average number of turns of the spike part of the MU had a very similar value and amounted to 2.05, SD 0.69. These indicators were statistically significantly higher than the initial indicators in healthy subjects (1.48±0.3 and 1.30±0.4, respectively; p<0.01).
Fig. 2. Changes in the density of muscle fibers of the motor unit and the number of turns of the spike part of the potential recorded in the myofascial trigger zone before and at various periods after the administration of botulinum toxin type A.
MF - muscle fibers; MPU - motor unit potentials.
Fig. 2. Changes of muscle fiber density and the number of turns of the main spike in myofascial trigger zone before and within different periods after type A botulinum toxin injection.
One week after BTA administration, no changes in CF density were observed. By the end of the first month after administration of the drug, a decrease in both the number of turns and a decrease in the density of MVs in the MTZ were recorded; after 4 months, an increase in the analyzed parameters was observed, followed by their stabilization and return to the original value. A strong correlation was revealed between the value of the MV density and the number of turns of the commissure part of the MUAP. This once again confirms the possibility of indirectly judging the density of MVs in the motor unit by only analyzing the number of turns of the spike component during a standard EMG examination. A year after administration of the drug, there was a tendency toward restoration of MV density (1.6, SD 0.27), but the indicator was statistically significantly lower than the initial value and comparable to the indicators recorded in the muscle of healthy subjects.
As the analysis of clinical data showed, the positive dynamics of the patients’ condition appeared by the end of the first week after the administration of the BTA drug, and by the end of the first month, restoration of muscle tissue density was recorded and the trigger phenomenon was almost leveled out. There was no relapse in the studied muscles within 6 months. Only in a number of patients under the influence of unfavorable factors, primarily postural overload and emotional stress, the formation of latent MTZ in this area was observed. With the additional influence of methods for correcting the motor stereotype, it is possible to increase the interval of action of the drug to a year and it is quite acceptable to refuse repeated use.
The identified background local changes in EMG, reflecting the pathological activity of motor CPs, make it possible to localize the focus to the zone of a small number of abnormally functioning motor CPs. In accordance with this, the long-lasting effect of BTA when using small doses is quite explainable. Moreover, local administration of small doses of BTA directly into the MTZ made it possible to avoid rapid diffusion, clinically manifested by generalized muscle weakness and neurophysiologically - active denervation, which is usually observed when BTA is administered in a relatively large volume into the motor point of the muscle [19].
It is known that the action of BTA associated with the blockade of cholinergic innervation entails a reversible decrease in muscle hyperactivity, decompression of sensory endings and vessels with the cessation of nociceptive afferentation and restoration of blood circulation in the MTZ.
The state of blood flow in the MTZ was assessed during an ultrasound examination of 50 patients (average age 41.67±11.86 years, average disease duration 3.32±2.56 years) with painful muscle spasm in the cervical and lumbar spine due to myofascial pain syndrome [20]. The prospects of ultrasound diagnostics of MTZ for the clinic in order to identify the area of compaction and the possibility of accurately inserting a needle into muscle tissue during local injection therapy are mentioned in the works of S. Sikdar et al. [21]. Local muscle compaction is characterized by point and linear hyperechoic inclusions in the connective tissue structures of the muscle, disrupting the continuity of the fascicular lines; echogenicity increases as the degree of fibrosis increases [6]. An ultrasound scan of the myofascial trigger zone allowed not only to locate the MTZ, but also to assess the state of blood flow in the myofascial trigger zone. In the examined patients, a developing or formed hyperechoic, less often an isoechoic trigger zone (from 4×5×3 to 15×4×3 mm or more) with isolated inclusions of calcium was visualized. Color Doppler imaging showed reduced vascularization in all patients compared to nearby muscle areas. Peripheral blood flow was located at the base of the zone with a linear blood flow velocity of no more than 10-15 cm/s. In some cases, power Doppler ultrasound did not reveal signs of blood flow (avascularization). Thus, patients with MBS experience intramuscular hypoperfusion, and its result is hypoxia in the myofascial trigger zone.
It is known that patients with occupationally caused trapezius myalgia had a deficiency of cytochrome C oxidase, which suggests an energy crisis within the muscle. This finding correlates with reports of low ATP and ADP levels in individuals with trapezius myalgia. A high degree of mitochondrial dysfunction and a decrease in the number of blood capillaries were also noted in the muscles [11]. Data support the concept of an ischemic-induced energy crisis in the development of muscle pain.
A repeat ultrasound was performed 10 days after local injection therapy, which was carried out with the aim of muscle relaxation of the trigger zone, elimination of ischemia and, as a result, pain relief. The drug used was tolperisone hydrochloride, prescribed to treat painful muscle spasms or spasticity.
