The brain is protected from external mechanical influences by the cranium. The most important sections are located at the bottom of the skull. The gray matter of the brain contains 25 billion neurons, which is almost 4 times the population of the globe (6.5 billion). The human brain is covered by three membranes:
- vascular (web-like),
- soft,
- hard.
In the area of the brain there are five ventricles - containers connected to each other by channels. Inside the cavities there is cerebrospinal fluid - a biological fluid that circulates both in the cisterns of the brain and in the spinal canal.
What is the brain, encephalon, its meaning?
The brain is the anterior part of the central nervous system. Brain
located in the cranial cavity, it interacts with the human body (men, women) with the external environment, integrating the functioning of all body systems.
The brain has the ability to assimilate, organize, store, and retrieve information about past experience. The brain is the material substrate of higher nervous activity. Phylogenetically, the brain is the anterior end of the neural tube. Ontogenetically, the brain is a derivative of the cerebral vesicles, from which parts of the brain are formed: the telencephalon, the diencephalon, the midbrain, the hindbrain, which is represented by formations such as the pons, cerebellum, and medulla oblongata. The cavities of the brain vesicles develop into the ventricles of the brain.
Risk factors
Brain diseases can be caused by various reasons related to lifestyle, as well as existing health problems.
- Smoking. Nicotine and other substances contained in tobacco smoke provoke atherosclerosis and vascular aneurysm at a high rate.
- Low physical activity. Physical education improves the plasticity of the brain - its ability to create new connections and transform itself. Accordingly, if a person does not perform even minimal exercise, his brain does not create new neural connections and quickly destroys old ones.
- Male gender. According to research, men are more likely to suffer from brain diseases because they lead an unhealthy lifestyle.
- High blood pressure. As a result of surges in blood pressure, protrusion of the vessel wall in a weak spot may occur.
- Poor nutrition and obesity. If a woman’s waist exceeds 88 cm, and a man’s waist exceeds 102, it is necessary to adjust your diet. With obesity, insulin insensitivity develops (cells lose sensitivity to the hormone, and the pancreas produces more of it than normal).
- Alcohol. The alcohol contained in alcoholic drinks is absorbed into the blood, enters the brain and destroys its cortex.
- High cholesterol. It affects blood vessels, forming cholesterol plaques on their walls, interfering with normal blood flow.
- Stress. Recent studies have shown that stress impairs brain function due to the production of cortisol (the stress hormone).
- Age. Many diseases begin to appear younger and appear at an earlier age than decades ago. For example, cholesterol plaques begin to form in the blood vessels of the brain by the age of 35, which can lead to atherosclerosis.
- Genetics. If your close relatives have developed brain diseases under 50 years of age, then you are at high risk.
- Infections and inflammations. They affect the brain matter, disrupting the functioning of the immune system and brain.
Brain structure
The cerebrum, or telencephalon, is represented by two hemispheres, which are connected to each other by the corpus callosum, corpus callosum. It consists of nerve fibers running transversely from one hemisphere to the other. The corpus callosum ensures the unity of functioning of both hemispheres. When the corpus callosum is cut, each hemisphere of the brain begins to function independently of each other. Under the corpus callosum is the fornix, fornix. Anterior to the pillars is the anterior commissure, comissura anterior. Between the anterior part of the columns of the fornix and the knee of the corpus callosum there is a thin vertical plate of brain tissue - the transparent septum. Between the plates of the septum there is a slit-like cavity that does not have an ependymal lining. A number of authors call it the 5th ventricle.
The surface of the hemispheres is covered with a layer of gray matter - this is the cerebral cortex. Underneath it is the white matter and subcortical nuclei: striopallidal system, extrapyramidal system.
