Every year there is an increasing increase in oncological pathology. Lung cancer occupies the first place in the structure of oncological diseases. This is due to both environmental pollution and smoking, alcoholism, genetic predisposition and other factors. The statistics of deaths from lung cancer are also frightening. Everything is connected with the fact that a person does not notice symptoms at all for a long time, and even when he notices them, he easily finds a simpler explanation for them. This is followed by a period of symptomatic treatment, and only when things get really bad do patients seek help. Unfortunately, more than half of patients already have numerous metastases when a pronounced clinical picture appears.
Depending on the location, central and peripheral lung cancer are divided, and if the entire lung is involved in the process, it is called massive. Central lung cancer is localized in large bronchi, and peripheral lung cancer is located in bronchi with a smaller diameter down to the alveoli. But scientists argue that the differences are not only in localization, but also in structure, origin, pathogenesis, clinic, etc. For example, it is believed that smoking and prolonged inhalation of polluted air are the etiological factors for central, and for peripheral lung cancer, lymphogenous and hematogenous are characteristic ingress of carcinogens.
How long you live with peripheral lung cancer depends on many factors, including treatment. The prognosis for peripheral cancer is significantly more favorable with timely diagnosis and effective specific therapy.
About seventy percent of cases of peripheral cancer of the right lung are localized in the upper lobes, about twenty in the lower lobes, and less than ten in the middle lobes. Histologically, peripheral cancer is most often represented by either adenocarcinoma or squamous cell carcinoma.
It is the peripheral form of cancer that is practically asymptomatic. Diagnosis at an early stage is often associated with preventive medical examinations.
The Yusupov Hospital is equipped with all the modern equipment necessary to diagnose lung cancer. Comfortable rooms, polite staff, highly qualified doctors - these are all the keys to successful treatment.
Forms of the disease in question
Tumor processes in the lungs are diverse. Peripheral lung cancer has several types. The cortico-pleural appearance is an oval-shaped formation that grows in more than one node. This neoplasm grows directly into the chest, after which it is located in the so-called subpleural space. The resulting pathology belongs to the squamous cell type of cancer. The structure of the tumor is homogeneous; it has a lumpy inner surface and poorly distinguishable contours. The tumor can grow both into adjacent ribs and into the bodies of adjacent thoracic vertebrae.
The so-called cavitary form of peripheral lung cancer is characterized by the absence of symptoms. It is detected at later stages, when pathological processes have become irreversible. Cavity formations are formed inside the pulmonary sections, having the shape of a ball, a lumpy outer surface and poorly distinguishable contours. The growth of the tumor leads to the proliferation of formations with parallel thickening of their walls.
Chemotherapy
Planning the course of treatment for non-small cell lung cancer includes the use of pharmacological agents. It is used for prevention purposes: adjuvant (auxiliary), postoperative chemotherapy for stages 2-3 of the disease and in the therapeutic course.
Depending on the histological type of tumor, stage of the disease and expected sensitivity to effects, various regimens for the use of chemotherapy have been developed.
Targeted therapy (eng. target - target, goal)
A separate type of pharmacological treatment, which consists in prescribing inhibitor drugs that act only on tumor cells in which various disorders have been identified, delaying or even blocking further growth.
- Tyrosine kinase inhibitors (gefitinib, erlotinib, afatinib) are used in the treatment of patients whose tumor tissue has mutations in the EGFR gene.
- If the EGFR mutation status is negative, use ALK inhibitors (crizotinib, alectinib).
There are targeted drugs, the prescription of which does not require the identification of any abnormalities in tumor cells. These include bevacizumab (VEGF inhibitor), nivolumab and pembrolizumab (anti-PDL1 antibodies).
Oncology of the upper lobe of the left lung
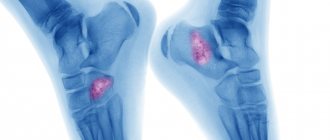
In people with this type of cancer, X-rays clearly show blurred contours, an irregular shape of the formation and its heterogeneous structure. The pulmonary roots are expanded due to the influence of the vascular trunks. In most cases, the lymph nodes remain the same size (in the case of lower lobe cancer, the situation is the opposite).