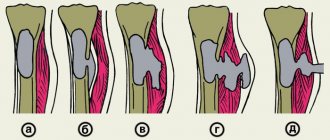
The muscle relaxant effect of the drug tolperisone hydrochloride is realized by inhibiting the presynaptic release of neurotransmitters from the central terminals of afferent fibers due to the combined effect on voltage-gated sodium and calcium channels. In addition to its effect on muscle tone, the drug tolperisone hydrochloride can improve peripheral circulation, which is explained by the blockade of adrenergic receptors located in the vascular wall [22, 23]. 10 days after the administration of a therapeutic dose of the drug tolperisone hydrochloride, normalization of the muscle structure was observed in the MTZ, and the area of compaction became more diffuse. Color Doppler imaging showed moderate hypervascularity compared with the previous study. Peripheral arterial blood flow was located with a linear blood flow velocity of more than 30 cm/s, central blood flow - 5-7 cm/s; in some cases, signs of pronounced “neovascularization” of the muscle were recorded. Ultrasound data with restoration, and sometimes resumption of blood flow, made it possible to substantiate the pathogenetic direction of the use of the drug tolperisone hydrochloride in MTZ (Fig. 3) .
Rice. 3 . Ultrasound examination of the upper portion of the trapezius muscle.
a - before local administration of the drug tolperisone hydrochloride; a formed hyperechoic trigger zone with single inclusions of calcium measuring 15×4×3 mm is located; with color Doppler mapping, peripheral blood flow is located at the base of the zone with a linear blood flow velocity of 11 cm/s; b - 10 days after local administration of the drug tolperisone hydrochloride; normalization of the muscle structure is detected, the trigger zone has become more vague, color Doppler mapping detects peripheral blood flow with a linear blood flow velocity of 30-40 cm/s, and central blood flow of up to 5 cm/s is recorded.
Fig. 3. Ultrasound examination of the upper trapezius muscle.
a — prior to local injection of Tolperisone hydrochloride; hyperechoic trigger zone with single calcium inclusions 15×4×3 mm is visualized; peripheral blood flow is observed at the base of this zone with a linear blood flow velocity of 11 cm/s during Doppler mapping; b — 10 days after local injection of Tolperisone hydrochloride; muscle structure normalization, trigger zone has become vaguer, peripheral blood flow with a linear blood flow velocity of 30—40 cm/s is visualized during Doppler mapping, central blood flow up to 5 cm/s is observed.
The study of MU potentials, their spike component and analysis of MV density in the study of latent MTZ revealed changes of a similar nature, but less in degree of manifestation than those recorded in active MTZ. This confirms the structural rearrangement of the motor unit in the zone of both active and latent trigger. Often latent MTZs are recorded in the corresponding muscle of the contralateral side. Perhaps their formation is facilitated by the central mechanisms of signaling triggering sprouting. Latent MTS exists at the stage of evolution, which is subsequently transformed, under negative influences, into an active state with a corresponding set of symptoms.
From the point of view of clinical practice, the differentiation of active and latent MTZ is rather arbitrary, since they are successive stages of a single pathological process and require timely pathogenetic therapy. It should be noted that compactions within the muscle or dense cords are the primary response of the muscle to metabolic or physical stress, and the dominant factor in the development of areas of muscle compaction is ischemia. Areas of local muscle compaction have their own characteristics that differ from intact muscle tissue. MTZs are permanently tense, their tissue can further sharply contract due to mechanical irritation, for example, when pinched or pricked with a needle.
It has been experimentally shown that neuromuscular dysfunction of the MTP area is associated with changes in the state of the motor CP [9]. Absence of spontaneous activity of muscle fibers, registration of spontaneous activity of the PC and its inactivation by the introduction of BTA, analysis of MUAP parameters (decrease in amplitude, shift of the histogram of MUAP distribution over duration towards smaller values and a large proportion of polyphasia due to an increase in the number of turns), as well as an increase in the density of muscle fibers MTZ of human skeletal muscle is characterized by structural and functional changes in the state of the muscle, which prove the reorganization of motor units with predominant damage to the muscle substrate in the area of the motor CP with excessive acetylcholine activity.
An electron microscopic examination of the MTZ of the trapezius muscle showed atrophic changes in the form of destruction of myofibrils, leading to their thinning and an increase in interfibrillar spaces (Fig. 4) . Similar changes have been described, in particular, in experiments with exhaustive physical exercise [24, 25]. Individual myofibrils lost their integrity due to the splitting of sarcomeres, as well as the loss of part of the contractile proteins of the sarcomeres. The identified divergence of myofilaments and Z-lines (Fig. 5) may be associated with the destruction of myofibril cytoskeletal proteins, including the possibility of mechanical separation of actin filaments from the Z-line as a result of the breaking force on the muscle, which is initially in a spasmodic state. Structural abnormalities in the trapezius muscle in chronic myalgia in the form of altered myofibrils, as well as uneven distribution of mitochondria within the fiber with frequent accumulation under the sarcolemma and the absence of a Z-disc in the area, combined with the presence of “moth-eaten” and torn red fibers (identified by light microscopy ) may be a consequence of impaired microcirculation with local hypoxia or ischemia and local muscle overload [26, 27]. The appearance of autophagosomes in the area of muscle compaction (Fig. 6) may be associated with muscle atrophy as a result of inadequate load or with a violation of neurotrophic control, which is reflected in the works of F.A. Khabirov [28].
