The foot is a section of the lower limb that consists of several bones, ligaments and muscles. The main sections are the metatarsus, the fingers themselves, and the tarsus. The ligamentous apparatus is represented by the ankle, talus and other joints. Also an integral element are the muscles and fascia of the foot, which provide all kinds of movements with the toes.
Bones of the foot: tarsus
The tarsus is one of the integral elements of the foot. It consists of 2 sections - posterior and anterior. The posterior one is represented by the calcaneus, as well as the talus. The anterior one consists of 3 wedge-shaped bones. It also includes the cuboid and scaphoid bones.
If we consider the anatomy of the posterior region, it is necessary to mention bones such as the calcaneus and talus. The constituent elements of the latter are the body and the head, and between these sections there is a neck (narrow part). On top there is an articular surface, which serves as an articulation with the adjacent part of the limb - the lower leg.
The shape of the calcaneus is elongated, and it is laterally flattened. This is the largest bone of the foot. It consists of a body and a tubercle that can be easily felt by hand. There is a protrusion on the inside that serves as a support for the adjacent talus.
In the anterior section there are sphenoid bones connected to each other. There is also a cuboid and a navicular. The latter is located near the inner edge. From the inside, its surface is lumpy, which, when palpated, allows one to determine the height of the arch of the foot. It has several articular surfaces, with the help of which it articulates with neighboring bones.
The cuboid bone runs along the outer edge and connects to the sphenoid bone. It also comes into direct contact with bones such as the scaphoid and calcaneus, as well as the metatarsal region. There are also 3 wedge-shaped bones - lateral (back), medial and intermediate.
Functional structure of the foot
The foot, as a structure, has a rather complex arched shape, reminiscent of a spiral or propeller blade. The foot has an arched structure. It is customary to distinguish between two longitudinal arches and one transverse arch.
Longitudinal bone arches: internal (spring) is formed by the calcaneus, talus, navicular, three wedge-shaped, 1,2,3 metatarsal bones, is an arch that runs through the entire foot, starts from the calcaneal tubercle and ends at the fulcrum of the head of the 1st metatarsal bone;
the outer (cargo) is formed by the calcaneus, cuboid, 4th and 5th metatarsal bones, and also has the shape of an arc that runs through the entire foot, starting from the heel tubercle and ending at the fulcrum of the head of the 5th metatarsal bone.
The vast majority of doctors do not doubt the existence of the transverse fornix, but there are two opinions regarding its localization. First: the transverse bony arch is an arch formed by all the heads of the metatarsal bones. It is located in a plane perpendicular to the arcs of the longitudinal arches. Second: the transverse arch is most clearly expressed in the area of the sphenoid, cuboid and bases of the metatarsal bones.
It is possible to consider the arches of the foot as independent elements only conditionally, since in reality they are in constant interaction and function as a single organ. In maintaining the arched shape of the foot, the leading role belongs to the ligaments, plantar aponeurosis and tendons of the muscles that pass from the lower leg to the foot, and the actual muscles of the dorsal and plantar surfaces of the foot.
The foot is supported at three points: the area of the heel tubercle, the heads of the 1st and 5th metatarsal bones. The pressure between the front and rear support points is normally distributed as 1:4.
Between the bony skeleton of the foot and the supporting surface there are soft tissue structures (muscles, ligaments, subcutaneous tissue, the layer of skin itself), which form the relief of the plantar surface of the foot; numerous vessels and nerves of the foot pass through here. The skin of the plantar area in places of contact with the support has a cellular structure. Fibrous cords are located perpendicularly in it, between which there are areas of adipose tissue, which are good shock absorbers. In the area of support points (heel, area of metatarsophalangeal joints) the skin is denser and resistant to compression.
Anatomy of the foot: metatarsus
The next section of the foot is the metatarsus. Its shape is tubular. The bone is represented by the base, as well as the head and body. The latter is shaped like a conventional prism with 3 faces. On top of the bases of the metatarsus there are articular surfaces that connect to the adjacent section - the tarsus.
They also connect to the articular surfaces of the phalanges of the fingers. All bones of the metatarsus can be easily felt with the fingers, since the layer of soft tissue is small. Moreover, its component parts are located in different planes. The arch they form runs transversely.
Own muscles and tendons of the foot
Flexor digitorum brevis (FDB)
The muscle starts from the internal (medial) process of the calcaneus and the central part of the plantar fascia. It is attached to all 4 small toes. At the level of the PFJ, each muscle tendon is divided into 2 bundles, each of which goes around the tendon of the long flexor of the finger and is attached to the middle phalanges of 2-5 fingers.
