pharmachologic effect
The drug is highly active and is a macromolecular complex of the proteolytic enzyme hyaluronidase. When taken, it has the following effects:
- relieves inflammation;
- eliminates swelling;
- promotes activation of humoral immunity;
- antifibrotic.
Longidaza improves tissue nutrition, eliminates adhesions, contractures, accelerates the resorption of bruises and hematomas, and also increases joint mobility.
The drug works best in the initial stages of the disease, preventing its progression and the development of complications.
Longidaza also enhances the effect of local anesthetics, increasing their bioavailability.
The medication is characterized by incredibly low toxicity and the absence of negative effects on the body.
Longidaza in complex therapy of chronic prostatitis
Chronic prostatitis is the most common urological disease in men aged 25–55 years and has great medical and social significance. A long-term inflammatory reaction in the prostate tissue, characteristic of chronic prostatitis, leads to the development of sclerosis. For the treatment and prevention of sclerotic processes in the prostate gland, peloid therapy, physiotherapy, and proteolytic enzymes are used. Clinical studies conducted in leading Moscow clinics on the use of the drug Longidaza in patients with chronic prostatitis of categories II and IIIA showed its safety and effectiveness. The use of the drug Longidaza against the background of standard therapy significantly contributed to the disappearance or reduction of symptoms of the disease, regression of inflammatory-proliferative changes in the prostate gland and reduced the frequency of relapses. Taking into account the modern understanding of the pathogenesis and pathomorphology of chronic prostatitis, it seems advisable to use Longidase not only in the treatment of this disease, but also to prevent sclerotic changes in the prostate gland.
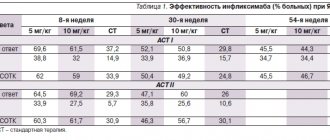
Table 1. Indicators of the effectiveness of Longidaza in patients with chronic prostatitis
Table 2. Indicators of the effectiveness of Longidaza in patients with chronic prostatitis
Table 3. Results of Doppler examination in patients with chronic prostatitis
Epidemiology
One of the most common urological diseases among men aged 25–55 years, chronic prostatitis, is the cause of 8 to 14% of outpatient visits to a urologist [1–3]. According to various sources, in Russia this disease affects from 8 to 35% of men aged 20–40 years [4, 5], and in the world, according to recent epidemiological studies, 2.2–9.7% of men [2]. In terms of prevalence, chronic prostatitis can be compared with diabetes mellitus and coronary heart disease [3], and in terms of its impact on quality of life - with myocardial infarction, angina pectoris, Crohn's disease and prostate cancer [6]. Chronic prostatitis reduces copulatory and reproductive functions in some patients, and its long course and frequent relapses determine its not only medical, but also social significance.
Pathogenesis
Chronic prostatitis is characterized by a long-term inflammatory reaction in the prostate tissue, leading to the development of sclerosis. Yu.V. Kudryavtsev, A.M. Chumakov [7, 8] note in their works that the inflammatory reaction in the prostate gland should be characterized not only and not so much by a temporary indicator, but primarily by the nature of the tissue reaction. It is the latter that is of greatest importance when choosing adequate treatment tactics. Few studies have been published on morphological changes in prostate tissue in various forms of chronic prostatitis, reflecting their relationship with clinical, laboratory and ultrasonographic manifestations of various types of prostatitis. Morphological signs of chronic prostatitis are detected in 6.3–16.3% of men, depending on age.
The inflammatory process in the prostate gland goes through a number of stages in its development: the alterative phase of cell damage, the exudative phase of the vascular response to damage (the release of fluid and blood cells from the vessels into the tissue), the proliferative phase of healing and repair. In the prostate tissue, the productive phase is layered in parallel with the existing or pre-existing episode of acute exudative inflammation onto the subsequent exudative phase. The completion of the productive phase of inflammation is accompanied by the formation of a focus of sclerosis. A change in tissue reactions in 86% of cases underlies the formation of a rather varied morphological picture in the prostate tissue in chronic prostatitis [8].
Treatment
The clinical picture characteristic of chronic prostatitis consists of symptoms of impaired urination, pain, and in the later stages, with the development of sclerosis, acute urinary retention and disturbance of the urodynamics of the upper urinary tract are possible. In the complex therapy of chronic prostatitis, a large number of different medications are used. To treat and prevent the development of sclerotic processes in the prostate gland, peloid therapy, physiotherapy and proteolytic enzymes are used.
