A urine test is a study that helps to obtain information about the condition of the baby’s body and the correctness of its development. At first glance, donating urine does not present any difficulties. However, parents of small children have many questions: how to collect urine for analysis of a newborn, how to properly prepare for this, how much urine is needed for the objectivity of the study. If certain requirements are not met, parents expect to hear from the doctor a request to retest the urine, since the test results will be uninformative.
Why do you need a general urine test?
Children undergo a general urine test regularly at each medical examination. In the first days of life, at 1, 3, 6, 12 months, then at 2 and 3 years, at each examination before entering the children's group. The doctor may also prescribe this analysis during the treatment of acute respiratory viral infections and other diseases in order to know how the infection affected the functioning of the kidneys and digestive organs. Bacterial infections often disrupt the functioning of the kidneys and other organs of the genitourinary system, which is why it is so important to prevent irreversible consequences in a timely manner. Urinalysis helps diagnose various chronic diseases.
Presence of protein in urine (proteinuria):
- nephrotic syndrome;
- diabetic nephropathy;
- glomerulonephritis;
- nephrosclerosis;
- impaired absorption in the renal tubules (Fanconi syndrome, heavy metal poisoning, sarcoidosis, sickle cell disease);
- multiple myeloma (Bence Jones protein in urine) and other paraproteinemias;
- impaired renal hemodynamics in heart failure, fever;
- malignant tumors of the urinary tract;
- cystitis, urethritis and other urinary tract infections.
1.6.Glucose in urine Glucose in urine is normally absent or found in minimal quantities, up to 0.8 mmol/l, because In healthy people, all blood glucose, after being filtered through the glomerular membrane, is completely reabsorbed back into the tubules. When the concentration of glucose in the blood is more than 10 mmol/l - the renal threshold is exceeded (the maximum ability of the kidneys to reabsorb glucose) or when the renal threshold is reduced (renal tubular damage), glucose appears in the urine - glucosuria is observed.
Detection of glucose in urine is important for the diagnosis of diabetes mellitus, as well as monitoring (and self-control) of antidiabetic therapy.
Reference values: negative.
When can a doctor order a test?
Urinalysis is prescribed in three main cases:
- When visiting a clinic with suspected pathological processes and diseases. General urine analysis is a basic study, which is traditionally included in the list of mandatory diagnostic measures;
- After an illness, to assess the results of therapeutic measures, monitor the general condition and possible complications in the functioning of the genitourinary system;
- During the period of scheduled preventive examination and upon admission to a new children's team.
What types of urine tests are there?
There are several types of urine tests that a pediatrician or specialist can prescribe for a child:
- A general urine test, which is prescribed in tandem with a blood test. Helps evaluate the physical and chemical composition: density, color;
- Biochemical urine analysis. The content of protein, glucose, amylase, creatinine, sodium, potassium, phosphorus, magnesium, microalbumin, urea and uric acid is calculated in the urine;
- Urinalysis according to Nechiporenko. Demonstrates the number of leukocytes and erythrocytes in morning urine and allows you to diagnose pathological processes in the kidneys and urinary tract;
- Urine analysis according to Zimnitsky. Prescribed to assess kidney function. In this case, daily urine is collected, its volume, density, and the ratio of daytime and nighttime portions are assessed. The analysis is carried out when diagnosing various diseases.
Child health: basic tests
As you know, most children “don’t like” coming to medical institutions, and examining a child is a real challenge for parents. In such conditions, the diagnosis of young patients should be based on the “all at once” principle. But what kind of tests are we talking about if the goal is a preventive examination of the child’s health?
Complete blood count with leukocyte formula
Many parents are already familiar with this analysis, because it is prescribed for any inflammation, including ARVI, to assess the severity and origin (viruses/bacteria) of the process.
However, the test can also reveal other common problems, such as anemia and dehydration.
Anemia in children is most often due to iron deficiency. And a lack of microelement reduces the body’s resistance to infections, both bacterial and viral, and also slows down recovery. Therefore, children with anemia are often classified as frequently ill, and their “sick leave” lasts for 2-3 weeks.