If you make a horizontal section of the brain through the cerebral hemispheres at the level of the thalamus and subthalamic nuclei, you can see the following formations: pineal body, superior colliculus, thalamus, frenulum, posterior limb of the internal capsule, globus pallidus of the lenticular nucleus, putamen of the lenticular nucleus, lateral sulcus, fence , anterior part of the internal capsule, head of the caudate nucleus, column of the fornix, anterior horn of the lateral ventricle, genu of the corpus callosum, septum pellucidum, interthalamic commissure, lentiform nucleus, external capsule, extreme capsule, convolutions of the insula, lateral sulcus, internal capsule, subthalamic nucleus, tail caudate nucleus, lateral geniculate nucleus, red nucleus, gray matter of the superior colliculus, cerebellar vermis.
Brain of a newborn, children, child, human: structure, anatomy
The brain of a newborn baby is shorter and wider than that of school-age children and adults. It is devoid of all tertiary and a number of secondary grooves. By the end of the child’s first year of life, the brain increases in size by 2–2.6 times. By 3 years it increases 3 times. From birth to adulthood, brain weight increases 4 times, and body weight increases 21 times.
The mass of the right hemisphere is most often greater than the mass of the left hemisphere. After birth, the parietal and frontal lobes develop most intensively. And because of this, the overall configuration of the brain changes. Unlike the adult brain, in a newborn the neurons of different layers are located closely next to each other, because of this, the radial striation of the cortex may be absent. Single neurons may be located in the subcortical white matter. In the substantia nigra of the brain stem, neurons do not yet have the pigment melanin, which usually appears by 3–4 years of age. Up to 3–6 months of extrauterine life, the outer embryonic layer, which is called “Obersteiner’s layer,” remains in the cerebellar cortex. Obersteiner's layer consists of medulloblasts and spongioblasts. The surface of the inferior olives of the fetal medulla oblongata is smooth. After the birth of a child, the olives acquire elevations and then noticeably increase in size with age. Almost always in newborns, immature cellular elements are found in the subependymal parts of the ventricular system of the lateral ventricles, the presence of which erroneously resembles manifestations of Virchow's local encephalitis. Immature cells are located in the subependymal layer diffusely or in the form of separate foci. Sometimes they can be traced along the blood vessels over a significant extent of the white matter. By 3–6 months of a child’s life, these cells gradually disappear. The presence of a large number of immature cells in the subependymal parts of the ventricular system is an additional morphological sign of fetal prematurity.
Brain and spinal cord
Spinal cord
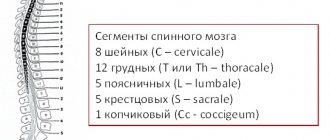
It is a nerve cord lying in the spinal canal formed by the vertebrae. Extends from the foramen magnum to the lumbar spine. At the top it passes into the medulla oblongata, at the bottom it ends with a conical point with a terminal filament.
The spinal cord is covered by several membranes: dura mater, arachnoid and pia mater. Between the arachnoid and soft membranes, cerebrospinal fluid circulates - cerebrospinal fluid, which surrounds the spinal cord and takes an active part in the metabolism of the spinal cord.
In cross section, the spinal cord (SC) resembles a butterfly. In the center is the gray matter, consisting of the cell bodies of neurons. At the periphery there is white matter, which is formed by the processes of neurons.
In the gray matter of the SC, there are two anterior projections (anterior horns), two lateral ones (lateral horns) and two posterior ones (posterior horns). In the next article we will study reflex arcs, so this knowledge will be very useful to us. The horns of the gray matter contain neurons that are part of the reflex arcs.
Numerous nerve fibers approach the posterior horns of the spinal cord, which unite to form bundles - the dorsal roots. Numerous nerve fibers emerge from the anterior horns of the spinal cord and form the anterior roots.
The white matter consists of numerous nerve fibers, bundles of which form cords. The spinal cord pathways are divided into ascending - from receptors to the brain, and descending - from the brain to effector organs. 31 pairs of spinal nerves arise from the spinal cord.