The discovery of the first proteolytic enzyme dates back to 1886. In 1940, K. Meyer introduced the term “hyaluronidase” to designate a group of enzymes of various origins capable of breaking down acidic mucopolysaccharides. Hyaluronidase improves tissue permeability and trophism, increases the bioavailability of antibiotics, increases the elasticity of scarred areas in the prostate gland, and promotes the resorption of hematomas. The action of hyaluronidase is aimed at hydrolyzing the connective tissue matrix. Hyaluronidase has antigenic properties, and with repeated administration of large quantities, the formation of neutralizing antibodies is possible. Hyaluronidase has pronounced specific activity, has a prolonged effect, and is thermostable. It can be prescribed in the acute and chronic phase of inflammation.
Currently, the pharmaceutical industry produces a combination drug Longidase, which consists of hyaluronidase and high molecular weight azoximer bromide. Azoximer bromide (Polyoxidonium) is the first immunomodulatory drug created by R.V. Petrov et al. in 1997 at the Institute of Immunology, has an immunostimulating, detoxifying, antioxidant, membrane-stabilizing effect.
Clinical studies on the use of the drug Longidaza in patients with chronic prostatitis, conducted in leading clinics in Moscow, showed its safety and effectiveness. Let's look at some of them in more detail.
Clinical efficacy of Longidase
Under the guidance of Professor D.Yu. Pushkar conducted a blind, placebo-controlled, randomized trial, clinical phase II [9]. The study involved 56 patients aged 19 to 48 years with chronic bacterial and abacterial prostatitis. Patients of the main group (n = 28), in addition to standard therapy, received Longidase at a dose of 3000 IU in the form of intramuscular injections in 2 ml of 0.5% novocaine solution once every five days (course of 10 injections, treatment duration 50 days). The comparison group (n = 28) received standard therapy and placebo.
The following criteria were used to evaluate treatment results. An excellent result is the disappearance of all symptoms of the disease (the clinical index of chronic prostatitis is close to 0 points) and the normalization of objective data. A good treatment result is a pronounced regression of symptoms (the clinical index of chronic prostatitis is insignificant - 0–10 points) and positive dynamics of objective data. Satisfactory – slight regression of symptoms (clinical index of chronic prostatitis is moderate – 11–25 points) and positive dynamics of objective data or no effect. In the main group, the overall effectiveness of treatment was 82.1%; no effect was recorded in 17.8% of patients; in the comparison group, similar figures were 71.4 and 28.5%, respectively. At the same time, excellent and good results in cases of using Longidase were achieved in 57% of cases, and with standard therapy - in 32% (Table 1).
Professor V.P. Avdoshin et al. in two parallel groups, a comparative randomized placebo-controlled clinical trial was conducted on the use of the drug Longidaza in patients with chronic prostatitis [10].
The main group (n = 25) received, in addition to standard therapy, the drug Longidaza 3000 IU in the form of rectal suppositories in the amount of 20 per course: first, one suppository every other day - 10 suppositories, then one suppository every two days - another 10 suppositories. The course of treatment was 49 days. The control group (n = 20), in addition to standard therapy, received placebo in the form of rectal suppositories for 49 days. Dynamic observation was carried out for six weeks after cessation of treatment (Table 2).
When analyzing the questionnaire according to the system of summary assessment of symptoms for chronic prostatitis, there was a significant decrease in the clinical index of chronic prostatitis from 27 ± 9 to 13 ± 6 in the main group in comparison with a decrease in the clinical index of chronic prostatitis from 25 ± 8 to 19 ± 6 in the comparison group .
In the group receiving anti-sclerotic therapy, there was a decrease in prostate fibrosis, an enrichment of the vascular pattern, and an increase in the speed of blood flow in the vessels of the prostate gland according to Doppler ultrasound (Table 3).
A similar study with dynamic observation of patients for 12 months involved 90 patients aged from 18 to 50 years with an established diagnosis of chronic prostatitis of category II (chronic bacterial prostatitis), IIIA (chronic prostatitis / chronic pelvic pain syndrome with signs of inflammation) according to the classification, proposed by the US National Institutes of Health – the presence of inflammatory changes in the secretion of the prostate gland [11].