With anemia, there is also a deterioration in the condition of the skin (dryness, peeling, inflammation) and its healing, as well as hair loss. And the general condition of the child, depending on the severity of the pathology, can vary between slightly increased fatigue and noticeable weakness.
Anemia in a blood test is indicated by a decrease in red blood cells and hemoglobin, as well as deviations in erythrocyte indices (MCV, MCH, MCHC), the decrease of which is often associated with iron deficiency.
You can check your iron levels using a blood test. True, the study allows us to identify only existing iron abnormalities, but does not make it possible to predict the risk of their occurrence.
A blood test for ferritin does not have such a deficiency, since it does not reflect the concentration of iron in the blood, but its reserves in the body. A decrease in the indicator indicates the depletion of “iron storage”, and “warns” of a high risk of anemia long before the onset of symptoms.
General analysis of urine and feces
A general urine test is unfairly considered by many to be “secondary”, because most often a visit to it is associated with existing symptoms of a urinary infection (frequent urination, burning, etc.).
At the same time, the analysis makes it possible to detect some serious kidney diseases (for example, glomerulonephritis) at a very early stage, in the absence of any symptoms. A consultation with a doctor requires the appearance of red blood cells and an increase in protein in the urine.
The appearance of bilirubin in the urine and an increase in urobilinogen indicate liver or gallbladder disease, or the destruction of red blood cells (hemolysis), and ketones and glucose are markers of possible diabetes or other metabolic pathologies.
Diagnosis of helminthiases
It is no secret that children often ignore simple sanitary rules, both regarding “dirty hands” and certain food products (berries, fruits, etc.). Therefore, it is not surprising that “little” patients constitute the main risk group for helminthiasis.
In this case, infection does not appear immediately. And only after some time may symptoms of allergies, skin pathologies, deficiency conditions (lack of iron, vitamins, etc.) and other nonspecific pathologies appear.
And some of the helminths are able to live in the liver and even in the brain, forming cysts and destroying the organ.
You can check for the presence of helminths using a stool enrichment method (PARASEP), which makes it possible to detect 16 types of parasites, or a blood test for IgG antibodies to the most common of them (for example, the “Diagnostics of Parasitic Diseases” complex).
It should be remembered that these studies do not exclude, but complement each other. Since the “cunning” of the life cycle of parasites does not always make it possible to detect their eggs in the material, and the “special relationship” with the immune system of the infected person can block the synthesis of specific antibodies.
Screening for endocrinological pathology
Diabetes mellitus today “spares” neither adults nor children and is the most common endocrinological problem.
At the same time, type 1 diabetes, unfortunately, requires lifelong insulin therapy, while type 2 diabetes can be cured in the early stages.
Therefore, the list of basic child health tests should include a blood test for glucose or, better yet, glycated hemoglobin, which reflects the average “sugar” level over the last 3 months.
Thyroid problems are the second most common problem after diabetes.
The thyroid gland controls all metabolic processes in the body and affects mental abilities. And a lack of thyroid hormones can lead to weight gain, decreased learning abilities and many other problems.
And to assess the “health” of the gland, a blood test for TSH, and free ones, is necessary.
How to collect urine: what not to do?
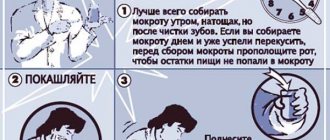
You should not use jars of canned food or baby food to collect urine. Poorly washed dishes and soap solution residues distort diagnostic results. It is also not recommended to collect biomaterial in the evening: morning urine is the most informative, and can be stored for no more than two hours. If you leave the material for analysis at home for a longer period, a precipitate may form and the reliability of the result will again decrease. It is best to collect urine from a child immediately after waking up; such material is considered the most informative.
How to collect urine correctly?
Urine must be transported carefully under certain temperature conditions. Severe frost or hot weather can negatively affect the diagnosis. If the weather outside is questionable, use a thermal bag. It is important to follow the following recommendations from pediatricians:
- Do not give your child unfamiliar foods the day before collecting urine, do not feed him vegetables and fruits that contain natural dyes;
- Maintain a normal temperature in the room; the baby should not overheat or freeze;
- Take care of the child’s mood - this also affects the result of the analysis, which may be distorted due to a poor emotional state;
- Try to collect the very first portion of morning urine, on an empty stomach before morning feeding.
