Aspirin (acetylsalicylic acid) is one of the most popular antipyretic drugs in the treatment of influenza. But this drug can lead to tragedy if it is prescribed for the flu in children. It's all about the so-called Reye's syndrome.
This rare but very serious and potentially fatal disease occurs in children 2–14 years of age who are given aspirin. Reye's syndrome can also occur with chickenpox, measles and some other viral infections. It usually occurs when the child is already recovering. Suddenly vomiting begins, then confusion occurs, the condition quickly worsens, a coma develops... The mortality rate with this disease is colossal. If active treatment was started in the early stages - up to 20%, if in the later stages - 80%.
Pathologist's disease
This disease was first described in detail in 1963 by Australian pathologist Douglas Rey . In the famous medical journal The Lancet, he and his colleagues described 21 cases of an unknown childhood disease in which children develop encephalopathy (brain damage) and steatosis (fatty liver). Less common was excess fat accumulation in the kidneys and other internal organs. 17 of these children died. The article did not mention any connection between the disease and aspirin, influenza, or any other viral infection.
Article on the topic
Snot again!
What to do to prevent a child from getting sick in the garden The following year, the American Johnson Johnson published a description of an outbreak of influenza, and among the sick, 16 children were described with the same symptoms as in D. Ray’s article.
After this, the new disease was often even called Ray-Johnson syndrome. And the role of aspirin was discovered only 15 years later - in 1979 in the USA. In 1980, the Center for Disease Control (an American organization similar to our sanitary and epidemiological service) notified doctors and parents about the connection of this disease with the use of aspirin in children with influenza and other viral infections. But an official warning in the instructions for drugs containing aspirin appeared only in 1986. In our country, this problem began to be actively discussed in the 1990s. And it must be said that the producers of paracetamol were the instigators then. This medicine was the main alternative to aspirin for influenza and other conditions when it was necessary to reduce fever.
Links[edit]
- ^ a b c d e f g h i j
"NINDS Reye's Syndrome Information Page".
NINDS
. September 25, 2009 archiving from the original on August 1, 2016. Retrieved August 8, 2021. - ^ B s d e g h i J k l m p o r d t y t
Pugliese, A
; Beltramo, T; Torre, D. (October 2008). "Reye's and Reye's-like syndromes." Biochemistry and cell functions
.
26
(7): 741–6. DOI: 10.1002/cbf.1465. PMID 18711704. S2CID 22361194. - ^ B s d e Schrör
, K (2007).
"Aspirin and Reye's syndrome: a review of the evidence." Pediatric drugs
.
9
(3): 195–204. DOI: 10.2165/00148581-200709030-00008. PMID 17523700. S2CID 58727745. - McMillan, Julia A.; Feigin, Ralph D.; DeAngelis, Catherine; Jones, M. Douglas (2006). Oski Pediatrics: Principles and Practice
. Philadelphia: Lippincott Williams and Wilkins. item 2306. ISBN. 9780781738941. Archived from the original on August 15, 2021. - Jump up ↑
Knight, J. (2009).
"Reye's syndrome". Healthy child care
.
12
(4). Archived from the original on May 22, 2013. - Boldt, D. W. (February 2003). "Reye's syndrome". John A. Burns School of Medicine, University of Hawaii. Archived from the original on March 6, 2013.
- "What is Reye's syndrome?" . National Reye's Syndrome Foundation. 1974. Archived May 11, 2013.
- "Reye's Syndrome". KidsHealth.org
. Nemours Foundation. Archived from the original on February 6, 2015. Retrieved February 6, 2015. - Jump up
↑ Ku AS, Chan LT (April 1999).
"First human case of H5N1 avian influenza infection with complications of adult respiratory distress syndrome and Reye's syndrome." Journal of Pediatrics and Child Health
.
35
(2): 207–9. DOI: 10.1046/j.1440-1754.1999.t01-1-00329.x. PMID 10365363. S2CID 7985883. - ^ a b c
Orlovsky JP, Hanhan UA, Fiallos MR (2002).
“Does aspirin cause Reye's syndrome? The case is against.” Drug safety
.
25
(4): 225–31. DOI: 10.2165/00002018-200225040-00001. PMID 11994026. S2CID 20552758. - Orlovsky JP (August 1999). “What happened to Reye's syndrome? Did he really exist? Critical Care Medicine
.
27
(8):1582–7. DOI: 10.1097/00003246-199908000-00032. PMID 10470768. - Jump up
↑ Hurwitz, E. S. (1989).
"Reye's Syndrome". Epidemiological Reviews
.
11
: 249–253. DOI: 10.1093/oxfordjournals.epirev.a036043. PMID 2680560. - Gosalakkal JA, Kamoji V (September 2008). "Reye's Syndrome and Reye's Syndrome". Child Neurology
.
39
(3):198–200. DOI: 10.1016/j.pediatrneurol.2008.06.003. PMID 18725066. - "New recommendations for oral use of salicylate gels for children under 16 years of age" (press release). Medicines and Healthcare Products Regulatory Agency. April 23, 2009 archived from the original on April 26, 2009. Retrieved May 1, 2009.
