Diverticula are pouch-like protrusions on the walls of the intestine. In a third of all cases, these formations are found in the sigmoid colon, and a little less often in the esophagus and duodenum. Colon diverticulosis is most common in men and women over 40 years of age, but there are cases of congenital diverticulosis.
In certain situations, the disease leads to serious complications that cannot be eliminated without surgery.
general description
Diverticular disease of the colon is a chronic disease in which pouch-like protrusions through the muscle layer form in the wall of the large intestine.
The protrusions themselves form in weak spots of the intestinal wall, where blood vessels pass through it. Typically, the size of diverticula varies from 5 to 10 mm. Diverticular disease includes:
- Diverticulosis - the presence of several diverticula in the intestine
- Diverticulitis - inflammation of the diverticulum
The prevalence of the disease among young people is very low - about 2-5%, with obese men most affected. With age, the risk of developing the disease increases and by the age of 70-80 reaches 65%. Up to 70 years of age, the incidence among men prevails over women.
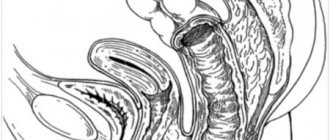
Intestinal diverticula
Treatment of patients with an uncomplicated form of diverticulosis is carried out in the gastroenterology department, and in case of severe complications - in a surgical hospital. Patients with acute or exacerbation of chronic diverticulitis, intoxication, high fever, severe concomitant pathology, impossibility of enteral nutrition, as well as those over 85 years of age are hospitalized. If there is a clinic with an acute abdomen, an urgent operation is performed.
Conservative treatment
If a patient is accidentally diagnosed with an asymptomatic intestinal diverticulum, no special treatment is required. In the presence of uncomplicated diverticula, a diet rich in fiber, antispasmodics, and prokinetics are prescribed. If all recommendations for treatment of the disease are followed, a lasting clinical effect is usually achieved. If the patient has developed diverticulitis, the use of intestinal antiseptics, antibiotics, and osmotic laxatives is recommended.
To normalize intestinal function, cleansing enemas and uncontrolled use of laxatives should be abandoned. A positive effect is also achieved when moderate physical activity is introduced into the daily routine - they help strengthen the muscular corset of the torso and normalize intestinal motility. To reduce pressure in the intestinal lumen, a diet rich in fiber is prescribed (except for very coarse fibers - pineapples, persimmons, turnips, radishes). The amount of fiber in the diet is increased to 32 g/l. It is necessary to exclude gas-forming foods, legumes, and carbonated drinks. To achieve the desired effect, you should drink at least two liters of water daily.
The use of stimulant laxatives and morphine-based painkillers for diverticula is contraindicated, as they provoke further impairment of intestinal motility and aggravate the course of the disease. To improve the passage of food masses through the intestines, osmotic laxatives are prescribed - they increase the volume of feces and accelerate their movement through the digestive tract. For diarrhea, sorbents and astringents are prescribed, and simethicone preparations are prescribed to relieve flatulence.
Acute diverticulitis requires hospitalization of the patient in a surgical hospital, the appointment of detoxification and plasma replacement agents, and antibacterial drugs. Treatment lasts at least two to three weeks; after discharge from the hospital, maintenance therapy is similar to that carried out for uncomplicated diverticula.
Surgery
Surgical treatment is indicated for the development of life-threatening complications: perforation, abscess formation, intestinal obstruction, profuse bleeding, fistula formation. Also, planned surgery is prescribed for recurrent bleeding and diverticulitis. Usually, a part of the intestine affected by diverticulosis is resected and an anastomosis is performed. In difficult situations, a colostomy is performed to facilitate the outflow of feces, and after stabilization of the condition, reconstructive surgery is performed.
Causes
The main causes of diverticular disease are:
- Dystrophic changes in the muscle wall of the large intestine
- Changes in her motor skills, weakness of the muscle component
- Impaired blood supply to the intestinal wall and the development of atherosclerosis with ischemic changes
Increased intraintestinal pressure due to prolonged spasm, leading to divergence of muscle fibers.
Diverticula are the final manifestation of intestinal wall disease, atrophy and expansion in sloping areas.