The spinal cord has two important functions:
- Reflex
- Conductor
Due to the bodies of neurons, which are located in the gray matter of the spinal cord and are part of the reflex arcs that provide reflexes.
Due to the presence of white matter in the spinal cord, which includes numerous nerve fibers that form bundles and cords around the gray matter.
Brain and its parts
We move on to the study of the human brain, the complex main organ of the central nervous system, located in a reliable bone container - the skull. The average brain weight ranges from 1300 to 1500 grams.
Let me note that the weight of the brain has nothing to do with intellectual abilities: for example, Albert Einstein’s brain weighed 1230 grams - less than that of the average person. Intelligence is rather determined by the complexity and ramification of the neural networks of the brain, but not by mass.
The human brain is divided into five sections: medulla oblongata, posterior (pons and cerebellum), middle, intermediate and terminal. The most ancient sections - the medulla oblongata, posterior and middle - form the brain stem, which resembles the structure of the spinal cord. Sometimes the intermediate section is also referred to as the brainstem. 12 pairs of cranial nerves arise from the brain stem.
The telencephalon differs from the structure of the brain stem; it is a huge accumulation (about 16 billion) of neurons that form the cerebral cortex (CCH). Neurons are arranged in several layers, their processes form thousands of synapses with other neurons and their processes. The centers of higher nervous activity - memory, thinking, speech - are located in the KBP.
We begin a fascinating journey through the parts of the brain. It is fundamentally important for you to separate and remember the functions of the various departments; for this, be sure to use your imagination!)
- Medulla
- Hindbrain (pons and cerebellum)
- Midbrain
- Diencephalon
- Finite brain
The most ancient part of the brain. Remember that it regulates vital functions: the cardiovascular system, respiratory and digestive processes. The centers of protective reflexes - vomiting, sneezing, coughing - are concentrated here.
The pons Varoliev performs a conductive function: all descending and ascending nerve pathways pass through the bridge. It also controls the work of the facial and chewing muscles of the face and the lacrimal gland.
The cerebellum has its own hemispheres connected to each other. The cerebellar cortex is formed by gray matter, the subcortical nuclei are surrounded by white matter.
The cerebellum takes part in the coordination of voluntary movements, helps maintain body position in space, regulates tone and balance. Thanks to the cerebellum, our movements are clear and smooth.
In the midbrain there are the superior (anterior) and inferior (posterior) tubercles of the quadrigeminal. The upper tubercles of the quadrigeminal are responsible for the visual orientation reflex, and the lower ones are responsible for the auditory orientation reflex.
What is the visual orientation reflex expressed in? Imagine walking into a dark room. In her corner the screen shines comfortably, the website (of course) Studarium is visible =) And then the visual orientation reflex begins: You move your eyes, turn your head in the direction of the source of intellectual light. At the same time, do not forget to regulate the size of the pupil and the accommodation of the eyes - all this is a visual orientation reflex.
The auditory orientation reflex is also necessary for us. It’s good if, while reading the textbook now, you are in silence. Suddenly your phone starts ringing: you immediately stop reading and head towards the source of the sound - the phone. Thanks to this orienting reflex, we can determine the location of the sound source relative to us (left, right, behind, in front).
The midbrain also performs a conductor function and is involved in the regulation of muscle tone and body posture.
Let me remind you that the hypothalamus we studied, the associated pituitary gland, pineal gland and thalamus belong to the diencephalon. You know that the hypothalamus controls the pituitary gland, the conductor of the endocrine glands, therefore the functions of the hypothalamus are: regulation of the metabolism of proteins, fats and carbohydrates, as well as water-salt metabolism.
In addition, the hypothalamus controls the sympathetic and parasympathetic systems, regulates body temperature, and is responsible for sleep-wake cycles. The hypothalamus contains the centers of hunger and satiety.
Consists of subcortical structures and cerebral cortex (CBC). The surface of the KBP reaches an average of 1.5-1.7 m2. Such a large area is due to the fact that the CBP forms convolutions - elevations of the brain matter, and grooves - depressions between the convolutions.