Rice. 4. Electron micrograph of the myofascial trigger zone of the trapezius muscle.
Thinning of myofibrils, expansion of interfibrillar spaces; destruction of myofibrils; in the interfibrillar spaces and at the site of destroyed myofibrils there are round or oval-shaped mitochondria with indistinct cristae with a slightly cleared matrix (magnitude 13,000).
Fig. 4. Electron microscopic image of myofascial trigger zone of trapezius muscle.
Thinning of myofibrils, enlargement of interfibrillary spaces; destruction of myofibrils; rounded or oval mitochondria with uneven crista and light matrix are visualized within interfibrillary space and destructed myofibrils (13,000-fold magnification).
Rice. 5. Electron micrograph of the myofascial trigger zone of the trapezius muscle.
Individual sarcomeres in the center are destroyed, the contact of actin filaments with the Z-line is not visible. The myofibrils at the ends of the sarcomeres diverge, forming “fan-shaped” structures. The interfibrillar spaces are expanded (magnitude 16,650).
Fig. 5. Electron microscopic image of myofascial trigger zone of trapezius muscle.
Destruction of several sarcomeres, no attachment of myofilaments to Z-line. Myofibrils diverge at the ends of sarcomeres (“fan-shaped” structures). Enlarged interfibrillary spaces (16,650-fold magnification).
Rice. 6. Electron micrograph of the myofascial trigger zone of the trapezius muscle.
Autophagosome in the area of the cell nucleus (magnitude 14,000).
Fig. 6 . Electron microscopic image of myofascial trigger zone of trapezius muscle.
Autophagosome near cellular nucleus (14,000-fold magnification)
Thus, short-term excessive load against the background of prolonged static tension, especially in a non-physiological position, can cause the development of acute or exacerbation of chronic myofascial pain. It should be noted that prolonged static load itself contributes to overload and overstretching of muscles. In this case, we can talk about the activation of pain receptors, that is, nociceptive pain. The average time for recovery and relief of nociceptive pain does not exceed 2-3 weeks, which, undoubtedly, should be taken into account when developing a set of therapeutic measures for patients with MPS.
An integrated approach to the treatment of MBS includes impact on all levels of the formation of a “vicious circle”: the prescription of analgesics, muscle relaxants, anxiolytics with a vegetative-stabilizing effect, antidepressants, impact on the involved muscle with MTZ (stretching, massage, heat, reflexology, compresses with dimexide and anesthetics) and local injection therapy. The most important aspect of treating myofascial pain is restoring the length and elasticity of the affected muscles, which is best achieved through muscle stretching exercises (post-isometric relaxation).
Treatment of myofascial pain with an injection into the MTZ (muscle relaxant, anesthetic, or dry needling) results in apparent softening of the tight band. In the complex therapy of MBS, local injections specifically into the MTZ are more effective than conventional intramuscular administration of drugs.
Our study on the use of a peripheral muscle relaxant - botulinum toxin type A - in patients with MBS demonstrated a positive effect on electrophysiological parameters reflecting the functional state of the peripheral neuromotor apparatus. The positive clinical effect significantly alleviated the patients’ condition and made it possible not to use any drugs from a huge number of pharmacological agents and manual aids for a long period [19].
Since the tolperisone molecule is similar to the lidocaine molecule, the drug has a local anesthetic effect along with a muscle relaxant, and due to its blocking effect on α-adrenergic receptors, it causes a vasodilating effect. This became the basis for using the drug as a local injection therapy for MBS [29]. The effectiveness and safety of local use of the drug tolperisone hydrochloride in patients with MBS is confirmed by its positive muscle relaxant and analgesic effect. This also contributed to the restoration of peripheral blood circulation in the MTZ, which is confirmed by the results of ultrasound examination. A significant analgesic effect of the drug when administered into MTZ appeared on the 3rd day, the maximum relaxing effect of therapy was noted on the 10th day [20].
The most important part of the treatment process for myofascial pain is rehabilitation with the formation of new “memory” of previously damaged muscles through neuromuscular learning. Thanks to this, the vicious circle of spasm-ischemia-pain-spasm is broken and a normal motor stereotype is formed. A carefully selected physical activity program becomes the basis for subsequent functional recovery of muscles in MBS.
