Treatment of endometriosis is a long and painstaking process, which, unfortunately, is not always successful. Modern protocols require an integrated approach consisting of surgery and drug therapy. Drugs for the treatment of endometriosis are used independently in cases where surgery is not possible. Basically, these are hormones or their synthetic analogues.
The most popular drugs for the treatment of endometriosis today are:
- combined oral contraceptives (COCs)
- gonadotropin releasing hormone agonists
- synthetic analogues of testosterone and progesterone
Birth control pills
Contraceptives were among the first drugs to treat endometriosis. At first, single-phase progestins containing only gestagens were used. They suppress the processes of proliferation and cyclic changes in the endometrium both in the uterus itself and in endometriotic foci. After some time, sclerosis and regressive development of the lesions are observed. With long-term use, these drugs suppress the synthesis of gonadotropic hormones. As a result, pain and other manifestations of the disease are reduced. The most common side effect of this therapy is irregular bleeding. Today, gestagen drugs have slightly lost their relevance, giving way to estrogen-gestagen drugs.
Among the representatives of this group, the following drugs are currently prescribed:
- Duphaston
- Norkolut
- Premalut
Over time, to reduce side effects and be more effective, COCs containing estrogens and gestagens began to be used. The course involves continuous use for 3-6 cycles of the following drugs:
- Janine
- Yarina
- Diana is 35
- Jess
- Claira
- Dimia
The drugs create a specific hormonal background in a woman’s body that simulates a false pregnancy. The result is approximately the same as when taking gestagens, endometrial proliferation decreases, endometriosis foci become sclerotic and decrease in size, new ones do not appear. In approximately 80% of women, regular use of estrogen-gestagen contraceptives relieves spasms and pain.
Myomectomy
This organ-preserving technique is considered the “gold” standard in the treatment of fibroids in clinics in Western Europe and America. During the operation, the myomatous nodes are “husked”, removed, and the body of the uterus is sutured. The presence of a capsule allows the operation to be performed without damaging the myometrium.
But myomectomy can be performed in three ways: using an open technique, laparoscopy or resectoscopy; in any case, the operation allows not only to avoid organ removal, but also preserves the woman’s reproductive abilities.
I always give preference to laparoscopic surgery, among the advantages of which are: minimal tissue trauma, rapid recovery, painlessness and excellent cosmetic results. I have developed and patented a unique technique that has been successfully used for more than 12 years. Using this technique, I am able to remove even large and complexly located myomatous nodes without blood loss, with the formation of a reliable scar on the uterine wall and the absence of adhesions, which is important for future pregnancy and childbirth. Many of my patients who were diagnosed with infertility, after myomectomy performed in our clinic, were able to safely give birth to a healthy child.
Analogues of male hormones for the treatment of endometriosis
Androgen-methyltestosterone analogues are the first drugs for the treatment of endometriosis, which began to be used in the treatment of this disease approximately forty years ago. The main purpose of their use, like contraceptives, is to suppress the menstrual cycle and the associated proliferation of the endometrium. Tablets were prescribed for the treatment of endometriosis at a dose of 5-10 mg for six months. Nowadays, 17a-ethynyl-testosterone derivatives, for example, danazol, are more common from this group. The drug reduces the level of gonadotropic hormone and blocks progesterone, estrogen and androgen receptors in the ovaries.
Danazol has many side effects, including:
- weight gain
- fatty seborrhea
- swelling
- acne
- mammary atrophy
- change in sexual desire
- symptoms of menopause (hot flashes, sleep disturbances, irritability, fatigue, depression, cycle irregularities and bleeding between periods)
- an increase in the level of low-density lipoproteins in the blood, which increases the risk of cholesterol plaques in the coronary vessels, angina pectoris, and heart attack
Approximately the same side effects occur when taking synthetic progesterone analogues, such as Provera.
Also included in this group are drugs such as:
- Duphaston (dydrogesterone)
- Visanne (dienogest)
- Orgametril (linestrenol)
The duration of taking the drugs is 6-8 months. Quite often, after completing the course, women experience relapses. Now this group of drugs is rarely used, they have been replaced by birth control pills for the treatment of endometriosis and more modern drugs.
Relevance
Endometriosis is
a pathological process in which benign growth of tissue occurs outside the uterine cavity, similar in morphological and functional properties to the endometrium [1]. Despite the existence of many controversies regarding the mechanisms responsible for its pathogenesis and progression, it is widely known that endometriosis is an estrogen-dependent chronic inflammatory disease [2], and genetic and epigenetic mechanisms are also considered [3].
The problem of treating endometriosis (both internal and external) remains unresolved to this day. The main goals of treatment for this disease are: removal of the focus of endometriosis; reduction in pain intensity; infertility treatment; prevention of progression; prevention of relapses, which reduces the need for radical surgery and allows preserving a woman’s reproductive function [1].