There are some prerequisites for the development of diverticula in the colon:
- the presence of an outer muscle layer in the form of three stripes, helping to weaken the intestine before external and internal influences
- the presence of haustra, in which increased intraintestinal pressure is generated
Diagnostic methods
To more accurately determine the symptoms and prescribe treatment appropriate to the disease, a comprehensive diagnosis is carried out. It includes an external examination and instrumental studies.
When palpating the abdomen, diverticulosis is indicated by swelling and tenderness of the large intestine, especially in the left side, while there is no tension in the anterior abdominal wall.
Instrumental diagnostics for suspected diverticulosis include:
- intestinal irrigoscopy (x-ray using a contrast agent);
- colonoscopy;
- computed tomography or virtual colonoscopy;
- plain radiography of the abdominal organs.
Additionally, ultrasound diagnostics of the abdominal organs is prescribed. This study is carried out to exclude pathologies that are accompanied by symptoms similar to diverticulosis.
During diagnosis, it is important to exclude intestinal cancer or detect hidden diseases such as hemorrhoids, anal fissures, intestinal polyps and others. No less useful is information about the localization of formations in the large intestine and their current condition: the presence or absence of inflammation, bleeding, etc.
Complications
The development of the disease is fraught with abscess formation, and the abscess can break into the abdominal cavity. The subsidence of symptoms does not in all cases lead to the final resorption of the infiltrate; in this case, hardening of the mesentery and surrounding tissues occurs, which can result in a tumor of the abdominal cavity.
Repeated attacks of diverticulitis can lead to adhesions of the intestine with neighboring organs. Here the abscess has the ability to open into the bladder, vagina, urethra, small intestine, and fistulas are formed. However, perforation of a sigmoid colon diverticulum into the free abdominal cavity can have quite tragic consequences, since peritonitis develops and rapidly progresses.
Intestinal bleeding in this disease cannot be called profuse, however, it is so pronounced that it is quickly noticed by both the patient and doctors. Its hidden forms usually manifest themselves in anemia. Since it is quite difficult to recognize the causes of all these symptoms, a comprehensive study is used. In addition to the clinical manifestations of the disease, the results of essential X-ray and endoscopic examinations are also taken into account.
How to make an appointment with a gastroenterologist
You can make an appointment with a gastroenterologist at Meditsina JSC (academician Roitberg’s clinic) on the website - the interactive form allows you to select a doctor by specialization or search for an employee of any department by name and surname. Each doctor’s schedule contains information about visiting days and hours available for patient visits.
Clinic administrators are ready to accept requests for an appointment or call a doctor at home by calling +7 (495) 775-73-60.
Convenient location on the territory of the central administrative district of Moscow (CAO) - 2nd Tverskoy-Yamskaya lane, building 10 - allows you to quickly reach the clinic from the Mayakovskaya, Novoslobodskaya, Tverskaya, Chekhovskaya and Belorusskaya metro stations .
They say you shouldn’t eat sunflower seeds or popcorn—it all gets stuck in the diverticula.
This is an old theory that has been completely refuted by modern research. American scientists observed 47,000 people who, during a routine examination between the ages of 40 and 75 years, were not found to have any diseases of the colon or diverticula. Participants filled out questionnaires about their condition and talked about their diet every 2 years for 18 years. It turned out that diverticulitis and bleeding from diverticula occurred with the same frequency in people who did not eat nuts, popcorn and seeds, and in people who ate well. Moreover, those who ate nuts twice a week were not only less likely to see doctors for diverticulitis because of diverticulitis than people who ate nuts only once a month.
Risk factors
Before you learn how to treat diverticulitis, it is worth addressing the risk factors. In this case, these include the already mentioned heredity, age, as well as poor nutrition and lifestyle, which contribute to impaired peristalsis. For example, people who sit a lot, hardly move, and have weak muscles are at risk. Many people hardly associate sports and peristalsis, but developed abdominal muscles really help the intestines to function properly. But you can’t get too carried away with heavy sports - otherwise there will be a backlash.
We also include anyone who does not follow the drinking regime into the risk zone - without a sufficient amount of moisture, the contents of the intestine become too dense, which can cause damage to its walls. Those who abuse bad habits, do not follow basic hygiene rules and do not take good care of their health are also in danger.
Which doctor should I contact?
Diverticulosis is a gastrointestinal disease, and treatment is most often carried out by a gastroenterologist. The primary task of the doctor is:
- Excluding diagnoses with similar symptoms;
- Purpose of examination;
- Determining a strategic approach to treatment.