The muscle performs flexion (plantar flexion) of the middle phalanges of the fingers in the PIPJ. As the muscle continues to contract, the proximal phalanges flex at the MCP joint.
Vermiform muscles
These are 4 small muscles starting from the 4 flexor tendons on the foot. The tendon of each lumbrical muscle is attached to the tendon extension of the long extensor muscles on the dorsum of the proximal phalanges of the fingers. Contraction of the lumbrical muscles leads to extension of the fingers in the PIPJ and DIPJ. Because the tendons are located below the point of rotation of the MCP joint, they also perform flexion at these joints.
Ligamentous apparatus
This apparatus is represented by a number of joints - ankle, talus, interphalangeal and others:
- The ankle includes the talus and tibia bones. It has the shape of a block. Provides flexion and extension of the foot, and in a fairly flexible form up to a right angle (90 degrees). The ankle is securely strengthened by ligaments that are located on both sides - above and below. Also on the inner surface there is a deltoid ligament, which has the shape of a conventional triangle. On the outer surface there are other ligaments that run towards the heel and talus bones.
- The subtalar provides articulation between the calcaneus and the talus and can be found in the posterior region. It has the shape of a conventional cylinder, partly reminiscent of a spiral. There is a thin capsule around the joint - it contains small ligaments.
- The talocaleonavicular is located between the calcaneus and talus bones. This joint is shaped like a ball. Moreover, it moves simultaneously with the subtalar joint, since together with it it forms a functional joint. Both joints are strengthened with the help of an interosseous ligament (the so-called syndesmosis).
- Tarsometatarsal - several small joints that are located between the bones of the main sections (tarsus and metatarsus). Basically they have a flat shape, mobility is functionally limited.
- Metatarsophalangeal joints are spherical joints with relatively low mobility. They consist of the heads of the metatarsals and provide flexion and extension of all toes.
- Interphalangeal - small joints between individual phalanges. Provides full finger mobility.
Muscles and tendons of the leg
Calf muscle
This powerful calf muscle consists of two heads, medial and lateral, which originate on the posterior surface of the distal end of the thigh and are attached by the Achilles tendon to the calcaneus.
The gastrocnemius muscle is involved in running, jumping, and all types of activities that involve high-intensity stress on the lower extremities.
Together with the soleus muscle, it forms the calf muscle, called the triceps surae muscle. The function of the gastrocnemius muscle is to flex the foot and ankle downward (plantar flexion).
Forceful dorsiflexion of the foot can cause damage to this muscle.
Soleus muscle
This muscle starts from the tibia below the level of the knee joint and is located under the gastrocnemius muscle. Distally, its tendon unites with the gastrocnemius tendon to form the Achilles tendon. Like the gastrocnemius muscle, the main function of this muscle is plantar flexion of the foot.
The calf muscle is involved in walking, dancing, and maintaining an upright body position when we stand. Also, one of its important functions is to ensure blood flow through the veins from the lower limb to the heart.
Plantaris muscle
It is a small muscle that originates along the lateral head of the gastrocnemius muscle. The tendon of this muscle is the longest tendon in the human body. It is a weak but still plantar flexor of the foot. Damage to this muscle can occur when playing sports.
Achilles tendon
The Achilles tendon is formed at the mid-calf level by the gastrocnemius and soleus muscles and is attached to the heel bone. This is the most powerful and durable tendon in the human body.
It is subjected to the most significant loads compared to all other tendons. When running and jumping, the tendon is subjected to loads that are 8 times greater than body weight, and when walking - 4 times.
Through the Achilles tendon, the gastrocnemius and soleus muscles perform plantar flexion of the foot and ankle joint.
The tendon consists of three parts:
- Musculotendinous part (proximal part of the tendon, at the level of which muscle fibers turn into tendon fibers)
- Non-insertional part (body) of the Achilles tendon
- Insertion part of the Achilles tendon
The blood supply to the Achilles tendon is quite poor compared to other anatomical structures. The tendon in its upper section receives blood supply from the muscles that form the tendon, and below - from the heel bone to which it is attached. The middle part of the tendon is supplied with blood by the branches of the peroneal artery and this blood supply is the poorest, so it is not surprising that this part of the tendon is most susceptible to damage. The Achilles tendon is surrounded by a soft tissue sheath called the paratenon. The middle part of the tendon receives its blood supply precisely through this sheath. The paratenon allows the Achilles tendon to glide relative to surrounding tissues for up to 1.5 cm.
Anterior to the Achilles tendon is the Kager fat pad, which performs an important function of protecting the Achilles tendon.