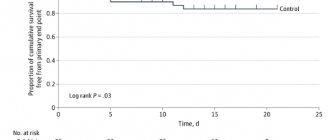
The variety of clinical manifestations and variability of responses to hormonal therapy require an individual approach to each specific case. According to the practice committee of the American Society for Reproductive Medicine, “endometriosis should be considered a chronic disease that requires a lifelong treatment plan to maximize the use of medical options and prevent repeated surgical procedures” [4].
Deep infiltrative endometriosis is a form of endometriosis in which pathological tissue can penetrate up to 5 mm below the surface of the affected structure [5]. The frequency of deep infiltrative forms is 20% of all cases of the disease, with the uterosacral ligaments being the most common location [6]. Two pathogenetic mechanisms explain the pain associated with deep infiltrative endometriosis: chronic inflammation associated with the metabolic activity of the ectopic epithelium, and secondary fibrosis caused by the invasion of endometriotic glands into scar tissue [7]. Treatment of deep infiltrative endometriosis can be either surgical, aimed at restoring normal anatomy by removing endometriotic lesions, or conservative (hormonal). Deeply infiltrating endometriosis causes the most severe pain, with potentially serious clinical consequences and the greatest risk if surgery is performed. Patients with this pathology should be considered a high-risk group, and progestins should be prescribed as first-line therapy [8]. Numerous published studies indicate that the choice of tactics aimed at surgical treatment of deep infiltrative endometriosis is in many cases considered a difficult task, because the operation can be associated with significant technical difficulties and the risk of serious complications [9]. With deep infiltrative endometriosis, the most complete excision of the lesions is required to reduce symptoms associated with the lesion [10]. However, surgical treatment is not always adequate. Thus, according to some authors, the rate of postoperative recurrence of endometriosis was 30% and 43% 4 and 8 years after surgery, respectively [11]. Therefore, there remains a need for effective, safe and well-tolerated drug therapy that can be used long-term if necessary. To reduce the frequency of recurrence and intensity of pelvic pain, conservative therapy, primarily hormones, is required [7, 12, 13]. However, the problem of targeted selection of a drug for drug therapy continues to be a priority. The principle of “no more than one operation in a patient with endometriosis” or an attempt to avoid surgical treatment altogether force us to choose not only highly effective, but also safe medications. Most international recommendations include combined oral contraceptives (COCs) and progestins as first-line medications. However, COCs do not have officially registered indications for the treatment of endometriosis, as well as clinical evidence of effectiveness [14]. The potential adverse effect of long-term COC use on the progression of endometriosis should be considered. In contrast, there are randomized controlled trials that support the use of progestins, not only for the treatment of pelvic pain associated with endometriosis, but also for suppressing the growth of endometrial ectopia. Therefore, they should be considered as first-line drugs in the treatment of endometriosis [15].
Gonadotropin-releasing hormone (GnRH) agonists cannot be considered as drugs of choice for long-term therapy due to the adverse vasomotor effects and decreased bone mineral density associated with estrogen deficiency [16].
Gonadotropin releasing hormone agonists as drugs for the treatment of endometriosis
This group of drugs is a synthetic analogue of pituitary releasing hormones, which are responsible for the synthesis of latinizing and follicle-stimulating hormone. Their decrease in the blood causes a decrease in the production of progesterones by the corpus luteum of the ovaries in the second half of the cycle. As a result, there is no proliferation of the endometrium in endometriotic lesions. Estrogen levels also decrease, leading to a state of artificial reversible menopause. The drugs are administered by injection daily or once every 28 days under the skin of the abdomen. There are medications in the form of sprays that are sprayed into the nose.
The most well-known drugs for the treatment of endometriosis from this group are:
- Leuprolide acetate or Lupron
- Nafarelina acetate or Sinarel
- Goserelin acetate or Zoladex.
Although today gonadotropin releasing hormone agonists are considered the most acceptable for drug therapy for endometriosis, their side effects are quite serious. First of all, these are symptoms of menopause. It includes:
- tides
- irritability
- sleep disorders
- decreased performance
- mood swings up to depression
- weight gain
- limb cramps and signs of osteoporosis due to impaired calcium absorption
- increased risk of angina and heart attack
In rare cases, menopause may be irreversible. Medicines in this group are not recommended to be taken for more than six months in a row.
In what cases is Mirena prescribed for adenomyosis?
Adenomyosis is a gynecological pathology in which the endometrium grows into the muscular layer of the uterus. The progression of the disease is accompanied by pathological symptoms, disruption of the reproductive system, and the inability to conceive and bear a child. Mirena for uterine adenomyosis helps stop the uncontrolled growth of the endometrium and relieve unpleasant symptoms.