Symptoms of myofascial syndrome
It happens that different diseases have similar symptoms, for example, pain. Speaking about myofascial syndrome, we do not forget that there are disc herniations, osteochondrosis and other diseases. After all, it often happens that a person has two or three diseases at the same time, and in different stages. For example, inactive disc herniation and exacerbation of myofascial syndrome. Therefore, it is important to distinguish what exactly is bothering the patient at the moment. Therefore, in order to truly cure a disease, it must first be recognized among the jumble of active and inactive symptoms.
Symptoms of myofascial syndrome are:
- trigger points;
- areas of referred pain;
- numerous vegetative disorders.
Now let's look at each of them separately.
Stages of disease development
The development of the disease, its course, as a rule, goes through three stages:
- Due to a number of reasons, active pain points appear. The muscles begin to contract involuntarily. There is severe pain that appears and disappears randomly.
- At the second stage, pain occurs only at the moment of impact on the affected muscle. When the muscles are at rest, there is no trigger activity.
- It becomes unimaginably difficult to move, because... the disease becomes chronic. The affected area may hurt during exposure to it, or may be in a calm state. It is impossible to understand when new spasms may occur.
Trigger points
Myofascial syndrome originates in the thickness of the muscles with microscopically small muscle spasms. Gradually, the spasm zone reaches a size that is significant for the microcosm. The number of such areas increases, they become denser and become incredibly painful. They are called trigger points - from the English word “trigger”, which in this case denotes the mechanism that triggers myofascial pain syndrome.
Please note that trigger points are a specific symptom inherent only(!) to myofascial syndrome. Trigger points fundamentally distinguish myofascial syndrome from all other diseases: osteochondrosis, disc herniation, etc.
Treatment of trigger points at the Spina Zdorova clinic is carried out according to the American method of gentle manual therapy, described in the book by Travel and Simons “Myofascial pain and dysfunction.”
If you accidentally discover similar painful points in different parts of your body, then the likelihood of myofascial syndrome is very high. But two other symptoms will help to make sure of this.
TREATMENT WITH SHOCK WAVE THERAPY
Today there are many treatment options, but the fastest and most effective modern physiotherapeutic method is shock wave therapy. Recent studies conducted in European countries indicate the highest effectiveness of shock wave therapy with no side effects.
| The points of impact of shock waves during myofascial pain are diverse, which leads to a rapid break in the vicious circle of pain and spasm. UVT improves local blood circulation and lymphatic drainage at the level of small vessels, which helps remove accumulated algogenic substances (causing pain) and inflammatory mediators. Local metabolism also improves, which leads to a decrease in the degree of oxygen starvation in the muscle. |
Shock wave therapy has an excellent antispasmodic effect, which is achieved both through mechanical stimulation of the muscle and reflex action through the peripheral nervous system due to the effect on mechanoreceptors of pressure and vibration. SWT will not only be able to cure, but also use trigger points to diagnose whether there are any other diseases.
UVT sessions do not require any preliminary preparation, are non-invasive (no injections or other violations of the integrity of the skin are required) and are well tolerated by patients. The clinical effect occurs quite quickly, often already during the procedure itself!
Therapy will allow the patient to reduce the frequency of taking analgesics, and subsequently completely abandon them. At the moment, shockwave therapy in the treatment of myofascial syndrome is the most effective. We will save you from pain!
The course of treatment includes 3-5 UVT procedures with an interval of 5-7 days. The use of shock wave therapy allows you to quickly relieve pain and eliminate muscle spasms, thereby enabling the patient to get rid of excruciating pain, stiffness of movement and significantly improve the quality of life.
Areas of referred pain
Referred pain is like a sunbeam falling on a wall. Although the wall glows, any adult understands that it is just a reflection of the sun. Likewise, reflected pain is felt far from the place where its true source is hidden. Referred pain can manifest itself in different ways: both independently and simultaneously with pain at the trigger point itself.
It is impossible to catch the sunny “bunny” until you cover the mirror. Referred pain cannot be eliminated if you do not know where its true source is. The great success is that each trigger point has its own strictly defined “pattern” of the pain zone - a pain pattern. This correspondence allows the chiropractor to accurately find the true sources of pain and effectively eliminate them.
Classification and clinical picture
MPTTs are classified as active and latent trigger points. An active trigger point is a point with spontaneous pain or pain in response to movement that can provoke local or referred pain. A latent trigger point is a sensitive point with pain or discomfort that appears only in response to compression.
Active or latent MPTTs are subject to the following clinical characteristics.
- Pain with compression. Compression may cause local pain and/or referred pain, similar to the patient's typical complaints, or may worsen existing pain.
- Local reaction in the form of twitching. Palpation with crunching (rapid compression through muscle fibers) can cause a local twitching reaction, which is manifested by rapid contraction of muscle fibers in or around the site of tension.
- Muscle tension. Limited range of stretch and increased sensitivity to stretch at the site of tension can lead to tightness in the muscles involved.