As for oncology of the upper lobe of the right lung, it is in many ways similar to the previous pathology, but it is diagnosed much more often. The formation of the nodular form occurs in the terminal bronchioles. The disease makes itself felt after the soft lung tissues germinate. X-ray examination allows us to examine a formation that has a nodular shape, clear contours and a bumpy surface. Sometimes the edge of the tumor contains a small depression. The presence of such a depression indicates that a large vessel has entered the node.
Reasons for appearance
Factors in the development of lung cancer can be grouped into three groups: genetic, exogenous (external) and endogenous (internal). Genetic causes include:
- The familial nature of the disease is three or more cases of lung cancer in close relatives.
- The patient has a history of another malignant tumor.
External factors that influence the development of this neoplasm:
- Smoking. It is addiction to this habit that is the main reason for the development of lung cancer. Moreover, not only active but also passive smoking can lead to the appearance of a tumor.
- Exposure to carcinogens: exhaust gases; some organic substances (for example, arsenic, cadmium); tars and cokes that appear in the air as a result of coal and oil processing.
- Occupational hazards: work in uranium mines; industrial processing of steel, wood, metal. Also, the risk of lung cancer is increased among those workers who come into contact with stone dust, asbestos, aluminum and nickel. The combination of these factors with smoking further increases the likelihood of developing the disease.
Endogenous factors for the development of central lung cancer include:
- Age over 50 years.
- Chronic inflammatory processes in the bronchi.
- Presence of endocrine diseases.
- Immunodeficiency conditions (HIV infection, therapy with cytostatic drugs).
Under the influence of unfavorable factors, precancerous changes are formed in the bronchi. They play an important role in the pathogenesis of this disease.
Tumor collapse and centralization syndrome
When the pathogenic formation reaches a large size, the pulmonary blood supply deteriorates, and this leads to tumor disintegration. The decay occurs gradually with the formation of cavities inside the tumor node. Due to the unevenness of the process, small tumor masses remain on the walls of the cavity. When small cavities merge into one, the stage of major decay begins. At the end, the phase of the so-called central decay begins. Thanks to the examination, it is possible to identify the presence of a cavity formation with thick walls; There is a horizontal liquid level inside it. The course of the described pathology is similar to the course of an abscess. A person’s temperature rises, the expectoration becomes purulent (sometimes there is blood in the secreted mucus).
Treatment
The main treatment for central lung cancer is surgical removal. Oncologists also use radiation treatment, chemotherapy and photodynamic therapy.
Surgical method
When excision of central cancer, a section of lung tissue in a volume of at least a fraction is removed with a minimum indentation of 2 cm from the border of the tumor towards healthy tissue. Regional lymph nodes are also removed.
Surgical options for this disease include:
- Lobectomy (removal of a lobe of the lung).
- Bilobectomy (excision of two lobes).
- Pneumonectomy (complete removal of the lung).
If the tumor spreads to neighboring organs, their resection may be performed. For example, if the cancer is located near the trachea, its partial removal is possible.
Other therapies
Radiation therapy can be used as a radical method or as part of palliative care for the patient. As an independent method of treatment, it is used for tumors of stages I-II in case of contraindications to surgical treatment.
The administration of chemotherapy drugs is considered as an auxiliary method for lung cancer. The best result is provided by a combination of radiotherapy and chemotherapy (when used sequentially or simultaneously).
Symptoms of the described deviation
In the early stages of peripheral lung cancer, a person may suffer from shortness of breath and chest pain. There is often expectoration of blood. The progression of the pathology leads to an increase in temperature and copious sputum production. After a certain time, secondary symptoms are added to the main symptoms, which appear after the pathogenic formation grows into adjacent tissues, as well as nearby organs.
Atelectasis - forms after the tumor grows inside the bronchus. This germination disrupts the pneumatization of lung tissue.