Cerebral cortex
The cortex has several layers of cells, between which numerous branched connections are formed. Despite the fact that the cortex functions as a single mechanism, its different parts analyze information from different peripheral receptors, which I.P. Pavlov called the cortical ends of analyzers.
The cortical representation of the visual analyzer is located in the occipital lobe of the CBP; it is in connection with this that, when falling on the back of the head, a person sees “sparks from the eyes” when the neurons of this lobe are excited mechanically, as a result of the impact.
The cortical representation of the auditory analyzer is located in the temporal lobe of the cerebral cortex.
Remember that the cortical representation of the motor analyzer - the motor zone - is located in the anterior central (precentral) gyrus, and the representation of the skin analyzer - the sensory zone - is in the posterior central (postcentral) gyrus.
Think about it! When making any voluntary (conscious) movement, a nerve impulse arises precisely in the neurons of the precentral gyrus, from where it begins its long journey through the brain stem, spinal cord and finally reaches the effector organ.
Impulses from skin receptors reach the neurons of the postcentral gyrus - the sensory department, thanks to which we receive information from them and are aware of our own sensations.
The number of neurons in these convolutions allocated for different organs is not the same. Thus, the projection area of the fingers of the hand takes up a lot of space, making fine movements of the fingers possible. The projection area of the torso muscles is much smaller than the area of the fingers, since the movements of the torso are more uniform and less complex.
The areas of the brain that we studied, in which the transformation and analysis of incoming information occurs, are called associative zones of the CBP. These zones connect different parts of the CBP, coordinate its work, and play a crucial role in the formation of conditioned reflexes.
Our conscious activity lies within the framework of the cerebral cortex: any conscious movement, any sensation (temperature, pain, tactile) - everything has representations in the CBP. The cortex is the basis for communication with the external environment and adaptation to it. QBP also lies at the foundation of the thinking process. In general, you understand how highly you should value it and how well you should know this topic 
You've probably heard that the right and left hemispheres are functionally different. The left hemisphere contains the mechanisms of abstract thinking (language abilities, analytical thinking, logic), and the right hemisphere contains the mechanisms of concrete figurative thinking (imagination, parallel processing of information). With injuries or damage to the left hemisphere, speech may be impaired.
Diseases
Depending on the level of damage to the spinal cord during trauma, the picture of neurological disorders manifests itself differently. The higher the level of damage, the more nerve pathways are “cut off” from the brain. So, for example, with a lumbar injury, arm movements are preserved, but with a cervical injury, arm movements are impossible.
Sometimes after a stroke (bleeding in brain tissue) or injury, paralysis (complete lack of movement) develops on one side of the body. Knowing the anatomy, you can conclude: if movements are lost in the right arm and leg, then the stroke occurred on the left.
Why does this pattern exist? The fact is that the nerve fibers running from the precentral gyrus to the working organs - the muscles - form the so-called physiological cross at the border of the medulla oblongata and the spinal cord. That is, to put it simply: part of the nerves that came from the left hemisphere pass to the right side and vice versa - nerves from the right hemisphere pass to the left side.
© Bellevich Yuri Sergeevich 2018-2021
This article was written by Yuri Sergeevich Bellevich and is his intellectual property. Copying, distribution (including by copying to other sites and resources on the Internet) or any other use of information and objects without the prior consent of the copyright holder is punishable by law. To obtain article materials and permission to use them, please contact Yuri Bellevich
.
How does a child's brain mass change with age?