- Local myasthenia. The muscle with the trigger point may be weak, but usually there is no atrophy.
- Patients with trigger points may have associated local autonomic phenomena, including vasoconstriction, pilomotor response, and hypersecretion.
Autonomic dysfunction
All processes that support both the life of the organism and its work are called vegetative. This includes breathing, nutrition and excretion, sleep and wakefulness, heating the body in the cold and cooling in the heat, and much more. Any disruption of these processes is usually called autonomic dysfunction.
In simple cases of myofascial syndrome, autonomic dysfunction is subtle. It is manifested by swelling of the sore spot, change in skin color or impaired sweating. But when myofascial syndrome is expressed strongly or for a long time, then autonomic dysfunction acquires very striking features. Morning stiffness, dizziness, nausea, sometimes vomiting, stuffy ears, a lump in the throat and anxiety appear. General weakness, fatigue, irritability, depression, bad mood and tearfulness, insomnia at night and drowsiness during the day, absent-mindedness and memory loss occur. Disturbances in the functioning of internal organs are common: abdominal pain, palpitations, lack of air. Headaches, feeling of squeezing of the head, torso or limbs.
However, patients associate all of the listed autonomic disorders with anything, but not with muscles. Therefore, people turn to a chiropractor as a last resort, thereby allowing the disease to spread its influence.
OUR DOCTORS:
| Lopatko Dmitry Nikolaevich | Neurologist, chiropractor, hirudotherapist, reflexologist, kinesiologist Neurologist of the highest category. Proficient in treatment methods in the following areas: manual therapy, applied kinesiology, osteopathy, homeopathy, reflexology. He successfully applies his knowledge in the treatment of pain syndromes associated with diseases of the musculoskeletal system, pathology of internal organs and psycho-emotional disorders. He has his own experience in the treatment and diagnosis of neurodental diseases. Author of patent for invention No. 2010153976 / 14 – (078049) “Method of therapeutic effects of transcranial magnetic stimulation for prosopalgia.” A specialist with more than 25 years of experience. Took training and master classes with prof. Vasilyeva L.F. Joseph, Shafer, Christopher Smith, David Leaf, Jose Palomar. |
| Zhimolostnov Andrey Vasilievich | Physiotherapist, shock wave therapy specialist, chiropractor, podiatrist (specialist in the manufacture of custom insoles) Provides treatment and prevention of diseases of the musculoskeletal system, chronic diseases of the ENT organs, and many others using various physiotherapeutic methods. Graduated from Krasnoyarsk State Medical Institute, internship. He completed advanced training in “Endoscopy in Pediatrics” at the Novokuznetsk State Institute for Advanced Training of Physicians. Also completed the courses “Children’s Infectious Diseases”, “Current Issues in Pediatrics”, “Neonatology”, “Pulmonology in Pediatrics”, “Doctor of Rehabilitation Medicine”, Krasnoyarsk State Medical University, “Physiotherapy”, at the State Scientific Center of the Russian Federation - Federal Medical Biophysical Center named after A.I. Burnazyan. Works with patients of all ages. |
Causes of muscle pain. What are the causes of myofascial syndrome?
Lifting weights, hypothermia, negative emotions. What connects all these factors and muscle pain?
Acute muscle overload
.
As a rule, if back pain occurs due to lifting, bending, awkward movement or injury, then it does not raise questions, its causes are so obvious. There is also chronic muscle overload
, and it occurs due to scoliosis, poor posture or monotonous posture, for example, with a sedentary lifestyle. However, we will discuss chronic muscle overload, due to its dominant pathological effect on the body, separately.
Metabolic disorders
. This includes overweight, hormonal deficiency, anemia, low levels of hemoglobin, vitamins, calcium, sodium and iron. In addition, various toxins have a fatal effect on metabolic processes: from viral and microbial (remember the muscle aches in the body during a cold), ending with the toxic products of smoking, alcohol or drugs. In general, any intoxication seriously disrupts the nutrition of muscle cells, leading to overexertion and the development of myofascial syndrome.
Another cause of pain is hypothermia
. It is the muscles that produce heat in the body. It’s not without reason that when actively moving, a person becomes hot, and when frozen, he shivers from the cold. Shivering is the extremely intense work of muscles to produce heat. Severe hypothermia can cause overload, leading to pathological tension and painful myofascial syndrome.
Emotional disturbances.
Let's focus on this reason. Do you know why? Because most people are not aware of the connection between emotions and muscles, and this connection is so significant that it cannot be neglected! And since we are talking about emotional stress, we need to understand that in a big city, even the most conflict-free and healthy lifestyle is associated with mental depression. Artificial light, street noise, lack of sleep and other factors in the metropolis catastrophically overload the sympathetic system, which serves as a starter for muscle overstrain. Emotional overload is a significant and very significant reason that increases pathological muscle tension - take this into account when analyzing your pain.