Bacteria in urine:
- infections of the urinary system (pyelonephritis, urethritis, cystitis).
Yeast The detection of yeast of the genus Candida indicates candidiasis, which most often occurs as a result of irrational antibiotic therapy.
Reference values: negative
2.6. Inorganic sediment of urine (crystals), salts in urine Urine is a solution of various salts that can precipitate (form crystals) when urine stands. Low temperature promotes the formation of crystals. The presence of certain salt crystals in the urinary sediment indicates a change in the reaction towards the acidic or alkaline side. Excessive salt content in urine contributes to the formation of stones and the development of urolithiasis. At the same time, the diagnostic value of the presence of salt crystals in urine is usually small. Increased doses of ampicillin and sulfonamides lead to the formation of crystals.
Under physiological conditions, uric acid occurs in high concentrations of urine, after a heavy meat meal, after profuse sweating.
Reference values: none
Uric acid and its salts (urates):
- highly concentrated urine;
- acidic reaction of urine (after physical activity, meat diet, fever, leukemia);
- uric acid diathesis, gout;
- chronic renal failure;
- acute and chronic nephritis;
- dehydration (vomiting, diarrhea);
- in newborns.
Hygiene procedures before collecting urine
Improper hygiene often causes poor analysis and unreliable diagnosis, so the doctor may order the test again. It is best to ensure that all rules are followed in advance. Cleanliness of the baby’s organs is the basis for accurate results!
Bacteria often accumulate on skin folds and easily penetrate into the urine collection container. It is for this reason that most often the child’s test results are poor.
Many people wonder: how to properly wash a small child? If we are talking about babies, then you need to wash them from front to back, this applies to both girls and boys. This minimizes the risk of bacteria entering the genital area. You need to wash your child immediately before taking the test; this must be done quickly, since babies do not know how to endure. The use of herbal decoctions is strictly prohibited - they can cause an allergic reaction and provoke pain and itching in the baby.
Microscopy of urine sediment
Microscopy of urine components is carried out in the sediment formed after centrifugation of 10 ml of urine. Sediment consists of solid particles suspended in urine: cells, protein-formed casts (with or without inclusions), crystals, or amorphous deposits of chemicals.
2.1. Red blood cells in urine Red blood cells (blood cells) enter the urine from the blood. Physiological erythrocyturia is up to 2 red blood cells/μl of urine. It does not affect the color of urine. During the study, it is necessary to exclude contamination of urine with blood as a result of menstruation! Hematuria (the appearance of red blood cells, other formed elements, as well as hemoglobin and other blood components in the urine) can be caused by bleeding anywhere in the urinary system. The main reason for the increase in the content of red blood cells in the urine is renal or urological diseases and hemorrhagic diathesis.
Reference values: none; with microscopy - up to 2 in the field of view. Red blood cells in urine - exceeding reference values:
- urinary tract stones;
- tumors of the genitourinary system;
- glomerulonephritis;
- pyelonephritis;
- hemorrhagic diathesis (with intolerance to anticoagulant therapy, hemophilia, coagulation disorders, thrombocytopenia, thrombocytopathies);
- urinary tract infections (cystitis, urogenital tuberculosis);
- kidney injury;
- arterial hypertension with involvement of the renal vessels;
- systemic lupus erythematosus (lupus nephritis);
- poisoning with benzene derivatives, aniline, snake venom, poisonous mushrooms;
- inadequate anticoagulant therapy.
2.2. White blood cells in the urine An increased number of white blood cells in the urine (leukocyturia) is a symptom of inflammation of the kidneys and/or lower urinary tract. In chronic inflammation, leukocyturia is a more reliable test than bacteriuria, which is often not detected. With a very large number of leukocytes, pus in the urine is determined macroscopically - this is the so-called pyuria. The presence of leukocytes in the urine may be due to the presence of secretions from the external genitalia in the urine due to vulvovaginitis, or insufficiently thorough toileting of the external genitalia when collecting urine for analysis.