If you monitor how the mass of a child’s brain changes depending on age, you will notice the following picture. If the child’s age is from 3 to 8 days, body length is 49 – 50 cm, then the brain weight will be 336 grams. At 1 month, the child’s height is 52 cm, brain weight is 360 grams. At 3 months, the child’s height is 56 cm, brain weight is 520 grams. At 6 months, with a height of 62 cm, GM weight is 670 g. At 9 months, with a height of 67 cm, GM weight is 760 g. At 1 year of age, the child’s height is 73 cm, brain weight is 960 g. At 1.5 years, with a height of 79 cm, the weight of the GM is 1045 g. At 2 years old, with a height of 85 cm, the weight of the GM is 1070 g. At 3 years old, the child’s height is 89 cm, and the brain weight is 1150 g. At 5 years old, height is 106 cm, weight is 1240 g. At 10 years old, height 132 cm, brain weight 1300 g. At 12 years old, height 145 cm, brain weight 1370 grams.
Physiology, brain function
Physiologically, all the work of the brain is built on the principles of hierarchy, integrity, systematicity and plasticity. These are the principles of functioning that carry out all conditioned and unconditioned reflexes. They contribute to the flow of conscious mental activity of a person. The principle of hierarchy is that phylogenetically younger parts of the brain carry out higher-order control, complementing but not replacing the function of phylogenetically more ancient parts. As a result of this, the body’s capabilities in more subtle differentiation of each stimulus by each analyzer are expanded, and a more adequate perception of the overall picture of the world is achieved based on the correlation of the results of the activities of many analyzers.
The highest form of expression of the hierarchical principle is the process of corticalization of functions. The principle of hierarchy is combined with the principles of integrity and systematicity, which consist in the fact that the brain functions as a single whole with the entire nervous system, while receiving afferent impulses, carries out its analysis and synthesis, forms a flow of efferent impulses that determine the adequate activity of all peripheral organs . As a result, a stable system is formed that provides continuous information communication: center - periphery - environment - periphery - center. Plasticity refers to the functional variability of nerve centers, which is clearly manifested in the process of compensation for impaired brain functions.
Irradiation of excitation plays an important role in the normal functioning of the brain. The feedback mechanism consists of closing the input and output of the same element or system. The dominant mechanism regulates the relationships between nerve centers.
Brain topography
Each part of the brain has its own functions. For example, information obtained through vision
is analyzed in the occipital region of the brain.
And the movement
is controlled by a fairly narrow strip of nervous tissue that stretches from the top of the head to the ear, like the earpiece of headphones.
Brain training
Is your memory failing? It’s not surprising, because she suffers without load in the same way as her muscles. Memory development exercises will help you - you can start doing them at any age.
At the same time, vision, hearing, movement, and all tactile sensations are controlled in a mirror way.
So, if a person has a stroke in the left hemisphere, the motor functions of the right side of the body are impaired. Next to the motor area is the area where tactile sensations
.
Therefore, often when the brain is damaged, a person simultaneously loses both the ability to move and the ability to feel. The perception of auditory information
occurs in the temporal region of the brain.
In right-handed people, the left temporal lobe is responsible for understanding words and expressing one's own thoughts. Right temporal lobe – helps to hear music and identify various noises. The area of the brain where the visual and auditory areas meet is responsible for the function of reading
- converting visual images into sounds.
Diseases, disorders, brain lesions
Diseases, disorders, and brain lesions are varied. In further articles, we will focus on pathologies such as brain tumor, brain cyst (including arachnoid, retrocerebellar, liquor), trauma, concussion or bruise of the brain, brain cancer, hydrocephalus (hydropsis), vascular atherosclerosis, aneurysm, encephalopathy, demyelination, ischemia, ischemic or hemorrhagic stroke, heart attack, atrophy, spasm or vasoconstriction, glioblastoma, meningioma, dysfunction, dystonia, diffuse changes, hypoxia (oxygen starvation), encephalitis, inflammation, vascular diseases, atrophic changes. The clinical picture of such diseases depends on the type of pathology.
Brain contusion (concussion) - symptoms and treatment
A patient with suspected traumatic brain injury should receive medical attention as soon as possible. Since it is impossible to reverse brain damage resulting from trauma, treatment measures should be aimed at stabilizing the patient's condition and preventing secondary damage.