During the treatment process, you may need to consult other specialists: a proctologist, a surgeon, a therapist, a pediatrician and geriatrician, an endoscopist and a nutritionist.
Prevention
Among preventive measures, a varied and balanced diet is of primary importance. Due to the fact that a diet low in plant fiber predisposes to the formation of diverticula, in order to reduce the risk of developing the disease, it is necessary to include large quantities of plant-based products. Since timely detection of diverticula plays an important role, it is extremely important to undergo preventive examination and regularly perform endoscopic examination of the intestine.
Diet
Since diverticular disease occurs much more often in people who limit their intake of vegetables and fruits, all patients with diverticulosis need to use foods high in plant fiber and pectin. Wheat bran (especially coarse bran) is very useful, which significantly reduces the pressure inside the intestine and accelerates the rate of movement of contents through the intestines.
It is imperative to exclude all foods that cause increased gas formation (legumes, lentils, grapes, sauerkraut, butter and yeast dough, onions) and constipation (blueberries, rice). It is also advisable to exclude seeds, fruits with a large number of grains and excessively coarse fiber (persimmons, pineapples, turnips, radishes, radishes).
Drug treatment
- In uncomplicated cases, the disease does not require the use of medications. The need to take medications depends on the clinical manifestations.
- For abdominal pain, antispasmodics are used.
- If dysbiosis is detected, drugs are used that help restore normal intestinal microflora.
- For persistent constipation, take medications to enhance gastric and intestinal motility: lactulose preparations, petroleum jelly or olive oil orally or in microenemas.
- For diverticulosis with clinical manifestations of inflammation, it is necessary to use the entire range of therapeutic measures: a laxative diet, antispasmodics; drugs that regulate intestinal motor function, and agents that normalize the composition of the intestinal bacterial flora.
Folk remedies
The following folk remedies are recommended to help normalize stools and restore intestinal function:
- Carrot seed powder (to do this, you need to thoroughly grind the carrot seeds and consume this powder several times a day (2-3), with a sufficient amount of water - 200-300 ml).
- Sauerkraut brine or radish juice (drink a few tablespoons after meals, 1-2 times a day).
- Infusion of aloe leaves (approximately 150 g of crushed leaves, pour 300 g of honey, leave the resulting mixture for 24 hours, strain and take a tablespoon an hour before meals).
- Flaxseed oil 1 tablespoon on an empty stomach daily.
- Mint tea (add 2-3 mint leaves to regular tea).
Chronic diverticulitis
Patients with chronic diverticulitis remain with persistent clinical symptoms despite standard treatment (pain in the left lower quadrant). It is considered atypical if systemic symptoms never develop. With systemic symptoms, chronic disease may manifest as a recurrent, intermittent acute illness or as a persistent illness with mild symptoms. It is often associated with cellulitis. If an infection occurs, inflammatory changes in the preparation will be visible.
Indications for surgical treatment for the acute phase of the disease
Indications for surgical intervention in acute illness include:
In an emergency requiring surgical intervention, simple disconnection with fecal diversion from the damaged segment of the colon, disconnection with suturing of the perforation site, obstructive resection (Hartmann operation) or with a mucous fistula (Mikulich operation) can be used. Additional measures include performing a thorough lavage of the abdominal cavity on the operating table.
In the acute setting, discussions of similar operations in the past have included a three-stage approach with disconnection, drainage, followed by a second-stage resection and a third-stage restoration of colonic continuity by anastomosis.
A modification of this approach involves suturing the visible area of perforation with tamponade of this area with an omental flap - as a primary operation. Alternatives consist of a two-stage approach consisting of a Hartmann or Mikulicz procedure followed by a second operation to restore intestinal continuity and resection with primary anastomosis, with or without a proximal protective stoma, in a single operation. For most cases, the entire debate revolves around the relative benefit of performing one-stage versus two-stage procedures in the acute phase requiring emergency surgery. The three-stage approach is least likely to be used unless the patient is extremely medically unstable.
Anatomy of the colon
The colon consists of the following sections: cecum, ascending colon, transverse colon, descending colon, sigmoid colon. The cecum has the widest lumen, and the sigmoid colon has the smallest. The junction of the sigmoid colon and the rectum is designated as the rectosigmoid junction. It is important to note that this section of the intestine has the narrowest diameter.