The subjects were randomly divided into four groups comparable in severity and prognosis of the disease. The first group consisted of 21 (23.3%) patients aged 20 to 50 years, for whom complex therapy, along with basic drug therapy, included magnetic laser therapy and enzyme therapy in the form of rectal suppositories of the drug Longidaza 3000 IU. The second group included 25 (27.8%) patients aged 18 to 49 years who, in addition to basic drug therapy, received enzyme therapy in the form of rectal suppositories of the drug Longidase 3000 IU. Administration regimen: one suppository rectally every other day - 10 injections, then one suppository rectally every two days - also 10 injections. The total course was 20 suppositories of Longidase 3000 IU. The third group consisted of 24 (26.7%) patients aged 19 to 50 years, who, along with basic drug therapy, received magnetic laser therapy. The fourth group included 20 (22%) patients aged 22 to 50 years who received only basic therapy.
When comparing the groups of patients who used the drug Longidaza with the group of patients who received magnetic laser therapy and the control group, the authors made significant conclusions. In relieving exacerbations of chronic prostatitis, the combination of magnetic laser and enzyme therapy with Longidase reliably demonstrated the highest effectiveness, this is due to the anti-edematous effects of magnetic laser therapy and the anti-sclerotic effects of enzyme therapy with Longidase. The inclusion of magnetic laser therapy and Longidase in the treatment of chronic prostatitis can significantly reduce the frequency of relapses of chronic prostatitis within a year after the end of treatment: two times compared with patients who received a combination with magnetic laser therapy, 1.8 times compared with patients who received a combination with Longidase, 2.8 times compared with patients receiving standard therapy.
Conclusion
Thus, the domestic drug Longidaza is an effective and safe means of complex therapy for bacterial and abacterial chronic prostatitis. The use of Longidase against the background of standard therapy significantly promotes the disappearance or reduction of symptoms of the disease, regression of inflammatory-proliferative changes in the prostate gland and reduces the frequency of relapses. Taking into account the modern understanding of the pathogenesis and pathomorphology of chronic prostatitis, it is advisable to use Longidaza not only in the treatment of this disease, but also to prevent sclerotic changes in the prostate gland.
Pharmacodynamics and pharmacokinetics
When the drug is administered by injection, it immediately enters the bloodstream, due to which the maximum concentration of the active substance is achieved in less than half an hour. The bioavailability of Longidase is about 90 percent, and it penetrates into any tissue of the human body. The half-life in this case is one day, and the drug is completely eliminated only after 5 days. It is excreted mainly by the kidneys, partly by the intestines.
When using suppositories, the maximum concentration is achieved only after 60 minutes. This dosage form has 70% bioavailability, and its half-life is extended to 2-3 days.
Longidaza, 20 pcs., 3000 IU, vaginal and rectal suppositories
Longidase® has hyaluronidase (enzymatic proteolytic) activity of prolonged action, chelating, antioxidant, immunomodulatory and moderate anti-inflammatory properties.
Prolongation of the action of the enzyme is achieved by covalent binding of it to a physiologically active high-molecular carrier (activated derivative of poly-1,4-ethylenepiperazine N-oxide, an analogue of the drug Polyoxidonium®), which has its own pharmacological activity. Longidase® exhibits antifibrotic properties, weakens the course of the acute phase of inflammation, regulates (increases or decreases depending on the initial level) the synthesis of inflammatory mediators (IL-1 and tumor necrosis factor-alpha), increases the humoral immune response and the body's resistance to infection.
The pronounced antifibrotic properties of Longidase® are ensured by the conjugation of hyaluronidase with a carrier, which significantly increases the resistance of the enzyme to denaturing influences and the action of inhibitors: the enzymatic activity of Longidase® is maintained when heated to 37 °C for 20 days, while native hyaluronidase loses under the same conditions your activity during the day. The Longidaza® preparation ensures the simultaneous local presence of the proteolytic enzyme hyaluronidase and a carrier capable of binding matrix components released during hydrolysis, enzyme inhibitors and stimulators of collagen synthesis (including iron, copper ions, heparin). Thanks to these properties, Longidaza® has not only the ability to depolymerize the connective tissue matrix in fibrogranulomatous formations, but also suppress the reverse regulatory reaction aimed at the synthesis of connective tissue components.