- "2.9 Antiplatelet drugs." British National Formulary for Children
. British Medical Association and Royal Pharmaceutical Society of Great Britain. 2007. p. 151. - Jump up ↑
Hall SM, Plaster PA, Glasgow JF, Hancock P (1988).
"Pre-administration of antipyretics for Reye's syndrome". Arch. dis. Child
.
63
(7):857–66. DOI: 10.1136/adc.63.7.857. PMC 1779086. PMID 3415311. - Autret-Leca E, Jonville-Béra AP, Llau ME et al (2001). "Incidence of Reye's syndrome in France: a hospital-based study." Journal of Clinical Epidemiology
.
54
(8):857–62. DOI: 10.1016/S0895-4356(00)00366-8. PMID 11470397. - Reye RD, Morgan G, Baral J (1963). “Encephalopathy and fatty degeneration of internal organs. Illness in childhood." Lancet
.
2
(7311): 749–52. DOI: 10.1016/S0140-6736(63)90554-3. PMID 14055046. - Starko KM, Ray CG, Dominguez LB, Stromberg WL, Woodall DF (December 1980). "Reye's syndrome and salicylate use." Pediatrics
.
66
(6):859–864. PMID 7454476. - Mortimore, Edward A. Jr.; and others. (June 1, 1980). "Reye's Syndrome - Ohio, Michigan". Morbidity and Mortality Weekly Report
.
69
(29): 532, 810–2. PMID 7079050. Archived from the original on June 11, 2008. - "Aspirin Labels to Warn for Reye's Syndrome". New York Times
. Associated Press. March 8, 1986. Archived March 5, 2016.
In the mirror of statistics
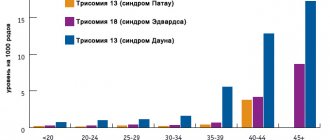
The abandonment of aspirin as an antipyretic for influenza and other viral infections in children quickly led to the fact that Reye's syndrome practically disappeared. This is how it looked in the mirror of American statistics. From 1980 to 1997, 1,207 cases of this syndrome were reported in children under 18 years of age. The peak incidence occurred in 1980 (555 cases). In 1985 and 1986, when information about Reye's syndrome was already known in the community and many people stopped using aspirin in children, approximately 100 cases were recorded per year. And after the inclusion of an official warning in the instructions for medications, the incidence began to decrease even more: from 1987 to 1993, about 36 cases of Reye's syndrome were recorded per year, and from 1994 to 1997 - only 2 cases per year on average. There are no statistics for Russia, but today isolated cases of the disease are recorded in the world.
Russian cold is useful. How do walks save children from colds? More details
Signs and symptoms[edit]
Reye's syndrome goes through five stages: [5] [6] [7]
- Stage I Vasoconstrictor rash on the palms and soles
- Constant severe vomiting that does not go away due to refusal to eat.
- Generalized lethargy
- Confusion
- Nightmares
- No fever is usually present [8]
- Headache
- Stupor
- Continuation of stage I and II symptoms
- Deepening coma
- Very fast onset after stage IV
Was there Reye's syndrome?
In recent years, many doctors have begun to doubt the presence of Reye's syndrome in general and that aspirin causes it. Articles with self-explanatory titles began to appear: “Is Reye's syndrome still the correct diagnosis?” or “Does aspirin cause Reye's syndrome?”
And there are reasons for such views. It turned out that in addition to aspirin, similar conditions can be caused not only by many other antipyretic drugs, but also by drugs from completely different groups. Similar syndromes have been recorded without these medications at all and without infections. A new diagnosis has appeared - “Rhea-like syndrome”.
Providing medical care
At the slightest suspicion that a child is developing Reye's syndrome, he must be urgently hospitalized; as a rule, an ambulance brings such patients to the intensive care unit. At the initial stage, treatment is more symptomatic and has the main task of stopping the dangerous changes that have begun in the body.
In medical practice, it is customary for this disease to use corticosteroids (most often Prednisolone), which help reduce the risk of inflammation in brain tissue, vitamin K, Mannitol to prevent brain swelling, as well as the introduction of electrolytes to restore water balance, and a glucose solution is also administered to restore its balance, as well as to maintain the body.
In addition, the introduction of fluid helps to remove ammonia from the body more quickly, but the doctor must always maintain a balance, since excess fluid can cause cerebral edema. Treatment is also aimed at correcting blood circulation.
For this purpose, plasma may be administered, a blood transfusion may be performed, or dialysis may be performed. In some cases, when breathing is already impaired, tracheal intubation with hyperventilation may be performed.
It is very important during treatment to systematically monitor the value of arterial and intracranial pressure. The value of the latter should be no more than 15 torr. If the value exceeds the norm, Furosemide is used in the form of injections to reduce pressure. During treatment, respiratory rate and pulse parameters are constantly monitored. In case of deviations, adequate treatment is prescribed with a wide arsenal of drugs.