MR anatomy of the Achilles tendon
- Musculotendinous part
- Kager fat body
- Non-insertional part of the Achilles tendon
- Insertion part of the Achilles tendon
Let's evaluate flat feet
The main causes of corns are foot deformation, prolonged wearing of narrow, incorrectly sized shoes, and high-heeled shoes. If there is no foot deformation or internal health problems, then you need to change your shoes to comfortable ones, and the corns will go away. If there is a foot deformity, then only individual insoles can help, which will compensate for the existing pathology.
You can remove corns in various ways, but if the cause of their appearance is not eliminated, they will form again. When making individual insoles, in about 30% of cases it is possible to completely get rid of corns. Standard ready-made insoles do not help. Therefore, I recommend that you contact a podiatrist (foot specialist) and figure out the reasons.
Neuropathy
Neuropathy - damage to sensory nerves occurs in 70% of patients with diabetes. Nerves in the legs are particularly susceptible to damage because poor diet and high sugar levels destroy the myelin sheath. In the neuropathic form, where a diabetic patient loses sensation in the legs, any microtrauma may go unnoticed until serious ulcers develop.
Signs of foot neuropathy:
- Numbness of the skin
- Tingling
- Pain or burning of the skin of the legs (some forms of neuropathy may cause pain)
Blood vessels
The foot is supplied by 2 main arteries: the posterior tibial artery and the dorsal pedis artery. They divide into smaller arteries and saturate the tissues of the foot with oxygen. Veins carry blood back to the heart. they are connected to the arteries by small capillaries. The veins are divided into superficial and deep. The longest vein in the body originates from the big toe and is called the great saphenous vein of the leg.
Due to the fact that the blood vessels of the foot are the most distant, it is in them that circulatory disorders most often occur. This can lead to arteriosclerosis, atherosclerosis, varicose veins, leg swelling, etc.
Egyptian foot - artificial toes
The Egyptian foot looks neat: the toes decrease evenly. If you draw an imaginary line from the tip of your first finger to your little finger, you will get a straight line at an angle of 45 degrees.
Artificial fingers were found on one of the ancient Egyptian mummies. Researchers from the University of Manchester have found two prosthetics, one made of papier-mâché and the other made of wood and leather.
Scientists decided to conduct an experiment and made their own version of prosthetic fingers. The results showed that they could help people who had lost their thumb to walk in sandals typical of ancient Egyptian times.
It has long been thought that people with Egyptian foot have a higher risk of ingrown toenails than others. The Japanese Nippon Medical School conducted a comparative study of Egyptian, Greek and Celtic feet and found that people with Egyptian toes, on the other hand, had less of this problem.
In Japan, 70–80% of the population has Egyptian foot type, so shoes there are made taking this feature into account. Some shoe manufacturers sometimes draw customers' attention to the fact that their products are designed for Egyptian feet.
Celtic foot - a mixture of cultures
The Celts are associated with Western Europe, especially Britain, but their exact origins are uncertain. The shape of their feet and toes also suggests a mixture of different cultures.
The Celtic foot shape is a combination of Germanic and Greek toe shapes. In this type, the second finger is longer than the others, and the first and third are almost the same length. Genetic research has shed light on the reasons for this combination.
The results showed that regions of the UK, such as Cornwall, Scotland, Wales and Northern Ireland, where Celtic ancestry predominates, are genetically distinct from each other. This means that there is no single Celtic genetic group as such.
Genetics of origin. Haplogroups
The Romans left their footprints throughout Europe and North Africa during their conquests. They invented the “foot,” a measure of length that is still used in Great Britain today.
A study of DNA samples from more than 6 thousand Europeans confirms this theory. According to the results, European populations migrated to the territory of the modern United Kingdom over the past 10 thousand years.
The shape of the Celtic foot may be the result of a mixture of several peoples.
Features of a child's foot
In children under 3 years of age, the subcutaneous fat layer is significantly developed; it fills the entire niche of the internal longitudinal arch, performing an arch-forming role and the role of a shock absorber.
The ligaments of a child’s foot contain few elastic fibers and a lot of ground substance. The main role in the passive fixation of the arches belongs to the plantar aponeurosis.
Children have wider joint spaces than adults. This makes the joints mobile and reduces the role of the articular surfaces as a passive stabilizer of the arches. Up to 6 years of age, X-rays do not show lines of force in the bones of the foot, which indicates their functional failure and vulnerability. The tarsal bones are not differentiated until the age of 6 years.
Only a doctor can assess the true condition of a child’s feet based on clinical examination data, measurements of foot parameters, and plantography.
It should be noted that in children under 3 years of age, upon examination, this fat pad gives false impressions of a decrease in the size of the soft arch and flattening of the internal longitudinal arch.