The wall of the colon consists of three layers: serous, muscular and mucous. The function of the mucous membrane of the colon is the absorption of water, the formation of feces, preparing them for evacuation by secreting a large amount of mucus and the synthesis of vitamins B and K. Under the epithelium of the colon mucosa there is a submucosa, represented by loose fibrous connective tissue in which blood vessels and lymphatic vessels and submucosal nerve plexus.
The muscular layer has a frame function and is responsible for the progressive movement of feces to the rectum. The muscular layer consists of a continuous inner circular layer, divided into three ribbons of the outer longitudinal layer.
The serous membrane consists of a connective tissue base covered with mesothelium, into which outgrowths of adipose tissue, the so-called fat pads, penetrate from the muscular layer.
Forecast
The prognosis is usually favorable if the disease is detected in a timely manner and the necessary preventive and therapeutic measures are started, provided that the patient follows all the necessary recommendations. However, if the need for prevention is ignored, diverticular disease can lead to the development of severe complications that threaten the life and health of the patient. Moreover, the disease is more common among older people who have a variety of concomitant diseases and lower body resistance.
Classification of diverticular disease
- Uncomplicated.
This form is detected accidentally during an X-ray or endoscopic examination of the intestine. Blood tests usually show no changes. The examination must be carried out to assess the extent of intestinal damage, prognosis of the course of the disease and the choice of a method for preventing complications or treatment. - Complicated
, occurring with an acute inflammatory process (diverticulitis, diverticular infiltrate, diverticulum perforation, abscess, peritonitis), a chronic inflammatory process, as well as bleeding. A chronic process includes situations when inflammation cannot be eliminated within 6 weeks, or it occurs again. In severe cases, an infiltrate, narrowing of the intestine, or a fistula from a destroyed diverticulum may form.
Treatment of chronic diverticulitis and recurrent diverticulitis.
Most patients who report a first episode of diverticulitis symptoms have been symptom-free for at least 1 month before the onset of the disease. Most of them were helped simply by diet and outpatient antibiotic treatment. At least 10% of patients with a first episode of diverticulitis who respond to outpatient treatment will have a recurrence of the disease or continuation of symptoms that require hospital treatment. Then 20% or more of these patients will have a relapse of the disease. Some, but not all, will require readmission to the hospital.
The interval between acute episodes of inflammation can be extended to 5 years. After the second hospitalization, more than 70% of patients continue to suffer from these symptoms, and more than half of them require another hospitalization within the next year. The more severe the attack of inflammation, the more likely the disease will relapse.
Patients with multiple, repeated episodes of acute diverticulitis confirmed on CT should be candidates for surgery with colon resection.
Traditional training of doctors in tactics for diverticulitis dictates that patients who have more than 1 episode of uncomplicated diverticulitis undergo resection of the sigmoid colon. In fact, most data on resection performance were published before the introduction of CT scanning and modern antibiotics into clinical practice. Because of this and other studies, the American Association of Colorectal Surgeons has revised previous recommendations regarding resection for diverticulitis. The parameters of the 2006 revision are as follows: “the decision to recommend surgical treatment should depend on the age and general medical condition of the patient, the frequency and severity of attacks of diverticulitis, and whether persistent symptoms of diverticulitis persist after an acute attack or not.”
Symptoms of diverticulosis
The uncomplicated form of the disease is accompanied by the following manifestations:
- Painful spasms - on the left or below, in the middle of the abdomen, sharp or aching;
- After eating, the pain intensifies, but after a while it goes away on its own;
- If the protrusions are in the sigmoid colon, the pain may resemble appendicitis;
- The pain may spread to the anus, sacrum and lower back, to the buttocks and groin;
- After bowel movement or gas release, the pain stops.
The disease is accompanied by the following symptoms:
- Chronic constipation, which may be followed by diarrhea;
- A lot of mucus is released from the anus;
- A person experiences a false urge to defecate;
- Foul gas, bloating;
- After defecation, there remains a feeling of incomplete emptying of the intestines.
Diverticulosis can be asymptomatic for a long time, but in some cases an inflammatory process develops. In this case, complications are possible:
- Intestinal obstruction;
- Internal bleeding;
- Accumulation of infiltrate;
- Fistulas inside and outside;
- Perforation - when perforation occurs, purulent processes are possible.