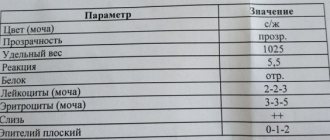
Reference values: none; by microscopy: boys - 0 - 3 in the field of view girls < 14 years old - 0 - 5 in the field of view
An increase in leukocytes in the urine is observed in almost all diseases of the kidneys and genitourinary system:
- acute and chronic pyelonephritis, glomerulonephritis;
- cystitis, urethritis, prostatitis;
- stones in the ureter;
- tubulointerstitial nephritis;
- lupus nephritis;
- kidney transplant rejection.
2.3. Epithelial cells in urine Epithelial cells are almost always present in urine sediment. Epithelial cells originating from different parts of the genitourinary system vary (usually squamous, transitional and renal epithelium are distinguished).
Squamous epithelial cells, characteristic of the lower parts of the genitourinary system, are found in the urine of healthy people and their presence usually has little diagnostic value. The amount of squamous epithelium in the urine increases with urinary tract infection.
An increased number of transitional epithelial cells can be observed in cystitis, pyelonephritis, and kidney stones.
The presence of renal epithelium in the urine indicates damage to the kidney parenchyma (observed in glomerulonephritis, pyelonephritis, some infectious diseases, intoxication, circulatory disorders). The presence of more than 15 renal epithelial cells in the field of view 3 days after transplantation is an early sign of the threat of allograft rejection.
Reference values: none; under microscopy: squamous epithelial cells: other epithelial cells - absent
Detection of renal epithelial cells:
- pyelonephritis;
- intoxication, intake of salicylates, cortisol, phenacetin, bismuth preparations, poisoning with salts of heavy metals, ethylene glycol);
- tubular necrosis;
- kidney transplant rejection;
- nephrosclerosis.
2.4. Cylinders in urine Cylinders are elements of cylindrical sediment (a kind of cast of renal tubules), consisting of protein or cells, and may also contain various inclusions (hemoglobin, bilirubin, pigments, sulfonamides). Based on their composition and appearance, there are several types of cylinders (hyaline, granular, erythrocyte, waxy, etc.).
Normally, renal epithelial cells secrete the so-called Tamm-Horsfall protein (absent in blood plasma), which is the basis of hyaline casts. Hyaline casts can be found in the urine in all kidney diseases. Sometimes hyaline casts can be found in healthy people. As a pathological symptom, they acquire significance when they are constantly detected and in significant quantities, especially when erythrocytes and renal epithelium are superimposed on them.
Granular casts are formed as a result of the destruction of tubular epithelial cells. Their detection in a patient at rest and without fever indicates renal pathology.
Waxy casts are formed from compacted hyaline and granular casts in wide-lumen tubules. They occur in severe kidney diseases with predominant damage and degeneration of the tubular epithelium, more often in chronic than in acute processes.
Erythrocyte casts are formed when red blood cells are layered on hyaline casts, and leukocyte casts are formed by leukocytes. The presence of red blood cell casts confirms the renal origin of hematuria.
Epithelial casts (rarely) are formed when the tubular epithelium is detached. Occurs with severe degenerative changes in the tubules at the onset of acute diffuse glomerulonephritis, chronic glomerulonephritis. Their presence in a urine test a few days after surgery is a sign of rejection of the transplanted kidney.
Pigment (hemoglobin) cylinders are formed when pigments are included in the composition of the cylinder and are observed with myoglobinuria and hemoglobinuria.
Cylinders are long structures consisting of mucus. Single cylindroids are found in urine under normal conditions. A significant number of them occur during inflammatory processes of the mucous membrane of the urinary tract. They are often observed when the nephritic process subsides.
Reference values: hyaline cylinders – single, others – absent
Hyaline casts in urine:
- renal pathology (acute and chronic glomerulonephritis, pyelonephritis, kidney stones, renal tuberculosis, tumors);
- hyperthermic conditions;
- heavy physical activity,
- high blood pressure;
- taking diuretics.
Granular casts (nonspecific pathological symptom):
- glomerulonephoritis, pyelonephritis;
- diabetic nephropathy;
- viral infections;
- lead poisoning;
- fever.
Waxy cylinders:
- chronic renal failure;
- kidney amyloidosis;
- nephrotic syndrome.