Horseshoes on the heels
The formation of horseshoes around the heels is often called a sign of joint problems. Corns in the form of horseshoes are formed in cases where the load falls on the marginal parts of the heel, as a rule, associated with deformation of the knee and hip joints, problems in the lumbar spine. Often these deformations are associated with autoimmune processes occurring in the body.
The heels are smooth. How to help “your two” Read more
Diagram of the main reflex zones of the feet
| LEFT FOOT 1. Head, brain (right side) 2. Frontal sinuses (right side) 3. Cerebellum, brain stem 4. Pituitary gland 5. Trigeminal nerve, right temple 6. Nose 7. Occiput 8. Right eye 9. Right ear 10. Left shoulder 11. Trapezius muscle on the left 12. Thyroid gland 13. Parathyroid glands 14. Lungs and bronchi on the left 15. Stomach 16. Duodenum 17. Pancreas 20. Solar plexus 21. Adrenal gland on the left 22. Kidney on the left 23. Urinary tract left 24. Bladder 25. Small intestine 29. Transverse colon 30. Descending part of the colon 31. Rectum 32. Anus 33. Heart 34. Spleen 35. Left knee joint 36. Left gonads 38. Left hip joint 57 Nervous system 60. Left lower leg 61. Throat | RIGHT FOOT 1. Head, brain (left side) 2. Frontal sinuses (left side) 3. Cerebellum, brain stem 4. Pituitary gland 5. Trigeminal nerve, left temple 6. Nose 7. Occiput 8. Left eye 9. Left ear 10. Right shoulder 11. Trapezius muscle on the right 12. Thyroid gland 13. Parathyroid glands 14. Lungs and bronchi on the right 15. Stomach 16. Duodenum 17. Pancreas 18. Liver 19. Gallbladder 20. Solar plexus 21. Adrenal gland on the right 22 Right kidney 23. Right urinary tract 24. Bladder 25. Small intestine 26. Appendix 27. Ileum 28. Ascending colon 29. Transverse colon 35. Right knee joint 36. Right gonads 38. Right hip joint 57. Nervous system 60. Right lower leg 61. Throat |
What types of feet are there?
According to the theory, there are five main types, which differ in the length of the fingers and the line they form.
| Foot type | Description |
| Greek | The second finger protrudes forward relative to all the others, including the thumb. |
| Roman | The first three fingers are the same length, while the two are usually shorter. |
| Celtic | The thumb is short, the second is longer than the others, the others decrease in size towards the little finger. |
| German | Large thumb and the rest are the same size. |
| Egyptian | The fingers decrease evenly (as a ladder) from the thumb to the little finger. |
It is assumed that people with Greek feet had Greek ancestors, those with Egyptian feet had Egyptian ancestors, and so on. The theory emerged in the 19th century, when the idea of belonging to "Germanic" or "Egyptian" populations, which were associated with ethnic homogeneity, became fashionable.
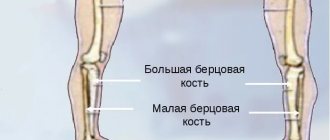
Structure and functions of the ankle joint
The foot is connected to the bones of the lower leg using a movable ankle joint. The bones of the lower leg (tibia - on the inside - and fibula - on the outside), thanks to the protruding ankles, form a kind of fork that covers the block of the talus bone. Movements in the ankle joint occur around the transverse axis: flexion, when the toe of the foot moves down, and extension, when the toe moves up and approaches the lower leg. These movements are sometimes called plantarflexion and dorsiflexion.
The ligaments that strengthen the ankle joint are located on the sides of the joint. Their fibers fan out from the ankles to the navicular, talus and calcaneus bones. Sprains in the joint are common. This happens when plantar flexion occurs simultaneously with the lowering of the outer edge of the foot. In this case, the narrower rear part of the talus block appears in the fork between the ankles, which is weakly wedged and leads to lateral movement - the leg is tucked in. The lateral collateral ligament may be sprained, and sometimes even part of the ankle may be torn off where the ligament attaches to it.
Complications
The extreme and most dangerous stage of DFS is the development of gangrene of the foot. Diabetic foot is the leading cause of non-traumatic amputation in peacetime. Every year in Russia 70,000 amputations are performed for diabetic gangrene.
Diabetic gangrene often occurs with an associated anaerobic infection. With this outcome, the damaged tissues die, and the blood and healthy tissues become infected. The disease develops very quickly, often leading to death.
Trophic ulcers are another complication, most often found on the sole or big toe. They can also form on the sides of the foot from poorly fitting shoes. If left untreated, they can lead to serious infections. The classification of complications of diabetes includes trophic changes in the skin of the foot.