The intrauterine device is installed only according to doctor's indications. The drug is recommended in the following cases:
Progressive internal adenomyosis, manifested by a pronounced clinical picture. A woman is worried about severe pain in the lower abdomen, heavy, prolonged menstrual bleeding, and discomfort during sexual intercourse.
- Uterine leimioma.
- Endometrial hyperplasia.
- Menstrual irregularities.
- Extensive damage by foci of adenomyosis of the myometrium.
- Heavy uterine bleeding, contributing to the development of iron deficiency anemia.
An intrauterine device is installed in women who have already given birth to a child. In exceptional situations, the drug is also used for nulliparous women, but in this case there is a high risk of prolapse of the system from the uterus. Before installation, the doctor sanitizes the vagina and cervix to make sure there are no active inflammatory processes. It is worth noting that after implantation, a woman will not be able to get pregnant for 5 years; this fact is also taken into account by the doctor before prescribing the drug.
Scheme for using a hormonal IUD
Before inserting an intrauterine device, simple preparation is required, including the following steps:
- Initial examination by a doctor. During the procedure, the gynecologist assesses the general condition of the patient’s genital tract and excludes contraindications for the use of the drug.
- Testing for sexually transmitted infections. Laboratory procedures such as bacterial culture and survey smear will help identify possible problems. If necessary, tests for viral and intracellular infection are prescribed - PCR, ELISA.
- Ultrasound of the pelvic organs. Ultrasound examination helps to assess the condition of the uterus and appendages, diagnose concomitant pathologies, and determine the degree of progression of adenomyosis.
If there are no contraindications to the insertion of an intrauterine device, the doctor will agree on the date and time of the procedure. The Mirena hormonal system is installed on the 3rd – 7th day of the cycle - at the end of menstruation. During this period, the cervix is dilated, which allows the IUD to be inserted inside without hindrance.
The technology for maintaining the Mirena therapeutic system includes the following stages:
- Control examination and treatment of the genital mucosa with an antiseptic solution.
- Introduction of the mirror.
- Grasp the upper lip of the cervix with special gynecological forceps.
- Checking the patency of the cervical canal and the depth of the uterine cavity with a probe.
- Insertion of a guidewire and an intrauterine device through it.
- Removing the conductor.
After the guide is removed, the IUD remains in the uterus. All manipulations are carried out under ultrasound control, which significantly reduces the risk of side effects. After 5 years the sprial will need to be removed. Premature removal of the system is carried out in the following situations:
- development of unwanted side effects;
- complications arising from the installed IUD;
- pregnancy planning.
The principle of operation of the hormonal intrauterine system
The Mirena therapeutic spiral contains the hormone levonorgestrel from the progesterone group. The hormone is enclosed in a special housing and protected by a membrane that regulates its release. Progestogen is released directly into the uterine cavity, affecting the functioning of the reproductive system.
The principle of operation of the hormonal intrauterine system:
- Reduces the sensitivity of receptors to specific hormones such as estrogen and progesterone.
- Makes the uterine mucosa immune to the female sex hormone estradiol.
- Prevents the growth of new pathological tissues.
Thanks to these medicinal properties, the coil for uterine adenomyosis helps to significantly improve the patient’s condition:
- Normalize the amount of menstrual flow, making it moderate.
- Eliminate pain and discomfort.
- Reduce the risk of uterine bleeding.
- Eliminate secondary anemia caused by excessive blood loss
Side effects and contraindications
After installation of the Mirena therapeutic system, side effects rarely develop, but they are still possible. Among the most common complications are the following:
- Individual intolerance to the drug, accompanied by pathological reactions and deterioration in general well-being.
- Frequent headaches, nausea, depressed mood, decreased libido.
- Periodic abdominal pain, bloating.
- Sudden jumps in blood pressure.
- Infections of organs located in the abdominal cavity.
- Failure of the menstrual cycle, manifested by a prolonged absence of menstruation.
Against the background of an implanted intrauterine device, the condition of the skin may worsen. Blackheads, acne, and inflammation appear on the face and body. In extremely rare cases, after the installation of an IUD, cysts form in the myometrium.
The Mirena therapeutic system is not prescribed to patients with suspected pregnancy. In this case, the woman must undergo tests to make sure there is no conception. Also, the IUD is contraindicated for implantation if the following pathologies are diagnosed:
- neoplasms of a malignant nature;
- uterine fibroids larger than 5 cm;
- inflammatory processes in the organs of the genitourinary system;
- congenital or acquired immunodeficiency;
- uterine bleeding of unknown etiology;
- individual intolerance to the active component of the drug.