Conservative treatment of brain contusions
In the setting of traumatic illness, decreased or increased intracranial pressure, decreased blood oxygen saturation, high temperature, and increased blood glucose levels can have a detrimental effect on the brain. In this regard, the main directions of therapy for people with severe bruises are identified [4]:
- breathing support (ventilators, oxygen mask);
- correction of blood circulation and infusion therapy (medication);
- treatment of intracranial hypertension;
- neuroprotection - protection of neurons from damage, carried out with medications.
Basic therapy. For victims with severe TBI, an open airway is created by removing saliva, blood and vomit. Sedatives and muscle relaxants are used as needed (designed to relax muscles, block nerve impulses and reduce pain.). Correction of elevated body temperature is necessary (using antipyretic drugs and/or physical conditioning methods) [4].
The development of convulsive syndrome in persons with a brain contusion is considered dangerous and requires immediate response. Seizures are always accompanied by rapid intracranial hypertension, an increase in the volume of intracranial hematomas, increased oxygen consumption in the brain, its blood supply and increased cerebral edema [13]. Prophylactic use of anticonvulsants (according to multicenter studies) in people with TBI reduces the likelihood of seizures in the acute period, but does not reduce the risk of their occurrence in the long-term period.
All persons with a cerebral contusion require prevention of thromboembolic complications (deep vein rhombosis of the lower extremities and pulmonary embolism), which involves the use of compression stockings, increased physical activity and anticoagulant therapy whenever possible. Mortality in thrombosis of the veins of the lower extremities reaches 9-50% [7].
It is also necessary to control blood glucose levels and prevent complications from the gastrointestinal tract (stress ulcers, gastrointestinal bleeding). The main reason for the development of stress ulcers is the release of catecholamine hormones during injury, which are produced in response to stress, insufficient blood supply to the upper gastrointestinal tract and disruption of its self-regulation.
Respiratory support. Indications for respiratory support [3][10]:
- depression of the level of wakefulness to stupor or coma;
- lack of own breathing;
- acutely developed breathing rhythm disturbances, pathological type of breathing (Cheyne-Stokes, Kussmaul);
- tachypnea (rapid shallow breathing) more than 30 respiratory movements per minute;
- clinical signs of hypoxemia (lack of oxygen in the blood) and/or hypercapnia (excess carbon dioxide): partial pressure of oxygen in arterial blood (PaO2) less than 60 mm Hg. Art.; hemoglobin saturation with arterial blood oxygen (SaO2) is less than 90%; partial pressure of carbon dioxide in arterial blood (PaCO2) more than 55 mm Hg. Art.;
- status epilepticus (epileptic seizures do not stop for more than 30 minutes);
- maxillofacial trauma combined with trauma to the facial skeleton, cranio-orbital region (near the orbit and adjacent areas) and/or chest.
The main task of respiratory support is to maintain normal carbon dioxide tension (PaCO2 - 30-35 mm Hg) and the necessary oxygenation of blood in the arterial bed (PaO2 more than 100 mm Hg) [6][7].
If the duration of mechanical ventilation is more than 48 hours after the start of breathing support, a tracheostomy should be performed (an operation to create an external opening in the wall of the trachea to establish breathing). When a brain contusion is combined with trauma to the facial skeleton and chest, it is preferable to perform a tracheostomy immediately upon admission of the victim to the hospital [10].
Correction of blood circulation and infusion therapy. More than half of patients with a decrease in wakefulness to stupor and coma are in a state of dehydration upon admission to the hospital. Causes include bleeding, insufficient fluid intake, overheating, vomiting and/or diabetes insipidus. Performing adequate infusion therapy (intravenous administration of medicinal solutions and drugs using a dropper) makes it possible to achieve a normal total blood volume, normalize cardiac output and the delivery of blood and oxygen to the brain.