Syndrome of neurological abnormalities - progresses when metastases enter the brain. The syndrome is characterized by signs of paralysis of the phrenic and recurrent nerves.
Perifocal inflammation - forms in situations where a focus of pneumonia forms around a tumor node. Symptoms include hyperthermia, cough with sputum production.
Pleural effusion is a deviation that cannot be treated by pleural puncture. After a certain time after removal, the pathology develops again.
Pancoast syndrome - manifests itself in the form of atrophy of the muscles of the upper extremities; There is often pain in the shoulder girdle area. Progresses in the presence of apical oncology, affecting the nerves and vessels of the shoulder girdle.
The so-called mediastinal compression syndrome makes itself felt by difficulty swallowing and pain in the chest area.
Life forecast
The prognosis of lung cancer in NSCLC includes symptoms, tumor size (> 3 cm), non-squamous histology, extent of spread (stage), lymph node metastasis and vascular invasion. Inoperability of the disease, severe symptoms and weight loss of more than 10% give lower results. Prognostic factors for small cell lung cancer include condition status, sex, stage of disease, and involvement of the central nervous system or liver at the time of diagnosis.
For non-small cell lung cancer, the prognosis for life with complete surgical resection of stage IA (early stage of the disease) is 70% five-year survival.
Differential diagnosis
In accurately identifying the pathology in question, bronchographic as well as radiation examination is of enormous importance. Thanks to such procedures, it is possible not only to diagnose the presence of cancer, but also to determine its form. If a person suffers from central cancer, x-rays will show insufficient ventilation of the lungs, atelectasis of lung tissue, narrowing of the central bronchi, and abnormal sizes of mediastinal lymph nodes. The tumor will have poorly distinguishable contours, as well as a heterogeneous structure. An x-ray will be able to show decay cavities with poorly visible contours; in addition, it will allow you to examine the node against the background of lung tissue. Bronchographic examination will provide consideration of multiple bronchial amputations; in addition, it will show narrowing of the small bronchi.
Features of the diagnosis of malignant tumors localized in large bronchi
If, based on the clinical picture and x-ray, the doctor suspects exophytic cancer, the patient most often undergoes bronchoscopy while simultaneously performing a biopsy. To do this, a special optical device with a device that allows you to take a small piece of tissue for analysis under a microscope is inserted into the respiratory tract. With a wet cough, examination of sputum for the presence of malignant cells is also indicated.
Endophytic neoplasms in the early stages are difficult and sometimes impossible to see using a bronchoscope. In this case, a preliminary diagnosis is made using x-rays and CT scans. Material for microscopic examination in such patients is obtained using a puncture biopsy under CT or X-ray control or through a low-traumatic diagnostic procedure - mediastinoscopy.
If it is necessary to clarify the diagnosis, other types of scanning may be prescribed: PET/CT, MRI.
A large exophytic tumor is clearly visible on CT
Determining the levels of tumor markers, as well as regular monitoring of these indicators, allows the doctor to optimize and adjust the treatment regimen.
Surgery
• removal of the pulmonary lobe (the most common procedure);
• tumor removal - this type of operation is usually performed on elderly people or patients with concomitant disease that prohibits extensive abdominal surgery (due to danger to life);
• complete removal of the lung - such an intervention is carried out in the 2nd and 3rd stages of cancer development;
• combined surgery – involves removal of the tumor, as well as affected neighboring organs and tissues.
Radiation therapy for lung cancer
Today, such modern methods of radiotherapy as IMRT (radiation therapy with the possibility of changing the radiation dose), 3D conformal radiation therapy (three-dimensional computer planning of selective irradiation) and stereotactic (precisely focused) radiation therapy are being actively implemented. In addition to oncologists, medical physicists, radiologists, dosimetrist physicists and other specialists participate in these manipulations.
Method shown:
- patients with a resectable lung tumor for whom surgical treatment cannot be performed due to contraindications from the cardiovascular system or for other reasons;
- as an alternative to surgery;
- to reduce the risk of relapse in case of damage to the mediastinal lymph nodes, a positive resection margin according to histological examination.