The specific substrate of testicular hyaluronidase is glycosaminoglycans (hyaluronic acid, chondroitin, chondroitin-4-sulfate, chondroitin-6-sulfate), which form the basis of the connective tissue matrix. As a result of depolymerization (breaking the bond between C1 acetylglucosamine and C4 glucuronic or induronic acids), glycosaminoglycans change their basic properties: viscosity decreases, the ability to bind water and metal ions decreases, the permeability of tissue barriers temporarily increases, fluid movement in the intercellular space is facilitated, and the elasticity of connective tissue increases. , which manifests itself in a decrease in tissue swelling, flattening of scars, an increase in the range of motion of joints, a decrease in contractures and prevention of their formation, and a decrease in adhesions.
Biochemical, immunological, histological and electron microscopic studies have proven that Longidaza® does not damage normal connective tissue, but causes destruction of connective tissue altered in composition and structure in the area of fibrosis.
Longidaza® does not have mutagenic, embryotoxic, teratogenic or carcinogenic effects.
The drug was well tolerated by patients; no local or general allergic reactions were noted.
The use of Longidase® in therapeutic doses during or after surgical treatment does not cause worsening of the postoperative period or progression of the infectious process; does not slow down bone tissue recovery.
Indications and contraindications for taking Longidaza
This drug is prescribed not only for the treatment, but also for the prevention of many diseases with connective tissue hyperplasia syndrome. It is used in the following medical fields:
- Gynecology: for inflammatory diseases of the genital organs, as well as for adhesions in the pelvic area.
- Pulmonology: fibrosing and sclerosing diseases of the lungs and respiratory tract, tuberculosis.
- Urology: chronic prostatitis and complicated cystitis.
- Surgery: prevention of adhesions after extensive abdominal surgery.
- Dermatovenereology: scleroderma, rough, keloid, disfiguring scars after various skin pathological processes.
There are also contraindications to the use of Longidase and, despite the low toxicity of the drug, there are quite a few of them:
- Individual intolerance to hyaluronidase.
- Oncological diseases.
- CKD.
- Bleeding and hemorrhage.
- Age under 18 years.
- Infections during the acute period of the disease.
Longidaza®
Longidaza® has hyaluronidase (enzymatic) activity of prolonged action, chelating, antioxidant, immunomodulatory and moderate anti-inflammatory properties.
Prolongation of the action of the enzyme is achieved by covalent binding of the enzyme to a physiologically active polymer carrier (azoximer). Longidase® exhibits antifibrotic properties, weakens the course of the acute phase of inflammation, regulates (increases or decreases depending on the initial level) the synthesis of inflammatory mediators (interleukin-1 and tumor necrosis factor - alpha), increases the humoral immune response and the body's resistance to infection.
The pronounced antifibrotic properties of Longidase are ensured by the conjugation of hyaluronidase with a carrier, which significantly increases the resistance of the enzyme to denaturing influences and the action of inhibitors: the enzymatic activity of Longidase is maintained when heated to 37 ° C for 20 days, while native hyaluronidase loses its activity under the same conditions during the day. The Longidaza® preparation ensures the simultaneous local presence of the enzyme hyaluronidase and a carrier capable of binding enzyme inhibitors and stimulators of collagen synthesis (iron, copper ions, heparin, etc.) released during hydrolysis of matrix components. Thanks to these properties, Longidaza® not only has the ability to depolymerize the connective tissue matrix in fibrogranulomatous formations, but also suppress the reverse regulatory reaction aimed at the synthesis of connective tissue components.
The specific substrate of testicular hyaluronidase is glycosaminoglycans (hyaluronic acid, chondroitin, chondroitin-4-sulfate, chondroitin-6-sulfate), which form the basis of the connective tissue matrix. As a result of depolymerization (breaking the bond between C1 acetylglucosamine and C4 glucuronic or induronic acids), glycosaminoglycans change their basic properties: viscosity decreases, the ability to bind water and metal ions decreases, the permeability of tissue barriers temporarily increases, fluid movement in the intercellular space is facilitated, and the elasticity of connective tissue increases. , which manifests itself in a decrease in tissue swelling, flattening of scars, an increase in the range of motion of joints, a decrease in contractures and prevention of their formation, and a decrease in adhesions. Biochemical, immunological, histological and electron microscopic studies have proven that Longidaza® does not damage normal connective tissue, but causes destruction of connective tissue altered in composition and structure in the area of fibrosis.