And finally, let’s name the most common, and perhaps the main cause of myofascial syndrome. It's called muscle imbalance
.
Pathophysiology
The initial muscle changes associated with myofascial pain seem to lead to the further development of a tension zone, which in turn is a movement abnormality. Several mechanisms have been put forward to explain this motor abnormality, the most accepted of which is the "Integrated Hypothesis", first developed by Simmons and later expanded by Gerwin.
Simmons' integrated hypothesis is a six-link chain that begins with abnormal release of acetylcholine. This causes an increase in muscle fiber tension (formation of a tension zone). The tension zone is thought to reduce blood flow, leading to local hypoxia. Decreased oxygen levels disrupt mitochondrial energy metabolism, reducing ATP, and leading to tissue distress and the release of sensitizing substances. These sensitizing substances lead to pain when nociceptors are activated and also lead to autonomic modulation, which then enhances the first step: abnormal acetylcholine release.
You can read about pain mechanisms here.
Gerwin expanded on this hypothesis by adding more specific details. He stated that the activity of the sympathetic nervous system increases the release of acetylcholine and that local hypoperfusion caused by muscle contraction (tight rim) leads to muscle ischemia or hypoxia, which in turn leads to a decrease in pH ("acidification" of the environment).
Prolonged ischemia also leads to muscle damage, which promotes the release of potassium, bradykinins, cytokines, ATP, and substance P, which can stimulate nociceptors in the muscles. The end result is the tenderness and pain seen in MPTT.
Depolarization of nociceptive neurons causes the release of calcitonin gene-related peptide (CGRP).
CGRP inhibits acetylcholinesterase, increases acetylcholine receptor sensitivity and acetylcholine release, leading to SEA.
In recent studies, Shah et al. confirmed the presence of these substances using microdialysis methods at trigger points. Increased levels of substance P, protons (H+), CGRP, bradykinin, serotonin, norepinephrine, TNF (tumor necrosis factor), interleukins and cytokines have been found in active trigger points compared to normal muscle or even latent trigger points. The pH of the active trigger point region decreased to 4 (normal value is 7.4), causing muscle pain and soreness, as well as decreased acetylcholinesterase activity, which led to prolonged muscle contractions.
Chronicity factors
In some cases, there may be “chronization factors” that have a direct effect on myofascial pain. These factors can chronicize pain and tenderness, playing an important role in the widespread distribution of pathological symptoms through central sensitizing mechanisms.
Mechanical factors
- Scoliosis.
- Difference in leg length.
- Hypermobility of joints.
- Excessive use of muscles.
Systemic or metabolic factors
- Hypothyroidism.
- Iron deficiency.
- Vitamin D deficiency.
- Vitamin C deficiency.
- Vitamin B12 deficiency.
Psychosocial factors
- Stress.
- Anxiety.
Other factors of chronicity
- Infectious diseases.
- Parasitic diseases (eg Lyme disease).
- Polymyalgia rheumatica.
- Use of drugs from the statin class.
In some cases, correction of the identified chronicity factor can lead to complete elimination of pain and may be the only therapeutic approach needed to relieve the patient's symptoms.
Muscle imbalance. Chronic muscle overload is the main danger
What is muscle imbalance? The balance between which muscles is disturbed with it? There is an opinion that muscle imbalance is a violation between the so-called opposing antagonist muscles, that is, flexor and extensor, anterior and posterior, deep and superficial. But in reality, muscle imbalance is an imbalance between the phasic and tonic muscles.
According to their functions, the muscles of our body are divided into two groups. Some perform a movement and are called motor, dynamic, or phasic. Others hold the pose, counteracting the gravitational forces of the earth's attraction and the pressure of the atmosphere on us. These muscles are called postural-tonic, tonic, or postural. During movement, all muscle groups work. For example, when walking, the motor muscles “go”, and the postural-tonic muscles keep the body vertical. Therefore, the workload of both groups is distributed evenly and balanced. When a person is motionless, for example, sitting, then only his tonic muscles work, and his motor muscles are inactive.
The life of a modern person is deprived of movement. Today, since childhood, static and monotonous poses have prevailed. And if we add to this poor posture and scoliosis, which in themselves are a static overload, then the scale of the problem becomes obvious. Static monotony forms a fatigue overstrain of the tonic muscles, which causes them to shrink and become “woody,” while the motor muscles, on the contrary, become decrepit from prolonged inactivity.
It is this ratio, when the tonic muscles are overloaded with work, and the motor muscles are relaxed from idleness, that is usually called muscle imbalance.
Sooner or later, muscle imbalance leads to the appearance of local muscle spasms. Having begun due to chronic muscle overload, spasms intensify under the influence of “second-order” causes. What aggravates the problem is that a person cannot feel muscle imbalance, unlike injury, heaviness or hypothermia. The invisibility of the initial stage of the disease allows it to take deep roots and spread its sprouts everywhere.