Bad mitochondria disease
It has been suggested that Reye's syndrome hides some inborn metabolic disorders that were not recognized at the time and only appeared against the background of critical conditions caused by infection and medications that aggravate them. And today it is already clear that the basis of most cases of Reye's syndrome is indeed a congenital functional failure of mitochondria. These formations in our cells play the role of power plants - they produce the energy necessary for life. But in extreme situations they may not withstand it and “break”. Brain damage and fatty degeneration of the liver and other organs in Reye's syndrome are all a consequence of the “failure” of mitochondria. Many children who survived this disease developed complications related to the deficiency of these living energy stations. They became chronic patients requiring constant treatment.
Training for immunity. Is a child afraid of colds? More details
Clinical symptoms
Due to metabolic disorders in the blood, there is a sharp decrease in sugar levels, while ammonia and acids become more than necessary. The liver swells, with the transformation of cellular tissue into fatty tissue. The most severe manifestation of Reye's syndrome is progressive cerebral edema with convulsions and loss of consciousness.
Symptoms of the disease may appear several days after the child gets sick with the flu or chickenpox. Often this happens already on the road to recovery.
The course of Reye's syndrome may differ in different patients, but, in general, two phases are typical for it. After the onset of the underlying illness (ARVI, influenza, chicken pox or other infection), as a rule, 5 to 7 days pass. The initial symptoms are vomiting and nausea, which are difficult to stop, with sudden changes in the spheres of perception and psyche. There may be:
- mild amnesia;
- visual and auditory impairments;
- disorientation in space;
- dilated pupils;
- severe anxiety.
If the condition is not stopped in time, unresponsiveness quickly worsens, with the appearance of decortication posture, convulsions, loss of consciousness and, as a result, respiratory arrest. Focal neurological symptoms are usually not observed. The liver is enlarged in 40% of cases, without manifestations of jaundice.
What to do?
What does all this mean for parents and their children? Should they avoid not only aspirin, but also other medications for the flu? Should this also be done for other viral infections?
First of all, there is no need to panic. Apparently, the likelihood of getting Reye's syndrome is not for everyone, but for those who have congenital problems with mitochondria. True, in victims of this disease they were usually hidden before its development. Is it possible to somehow identify them in this state? No, but there are signs that make them more likely. This happens if blood relatives in the family had or have congenital problems with metabolism or mitochondrial dysfunction. In the same way, special care should be taken if among such relatives there were hereditary encephalopathies (brain diseases) or other brain diseases. Many of them can be accompanied by problems with mitochondria.
Article on the topic
And wash, and lose weight.
Non-standard ways to use aspirin Secondly, the use of aspirin and other antipyretics in children is best avoided and non-drug methods of reducing fever are used more often. To do this, it is often recommended to wipe the skin under the arms and in the popliteal fossae with vinegar. But the famous pediatrician, advisor to the director of the National Medical Research Center for Children's Health, Professor Vladimir Tatochenko has a different opinion on this matter: “Under no circumstances use vinegar, forget about it, there will definitely be some mother who uses vinegar essence instead, and there will be a burn.” .
Ordinary lukewarm water is much more effective than vinegar. And you need to wet the entire surface of the body. At the same time, the child must be kept open in a room without drafts and with normal air temperature to avoid hypothermia. You can lubricate your skin with vodka in the same way. The treatment is based on the fact that alcohol and water, evaporating from the skin, take away heat and thereby reduce the temperature.” Thirdly, if the child tolerates the temperature satisfactorily, then it does not need to be reduced to 39 degrees. If it does come down to the need to take antipyretic drugs, then it is better to give children drugs with ibuprofen or paracetamol.
Versions about the reasons
The etiology and pathogenesis of Arnold-Chiari syndrome remain unspecified. Chiari suggested that the displacement of the cerebellum and medulla oblongata occurs due to intraembryonic hydrocephalus, which occurs as a result of stenosis of the Sylvian aqueduct - a narrow canal 2 cm long that connects the third and fourth ventricles of the brain.
Hydrocephalus is a pathological condition characterized by excessive accumulation of cerebrospinal fluid (CSF) in the cerebrospinal fluid spaces of the brain.
Cleland believed that the anomaly was associated with primary underdevelopment of the brain stem. In 1938, Canadian neurosurgeon Wilder Penfield (1891–1976) and his colleague proposed the “traction theory”: during the process of growth, the fixed spinal cord pulls the higher parts into the spinal canal cavity. In the "unified" theory, David G McLone and Paul Knepper in 1989 proposed that the primary neural tube defect is a leak of cerebrospinal fluid and insufficient expansion of the ventricular system, which leads to the formation of a reduced posterior fossa. However, subsequent studies indicate that there are different variants of Arnold-Chiari pathology: with and without a decrease in the posterior cranial fossa, with and without impaired cerebrospinal fluid outflow. Familial cases of MAC type 2 have been described, but the role of genetic factors has not yet been sufficiently studied.