Longidaza® does not have mutagenic, embryotoxic, teratogenic or carcinogenic effects.
The drug was well tolerated by patients; no local or general allergic reactions were noted.
The use of Longidase in therapeutic doses during or after surgical treatment does not cause worsening of the postoperative period or progression of the infectious process; does not slow down bone tissue recovery.
Longidaza: how to take
- Injection form. The course of therapy ranges from 5 to 25 injections, each of which is given once every few days, the frequency depends on the prescription of the treating doctor. When using Longidase for prophylactic purposes, the interval between injections is 2 weeks.
Before administration, the powder is dissolved in 1-2 milliliters of procaine or in saline if the anesthetic is intolerant. The drug is administered slowly and immediately after preparation; it cannot be stored.
- Suppositories. They are administered vaginally before bedtime and in a lying position, rectally only after cleansing the intestines. The course of treatment ranges from 10 to 20 suppositories, depending on the pathology. The interval between administrations is from 48 to 72 hours.
LONGIDAZE lyophilized powder for the preparation of solution for infusion 3000me No. 5
Longidaza is applied subcutaneously (near the site of the lesion or under scar tissue) or intramuscularly at a dose of 3000 IU in a course of 5 to 25 injections (depending on the disease) with an interval between injections of 3 to 10 days. Methods of application are selected by the doctor depending on the diagnosis, severity of the disease, clinical course, and age of the patient. If necessary, a repeat course is recommended after 2-3 months. In the case of treatment of diseases accompanied by a severe chronic productive process in the connective tissue, after a standard course, long-term maintenance therapy with Longidaza is recommended with breaks between injections - 10-14 days. To increase the bioavailability of drugs and diagnostic agents, a dose of 1500 IU is recommended with a preliminary 10-15 minutes intramuscular or subcutaneous injection into the same place as the main drug. Dilution The contents of the Longidaza ampoule or bottle are dissolved in 1-2 ml of procaine solution (0.25% or 0.5%). In case of intolerance to procaine, the drug is dissolved in the same volume of 0.9% sodium chloride solution for injection or water for injection. When used to increase bioavailability, the contents of the Longidaza ampoule or vial are dissolved in 2 ml, and with a dose of 1500 IU - in 1 ml of 0.9% sodium chloride solution for injection. The solvent must be introduced into the vial or ampoule slowly, wait for 2-3 minutes, and carefully mix without shaking so as not to foam the protein. The prepared solution for parenteral administration cannot be stored. Do not administer IV! Recommended prevention and treatment regimens For the prevention of adhesive disease and severe scarring after surgical interventions on the abdominal and pelvic organs IM at a dose of 3000 IU 1 time every 3 days for a course of 5 injections. If necessary, the use of the drug can be continued with a general course of up to 10 injections when administered once every 5 days. For treatment in gynecology: adhesions in the pelvis for inflammatory diseases of the internal genital organs - intramuscularly once every 3-5 days for a course of 10-15 injections; tubo-peritoneal infertility - IM with a general course of up to 15 injections: the first 5 injections 1 time in 3 days, then - 1 time in 5 days. in urology: chronic prostatitis - intramuscularly once every 5 days, in a course of 10-15 injections; interstitial cystitis - intramuscularly once every 5 days, for a course of up to 10 injections. in surgery: adhesive disease after surgical interventions on the abdominal organs - intramuscularly once every 3-5 days for a course of 10 to 15 injections; long-term non-healing wounds - intramuscularly once every 5 days with a course of 5-10 injections. in dermatovenereology, cosmetology: limited scleroderma - intramuscularly once every 3-5 days for a course of up to 20 injections. The dose and course are selected individually depending on the clinical course, stage, location of the disease and the individual characteristics of the patient; keloid, hypertrophic and developing scars after pyoderma, burns, operations, injuries - intra-scar or subcutaneous injection near the site of the lesion, administration 1 time every 3 days, for a course of up to 15 injections at a dosage of 3000-4500 IU. The volume of dilution of the drug Longidaza is selected by the doctor depending on the number of points of administration. If necessary, the course can be continued according to the scheme once every 5 days up to 25 injections. Depending on the area of skin damage and the age of scar formation, alternating subcutaneous and intramuscular administration is possible once every 5 days at a dose of 3000 IU, for a course of up to 20 injections. in pulmonology and phthisiology: pneumosclerosis - intramuscularly once every 5 days for a course of 10 injections; fibrosing alveolitis - intramuscularly once every 5 days for a course of 15 injections, then maintenance therapy once every 10 days for a total course of up to 25 injections; tuberculosis - intramuscularly once every 5 days for a course of up to 25 injections; Depending on the clinical picture and severity of the disease, long-term therapy is possible (from 6 months to 1 year at a dose of 3000 IU once every 10 days). in orthopedics: joint contractures - subcutaneously near the site of the lesion at a dose of 3000 IU once every 3 days for a course of 5 to 15 injections; arthrosis, ankylosing spondylitis - subcutaneous injection near the site of the lesion in a dose of 3000 IU once every 3 days for a course of up to 15 injections, if necessary, treatment can be continued with injections once every 5 days. The duration of maintenance therapy is selected by the doctor depending on the severity of the disease; hematomas - subcutaneously near the site of the lesion at a dose of 3000 IU once every 3 days for a course of up to 5 injections. To increase bioavailability: when administered subcutaneously or intramuscularly with diagnostic or medicinal drugs (antibiotics, chemotherapy drugs, anesthetics and others), Longidase is administered 10-15 minutes beforehand at a dose of 1500 IU in the same way and in the same place, as the main drug.