The injured brain is extremely sensitive to low blood pressure (below 90 mm Hg), which a healthy brain tolerates normally. Therefore, the management of patients with severe TBI involves maintaining blood pressure (BP should be at least 90 mm Hg), which is necessary for adequate brain perfusion (providing it with oxygen and glucose) in conditions of edema [4][5][6] [7][9]. However, aggressive attempts to maintain blood pressure using vasopressors (vasoconstrictors) should be avoided due to the risk of respiratory distress syndrome (pulmonary edema with difficulty breathing) and cerebral edema [4][7].
Treatment of intracranial hypertension. To select adequate treatment tactics, it is necessary to distinguish between intracranial and extracranial causes of high ICP. The former include intracranial hematomas, bruises, edema and/or cerebral ischemia, epileptic seizures, and meningitis. The second is a lack of oxygen supply, inadequate sedation or ventilation, impaired venous outflow from the cranial cavity, increased intrathoracic and intra-abdominal pressure [1][3]. All these reasons can accompany brain contusion.
Sedation and analgesia are first-line interventions for the treatment of intracranial hypertension [4][7]. The head of the bed must be raised by 30-40° to improve venous outflow from the cranial cavity. To treat increased intracranial pressure and protect the brain from secondary damage, craniocerebral hypothermia (lowering brain temperature) is used. It is sufficient to carry out moderate hypothermia (T = 30-31 °C) [1][4]. The use of hyperbaric oxygenation (saturation of the patient with oxygen under high pressure) is pathogenetically justified in persons with brain contusion, since this method increases the oxygen tension in arterial blood and improves oxygen saturation of the brain.
To reduce intra-abdominal pressure, drugs are used that improve intestinal motility and normalize the function of the gastrointestinal tract [4][6]. If intracranial hypertension is not responsive to drug therapy, decompressive craniotomy is indicated.
Neuroprotection. Currently, the use of neuroprotective drugs is a promising direction in the treatment of brain contusions [9]. Based on their mechanism of action, neuroprotectors are divided into several types:
- Calcium channel blockers (Nimodipine, Breinal, Dilceren, Nimopin, Nimotop). They reduce the entry of calcium ions into the cell, reduce the level of damage and death of nerve cells under the influence of neurotransmitters and prevent apoptosis (programmed cell death).
- Antioxidants and antihypoxants (Actovegin, polyethylene glycol superoxide dismutase, Solcoseryl, Neurox, Mexidol, Armadin, Cytoflavin, Neurocard, Astrox, Meksifin, tocopherol, Methostabil, ascorbic acid, Ascovit, Nootropil, Piracetam, Noocetam, Melatonin, Cavinton, Vinpocetine, Cohen winter Q10). These drugs are nitrogen synthase antagonists, they prevent the formation of free radicals, restore the activity of antioxidant enzymes, accelerate glycolysis (the process of glucose oxidation), increase resistance to hypoxia and improve cerebral blood flow.
- NMDA receptor antagonists (Memantine, Memantal, Memorel, Noodzheron, Akatinol, Memikar, Mirvedol, Memaneurin). Reduce the damaging effects of glutamate.
- Blockers of the inflammatory and immune response (Cycloferon, COX-2 inhibitors, CD11 and CD18 antibodies). Reduce the severity of the inflammatory reaction.
- Stabilizers of cell membranes: intermediate products of phosphatidylcholine synthesis (Recognan, citicoline, Ceraxon, Proneuro, Quinelle, Neuropol, Neurocholin, Noocil, Ceresil Canon), magnesium and potassium preparations (magnesium sulfate, Aspangin, Pamaton, Asparkam, Panaspar, Panangin).
- Drugs that improve synaptic transmission (precursors for acetylcholine synthesis - Cereton, Cerepro, Gleatser, Holitylin, Delecit, Gliatilin).