Red blood cell casts (hematuria of renal origin):
- acute glomerulonephritis;
- kidney infarction;
- renal vein thrombosis;
- malignant hypertension.
Leukocyte casts (leukocyturia of renal origin):
- pyelonephritis;
- Lupus nephritis in systemic lupus erythematosus.
Epithelial casts (most rare):
- acute tubular necrosis;
- viral infection (for example, cytomegalovirus);
- poisoning with salts of heavy metals, ethylene glycol;
- overdose of salicylates;
- amyloidosis;
- kidney transplant rejection reaction.
2.5. Bacteria in urine
Isolation of bacteria in urine has significant diagnostic value. Bacteria remain in the urine for no more than 1-2 days after the start of antibiotic therapy. The first morning urine sample is preferable for testing. The type of bacteria can be determined and the level of bacteriuria can be assessed, as well as the sensitivity of microorganisms to antibiotics can be determined using bacteriological urine culture.
Reference values: negative
How to collect a test from a baby?
For an older child, it is somewhat easier to collect the analysis. According to tradition, some parents patiently wait for about a 1-2 month old baby with a jar in their hands. However, there is an easier way: use a urine bag. This is a special container that is sold in pharmacies. It is glued to the skin in the perineum, and the urine is collected in a sterile container.
There is no reason to fear for the baby’s comfort: the children’s urinal is made of elastic, hypoallergenic, soft-to-touch materials. Its capacity is 100 milliliters. The baby will not have any marks on the skin after removing the device. The attached instructions describe all the steps in detail, so parents can easily solve the task without any problems.
How to avoid mistakes?
In order to exclude false results and not retake the urine test, it is important to avoid common mistakes:
- Do not take urine from the potty or wring out a diaper or diaper;
- Do not take urine samples from other than your first urination for analysis;
- Do not keep the material in the refrigerator in the evening and do not freeze it;
- Do not use dirty containers for delivery and transportation;
- Do not overtire your child and do not allow emotional overload;
- Do not get tested after taking medications or receiving injections.
Detection of ketone bodies in urine (ketonuria):
- diabetes mellitus (decompensated - diabetic ketoacidosis);
- precomatose state, cerebral (hyperglycemic) coma;
- long-term fasting (complete refusal of food or diet aimed at reducing body weight);
- severe fever;
- alcohol intoxication;
- hyperinsulinism;
- hypercatecholaminemia;
- isopropranolol poisoning;
- glycogenosis types I, II, IV;
- lack of carbohydrates in the diet.
1.10. Nitrites in urine Nitrites are absent in normal urine. In urine, they are formed from nitrates of food origin under the influence of bacteria, if the urine was in the bladder for at least 4 hours. Detection of nitrites in the urine (positive test result) indicates infection of the urinary tract. However, a negative result does not always exclude bacteriuria. Urinary tract infection varies among different populations and is dependent on age and gender.
Reference values: negative.
1.11. Hemoglobin in urine Hemoglobin is absent in normal urine. A positive test result reflects the presence of free hemoglobin or myoglobin in the urine. This is the result of intravascular, intrarenal, urinary hemolysis of red blood cells with the release of hemoglobin, or muscle damage and necrosis, accompanied by an increase in plasma myoglobin levels. It is quite difficult to distinguish hemoglobinuria from myoglobinuria; sometimes myoglobinuria is mistaken for hemoglobinuria.
Reference values: negative
Presence of hemoglobin in urine:
- severe hemolytic anemia;
- severe poisoning, for example, sulfonamides, phenol, aniline, poisonous mushrooms;
- sepsis;
- burns.
Presence of myoglobin in urine:
- muscle damage;
- heavy physical activity, including sports training;
- myocardial infarction;
- progressive myopathies;
- Rhabdomyolysis
Small tricks
Experienced parents share secrets that will help facilitate the testing procedure for their children. If your baby sleeps in a diaper, prepare yourself immediately before unfastening it. It is enough to open the diaper and the baby will start urinating because he will feel cool. To speed up the process, you can give a light abdominal massage or put the baby's feet in a warm bath. The sound of rushing water, which you can turn on on your phone, also helps. Follow the rules for taking tests, and the diagnostic results will be as reliable as possible!