Longidaza
Trade name: Longidaza International name: Hyaluronidase+Azoximer
Country of origin: Russia
Manufacturer: Petrovax Pharm NPO LLC
Release form: suppositories for vaginal or rectal administration 3 thousand IU (contour cell packaging)
Composition: hyaluronidase [as a conjugate with the activated form of azoximer] 3000 IU
Pharmacological group: enzyme agent
Pharmacological group according to ATK: V03AX Other drugs
Pharmacological action: hyaluronidase, improves microcirculation, stimulates tissue repair, increases tissue permeability
Drug registration number: LSR-002940/07
Dates of registration, re-registration: 01.10.2007
RF HS codes: 3004 90 190 9
Shelf life: 2 years.
Pharmacodynamics: Hyaluronidase has enzymatic proteolytic (hyaluronidase) activity of prolonged action, immunomodulatory, chelating, antioxidant and anti-inflammatory effects. An increase in the duration of action of the enzyme is achieved by covalent binding of the enzyme to a physiologically active high-molecular carrier (an activated derivative of poly-1,4-ethylenepiperazine N-oxide), which has its own pharmacological activity: it has an immunomodulatory, detoxifying, antioxidant effect. The covalent bond significantly increases the enzyme's resistance to denaturation and the action of inhibitors: the enzymatic activity of Hyaluronidase is maintained when heated to 37 degrees C for 20 days, while native hyaluronidase loses its activity within 24 hours under the same conditions. The covalent bond ensures the simultaneous local presence of a hydrolytic enzyme and a carrier capable of binding released enzyme inhibitors and stimulators of collagen synthesis (including iron ions, Cu2+, heparin). Thanks to these properties, the drug has not only the ability to depolymerize the connective tissue matrix in fibrogranulomatous formations, but also suppress the reverse regulatory reaction aimed at the synthesis of connective tissue components. The specific substrate of testicular hyaluronidase is glycosaminoglycans (hyaluronic acid, chondroitin, chondroitin-4-sulfate, chondroitin-6-sulfate), which form the basis of the connective tissue matrix. As a result of depolymerization (breaking the bond between C1 acetylglucosamine and C4 glucuronic or induronic acids) under the influence of hyaluronidase, glycosaminoglycans lose their basic properties: viscosity, the ability to bind water, metal ions, the formation of collagen proteins in fibers becomes more difficult, the permeability of tissue barriers increases, and fluid movement is facilitated in the intercellular space, the elasticity of the connective tissue increases, which is manifested in a decrease in tissue swelling, flattening of scars, an increase in the range of motion of joints, a decrease in contractures and prevention of their formation, and a decrease in adhesions. The drug weakens the course of the acute phase of inflammation, regulates (increases or decreases depending on the initial level) the synthesis of inflammatory mediators (interleukin-1 and TNF), increases the body's resistance to infection and the humoral immune response. Does not have antigenic properties, mitogenic, polyclonal activity, does not have allergenic, mutagenic, embryotoxic, teratogenic and carcinogenic effects.