Diagnostics
Palpation is the gold standard in determining the presence of an area of muscle tension. This involves training and developing the precise skills of specialists to identify these stress areas.
Palpation of tension areas requires precise knowledge of muscle anatomy, the direction of specific muscle fibers, and muscle function.
Muscle palpation must meet several basic criteria and supporting observations to identify the presence of trigger points.
Main criteria
- Tension zone (where muscles are accessible).
- Presence of a place of pain in the tension zone.
- Reproduction of symptoms upon palpation.
- Pain occurs when a muscle is stretched (limited range of motion).
Supporting Observations
- Visual or tactile response to local twitching.
- The patient reports pain when pressing in the tension area.
- SEA was confirmed by electromyography.
Over the past few years, the reliability of palpation has been the subject of scientific debate. Recent studies have seen improvements in methodological quality, but the main problem is the lack of blinding. This is a problem that is difficult to solve because the reliability of palpation depends on the level of competence of the specialist.
Recent studies have shown interesting results using magnetic resonance elastography. The technique involves injecting cyclic waves into the muscle and then using phase contrast imaging to identify tissue distortions. Wave speed is determined from graphic images. Shear waves travel faster in stiffer tissues. And then the tension zone can be distinguished from the surrounding normal muscles.
Another recent method used to confirm dilatation of MPTT areas is sonoelastography combined with Doppler imaging.
It uses a clinical ultrasound imaging system with a linear resolution of 12-5 MHz coupled to an external vibration source (handheld vibration massager) operating in cycles of approximately 92 Hz. Doppler imaging is used to identify surrounding blood flows.
Ballyns et al showed that sonoelastography can be a useful tool for classifying MPTT into regions. Larger areas correspond to active trigger points, and smaller areas correspond to latent trigger points.
It is noted that this method requires preliminary manual palpation of trigger points.
Effective treatment for muscle pain. Manual treatment of myofascial pain syndrome
How to restore lost balance to muscles? This task, although difficult, is quite realistic. Manual treatment and moderate physical activity will provide them with a full and high-quality recovery. And it doesn’t matter what you do: swimming, Pilates, exercise machines or physical therapy, the main thing is that the sports load does not exceed your physical fitness and is performed at the appropriate time.
Note! The cause of 90% of back pain is myofascial syndrome.
For any disease, there are basic, auxiliary and restorative treatment methods. You can’t do without the main ones, the auxiliary ones enhance the effect of the main ones, and the restorative ones help restore the body. Purely theoretically, the best result will be obtained by a simultaneous combination of all effects, but in practice this will result in either very troublesome or unreasonably expensive treatment. Therefore, the most rational choice remains the main method, supplemented, if possible, by auxiliary ones. And here the question arises, what method of treatment of myofascial syndrome should be considered the main one? To understand this, we will give a brief description of the most common methods.
Drug treatment. When a painful attack occurs, it can grow like an avalanche, activating more and more new trigger points. Therefore, if you do not have a better option now, then by all means take the medicine. The most commonly used drugs are analgesics, non-steroidal anti-inflammatory drugs (NSAIDs) and muscle relaxants. Remember, as an axiom, pain cannot be tolerated.
Some people ignore any pill because of possible side effects. But no medicine in the world can compare with the “side effects” of pain. Because even minor but constant pain is a stress factor. It seriously depletes and suppresses the nervous system. It may seem surprising, but the word “depression”, in Latin “depressio”, means real depression. In other words, even mild but prolonged pain gradually suppresses the nervous system, forming somatoform depressive states, the inevitable consequence of which is the consolidation and fixation of the pain itself. A vicious circle is created: muscle tension - pain - muscle tension.
The disadvantages of drug treatment for myofascial syndrome are that it cannot be used for a long time. Therefore, with pronounced, widespread and prolonged muscle tension, the final effectiveness of medications is low; they simply do not have enough time and power to free the muscles from tension and overcome the disease.
Acupuncture. It’s a good way to relax your muscles, but finding an intelligent specialist is a rare success; there are only a few of them. Therefore, most often the cost of acupuncture exceeds its effectiveness. Health is not something that can be frivolously experimented with using extravagant treatments, especially when there are correct and affordable solutions. This is my opinion.
Physiotherapy for pain and therapeutic exercises for pain are auxiliary types of treatment. At the right moment, they fully justify the tasks assigned to them. However, if physical therapy is prescribed prematurely, then the likelihood of a new exacerbation of pain is very high. During treatment at the Spina Zdorova clinic, the doctor will recommend the necessary exercises for you. The best option is Pilates classes.