- Apoptosis blockers (caspase-3 inhibitors, calpain inhibitors).
- Drugs with a neuron-specific neurotrophic effect (Cortexin, Cerebrolysate, Cerebrolysin).
- Immunosuppressants (cyclosporine A). Suppress the immune response.
Nutrition for severe brain contusion . With serious damage, patients, as a rule, cannot eat on their own, so early nutritional support (i.e., the introduction of nutrients into the body) is necessary. Such support should match the patient's protein and energy needs. Basic energy metabolism in patients with severe brain contusion corresponds to 20-25 kcal/kg per day [4][6].
Surgical treatment of brain contusions
Some patients with severe traumatic brain injury are transported to the operating room after a head CT scan. The purpose of surgery for severe brain contusion is to remove massive intracranial hematomas or correct elevated ICP.
Not all patients with TBI require emergency intervention. Since the size of a brain contusion and the volume of an intracranial hematoma may increase during the first hours/days after injury, dynamic monitoring is recommended. Treatment of such patients is carried out in an intensive care unit. If neurological disorders increase or intracranial pressure increases (if an ICP monitoring sensor was installed), a control CT scan is performed. If a significant increase in the volume of the hematoma or displacement of the brain is diagnosed, the safest option will be surgical intervention to prevent brain death.
Before surgery, the hair over the affected area of the brain is shaved. After cutting the scalp and removing the skin flap, the bone is cut out. The bone is removed and the underlying dura mater is opened with the utmost care. The doctor removes the hematoma or brain contusion. In the presence of severe cerebral edema, plastic surgery of the dura mater is performed using a patch from one’s own tissue or artificial replacement material. This is necessary to prevent further displacement of the brain. In such cases, the bone is not put back in its original place.
Before “closing” the wound, it is possible to install an ICP sensor if it has not been installed previously. Upon completion of the operation, the patient is transferred to the intensive care unit for intensive treatment measures aimed at combating cerebral edema and preventing infectious and thromboembolic complications.
Decompressive craniotomy is the most aggressive treatment for intracranial hypertension [3][9]. It is used when conservative therapy is ineffective. The main goal of decompressive trephination is to increase intracranial volume. As a result, the pressure in the cranial cavity is reduced and the blood supply to the brain is normalized.
Decompressive trepanation includes infratemporal and bifrontal decompression, temporal lobectomy and hemicraniectomy. They are carried out in cases of pronounced displacement of brain structures and persistent intracranial hypertension in patients with clinical and CT signs of brain compression.
Possible postoperative complications. In the long-term postoperative period of TBI, epilepsy is registered in 13% of patients, and post-traumatic hydrocephalus in 11% [3]. Post-traumatic epilepsy occurs due to the formation of a pathological focus in the brain. Post-traumatic hydrocephalus is caused by impaired circulation (formation of adhesions) and absorption of cerebrospinal fluid.
Brain treatment in Saratov, Russia
Sarklinik provides treatment for a number of diseases, diseases of the central and peripheral nervous system in Saratov, in Russia for children, adolescents, adults, boys, girls, guys, girls, men, women, brain treatment in Saratov . Hardware and non-hardware treatment methods make it possible to restore the functioning of the human nervous system.
Sign up for a consultation. There are contraindications. Specialist consultation is required.
Text: ® SARCLINIC | Sarclinic.com \ Sarlcinic.ru Photo: © pixologic / Photobank Photogenica / photogenica.ru The people depicted in the photo are models, do not suffer from the diseases described and/or all coincidences are excluded.
Related posts:
Accentuation of character in adolescents, types, test, methodology, correction in Saratov
Dysmorphophobia, treatment in Saratov, how to treat dysmorphophobia
Urination, urination mechanism, why does it happen, does urinary incontinence happen?
Millard–Gubler syndrome (A. Millard, AM Gubler) alternating pontine
Benedict's syndrome M Benedict, alternating peduncular syndrome