Pharmacokinetics: When administered parenterally, the drug is rapidly absorbed into the systemic circulation and is characterized by a high rate of distribution in the body. TCmax - 20-25 min. The half-life of distribution (alpha phase) is about 0.5 hours, T1/2 (beta phase) for different routes of administration is 42-84 hours. It is excreted mainly by the kidneys. In the body, hyaluronidase undergoes hydrolysis, and the carrier breaks down into low molecular weight compounds (oligomers), which are excreted by the kidneys. Penetrates into all organs and tissues, incl. passes through the BBB and the blood-ophthalmic barrier. Does not accumulate.
Indications: As part of complex therapy for diseases accompanied by connective tissue hyperplasia:
in pulmonology, urology, gynecology with the development of inflammation of the interstitial type: pneumofibrosis, tuberculosis, alveolitis, tuberculoma, chronic interstitial cystitis, adhesions in the pelvis, tubo-peritoneal infertility,
in orthopedics, surgery, cosmetology: keloid, hypertrophic, retracted scars after pyoderma, trauma, burns, operations, long-term non-healing wounds, joint contractures, arthritis, hematomas, adhesive disease,
in dermatovenerology: limited scleroderma of various localizations,
To increase the bioavailability of drugs and diagnostic drugs.
Dosage regimen: SC or IV (near the site of the lesion or under scar tissue) or IM at a dose of 3000 IU in a course of 5 to 15 injections (depending on the severity of the disease) with an interval between injections of 3 to 10 days. If necessary, a repeat course is recommended after 2-3 months.
Methods of application are selected individually depending on the diagnosis, clinical course and severity of the disease, and the age of the patient.
In the case of treatment of diseases accompanied by a severe chronic productive process in the connective tissue, after the standard course, long-term maintenance therapy is recommended at a dose of 3000 IU with breaks between administrations of 10-14 days.
For respiratory diseases - intramuscularly, 3000 IU once every 3-5 days for a total course of 10 injections. Further long-term therapy is possible (from 3-4 months to 1 year at a dose of 3000 IU once every 10-14 days).
For diseases of the pelvic organs, IM 1 time every 3-5 days at a dose of 3000 IU for a total course of 5 to 15 injections.
For limited scleroderma of various shapes and localization - intramuscularly 1 time every 3 days at a dose of 3000-4500 IU in a course of 5-15 injections.
Keloid, hypertrophic, retracted scars after pyoderma, burns, operations - intrascar administration at a dose of 3000 IU in 1-2 ml 1-2 times a week for a course of 5-10 injections, and/or intramuscular administration 1 time every 3-5 days a total course of up to 10 injections.
Long-term non-healing wounds - IM at a dose of 1500-3000 IU once every 5 days for a course of 5-7 injections.
Joint contractures, arthritis, hematomas - IM at a dose of 3000 IU 1-2 times a week for a course of 7 to 15 injections.
Adhesive disease - intramuscularly once every 3-5 days at a dose of 3000 IU, with a total course of 7 to 15 injections.
To increase the bioavailability of drugs and diagnostic drugs (antibiotics, chemotherapy drugs, local anesthetics) - intramuscularly once every 3 days at a dose of 1500 IU. A course of no more than 10 injections.
For chronic renal failure, it is prescribed no more than once a week.
The contents of the ampoule are dissolved in 1.5-2 ml of 0.25% or 0.5% procaine solution or (in case of procaine intolerance) in 0.9% NaCl solution or water for injection. For electrophoresis, the solution is prepared with distilled water, for inhalation - with a 0.9% NaCl solution.
Side effects: Pain at the injection site, allergic reactions, local reactions (skin hyperemia, tissue swelling at the injection site).
Contraindications: Hypersensitivity, malignant neoplasms, pregnancy, children under 12 years of age (efficacy and safety have not been established).
Interaction: Possible combination with antibiotics, antiviral, antifungal and antihistamines, corticosteroids, bronchodilators, cytostatics.
Increases the bioavailability of drugs, accelerates the onset of analgesia when administering local anesthetics.
Special instructions: It should not be injected into an area of infectious process, acute inflammation, or tumor.
Carefully. Acute renal failure, pulmonary hemorrhage.
Storage conditions: List B. The drug should be stored in a dry place, protected from light, out of reach of children, at a temperature not exceeding 15°C.
Dispensed from pharmacies: The drug is available with a prescription.