Manual treatment of myofascial pain syndromes rightfully deserves the highest ratings. Human hands are the softest, most sensitive, skillful... in general, the most “tool” in every sense. It is not for nothing that “handmade” has always been considered a sign of good quality and high quality. Judge for yourself, how can a pill “straighten” a vertebra? But manual therapy can. Relieve muscle tension and pain, eliminate joint blocks - you never know what else can be done by human hands and manual therapy. Of course, there are diseases that are more effectively treated with devices, medications or a scalpel, but the treatment of myofascial pain syndromes is the undisputed leader of manual therapy.
At the Spina Zdorova clinic we use all methods of soft manual therapy:
1
relaxation / PIR
Provides preliminary muscle relaxation and guarantees complete safety of subsequent effects. We start each session with PIR.
2
mobilization
Eliminates blocks and restores mobility of the spine and joints. Using gentle movements, it gently corrects the neck, spine, joints of the arms and legs.
3
inhibition
Causes an amazing effect of muscle relaxation and reliably eliminates pain.
4
recoil
Very soft local impact with variable amplitude for correction of vertebrae and joints.
5
facilitation
The doctor fixes the patient in special positions, thereby eliminating pain and severe strain.
6
Myofascial release
Frees muscles and vertebrae from clamps, thanks to which they painlessly “fall into place.”
The most effective method of manual therapy for combating myofascial syndrome is considered myofascial release , from the English word “release” - release, deliverance. This is a proven method that allows you to very efficiently and gently release muscles from tension, healing a person.
The qualifications of the doctors at the Spina Zdorova clinic allow us to freely use these and other methods for the treatment of myofascial syndrome. In addition, in each specific case, we combine them, taking into account the synergy effect.
What is synergy? Synergy is not just a heap of different effects, it is the correct sequence in the combination of methods. Synergy leads to additional quality of treatment. An example from life is our hands. How long does it take to fasten a button? Seconds?! And if you do it with one hand, you may not be able to do it in a minute. That is, to act with two hands is not twice as fast as with one, but many times faster. Is there a difference between listening to the same music performed by individual instruments or by the whole orchestra together? This is the effect of synergy - it makes it possible to do everything much more powerfully, efficiently and quickly, but at the same time more carefully. This also applies to treatment at the Spina Zdorova clinic.
Diagnosis
The clinical diagnosis of myofascial pain depends in principle on the physician, who can suggest this cause as a possible cause to explain the nature of the pain. Myofascial pain syndromes can be similar to a large number of other diseases, so adequate evaluation is necessary. Myofascial pain is characterized as a non-intense, deep sensation of pain, which intensifies with the work of the muscles involved and stress, which increases muscle stiffness. A characteristic clinical feature of myofascial pain is the detection of a trigger point. This is a clear focus of local pain within the muscle. Sometimes pain on palpation can spread and reproduce the patient's symptoms. But as a rule, the irradiation of pain does not follow the same paths as the cutaneous innervation of the root. Palpation usually reveals a rope-like condensation of muscle fibers, often called a “taut ligament.” Sometimes, quickly flicking this ligament or piercing a trigger point with a needle will lead to a spasmodic contraction of the affected muscle. This convulsive reaction can only be detected in superficial muscles. Myofascial pain often follows muscle injury or repetitive strain. Often in modern clinics numerous expensive examinations were carried out before a diagnosis of myofascial pain was made. Some patients with a clear cause of musculoskeletal pain (eg, rheumatoid arthritis) may develop myofascial pain syndrome that goes undiagnosed as there is an underlying disease. Myofascial pain has certain clinical features that help in making this diagnosis. The pain is typically described as a deep aching sensation, often with a feeling of stiffness in the area involved; this is sometimes seen as joint stiffness. Myofascial pain increases with use of the affected muscle, stress, exposure to cold, or postural imbalance. Radiation from the trigger point may be described as paresthesia, thus being similar to symptoms of radiculopathy (lumbar or cervical). Muscle weakness that occurs due to its low load can lead to symptoms such as fatigue, poor coordination of movements, and sleep disturbances. Patients with myofascial pain involving the muscles of the neck and face may experience symptoms of dizziness, tinnitus, and static disturbances.
Characteristics of a myofascial trigger point:
- Focus of pain on palpation of the affected muscle
- Reproduction of a complaint of pain when palpating a trigger point (with a force of about 3 kg)
- Palpation reveals induration (hardening) of the adjacent muscle
- Limited range of motion in the affected muscle
- Often pseudo-weakness of the muscle involved (without atrophy)
- Often referred pain with prolonged (~5 seconds) pressure on the trigger point.
Prevention of myofascial syndrome
To avoid relapses, you must first get rid of the disease completely. And then reduce the risk factors. Create comfortable conditions for sleeping and working. Watch your weight and eat right. Keep up your physical activity. But the main thing is do not neglect your health and do not skimp on it. Don't let things take their course. After recovery, try to do at least one maintenance session of gentle manual therapy once every three to six months - this will help to significantly reduce risk factors. Remember: your health comes first!