Iron deficiency anemia IDA is a hypochromic microcytic anemia that develops as a result of an absolute deficiency of iron in the body.
In addition to anemic syndrome, it is characterized by dysfunction of the skin, its appendages and mucous membranes - sideropenic syndrome.
IDA is the last stage of iron deficiency; Before the onset of anemia, often with detailed questioning and examination of the patient, manifestations of sideropenia can be detected, which will allow timely identification of the cause of iron deficiency and prevent the development of IDA.
Types of iron-containing drugs
Pharmacological companies offer a wide range of medicines and dietary supplements containing iron. The first group is prescribed for treatment, since the medications have a higher dosage of the main active ingredients. Supplements are used to prevent iron deficiency and maintain it within normal limits.
Main types:
- Iron tablets. Medicines contain ferrous iron in the form of ferrous gluconate or ferrous sulfate. The second substance has a little more iron, but the difference is smoothed out by selecting the dosage. The effectiveness of both substances is approximately the same. Iron tablets should not be prescribed to yourself, as they are used to treat confirmed anemia. Medicines have side effects and contraindications, but they are fast-acting and easy to digest. If you take the tablets for 14-28 days, you can significantly improve your hemoglobin level.
- Iron in vitamin complexes. Multivitamins can help with mild anemia, but are not suitable for treating severe conditions. In pharmacies you can buy complex preparations with ferric iron. The substance is less digestible, but easier to tolerate. To achieve an effect, the duration of use should be from two to three months. The effect of taking iron as part of vitamin complexes is enhanced by the presence of other minerals and vitamins - ascorbic and folic acids, vitamin B12, copper, manganese.
- Biologically active additives. Vitamins can also be classified as dietary supplements. However, dietary supplements with iron may contain extracts of medicinal herbs, as well as vitamin compounds. To increase vitality, supplements may contain eleutherococcus or ginseng extract. A permanent or course treatment is indicated.
Clinical pharmacology of modern iron preparations and their place in the treatment of iron deficiency anemia
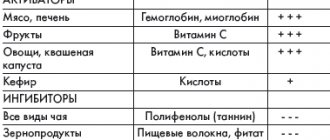
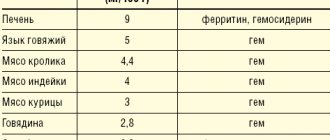
Latent iron deficiency in the population of Europe and Russia is 30–40%, and in some regions (North, Northern Caucasus, Eastern Siberia) – 50–60% [2,3]. Iron deficiency anemia is a hypochromic microcytic anemia that occurs as a result of a decrease in iron content in the body and is an independent nosological form (code D-50 according to ICD-10). Latent iron deficiency is considered a functional disorder, does not have an independent code and is usually coded in the section “Insufficiency of other nutrients” (E61). Chronic IDA is a consequence of a long-term negative iron balance in the body. The reasons for its development may be chronic blood loss due to gastrointestinal bleeding (erosive gastritis, peptic ulcer, hemorrhoids, taking acetylsalicylic acid, indomethacin), uterine bleeding during heavy menstruation, as well as tumors (rectal and colon cancer, bladder cancer), donation, increased need for iron during pregnancy and lactation, in adolescence (juvenile chlorosis), with parasitic diseases (diphyllobothriasis), insufficient iron intake (gastroduodenitis, colitis, gastrectomy), nutritional iron deficiency in vegetarians [2,4]. Pathogenesis. The total amount of iron in the body is 4–4.5 g. Iron is involved in the functioning of all biological systems, being an obligatory and indispensable component of various proteins and enzymes that provide the necessary level of systemic and cellular aerobic metabolism, as well as redox homeostasis in the body as a whole . Iron plays an important role in maintaining a high level of immune resistance; its adequate content in the body contributes to the full functioning of nonspecific defense factors, cellular and local immunity. Normal iron content is necessary for complete phagocytosis, synthesis of lysozyme, interferon, ensures high activity of natural killer cells and the bactericidal ability of serum [5,6]. The daily requirement for iron is 10 mg for men, 18 mg for women (during pregnancy – 38 mg, lactation – 33 mg) [6]. The need for iron is also increased in active donors. In children and adolescents, due to the increased needs of the growing body and insufficient intake of iron from food, the iron balance is often disturbed [7]. The main source of iron for humans is food products of animal origin, which contain iron in the most digestible form (as heme). The absorption of iron from foods decreases after heat treatment, freezing, and long-term storage. Iron, entering the body with food, is absorbed in the intestine (most intensively in the duodenum and the initial part of the jejunum). Iron absorption depends on the nature of the food, the calorie content of the diet and the absorption capacity of the small intestine. Iron in heme is absorbed much better. People who eat meat get more heme iron (in myoglobin) than vegetarians. Strict vegetarians may develop iron deficiency over time because vegetables and grains contain substances that interfere with iron absorption, particularly phosphates [7,8]. Fructose, hydrochloric, ascorbic, succinic, pyruvic acids, cysteine, sorbitol and alcohol enhance iron resorption. Ferrous inorganic iron is absorbed much better than oxide iron contained in meat products [9]. From the gastrointestinal tract (GIT), iron is absorbed only in the divalent state, the conversion to which is ensured by organic acids, in particular ascorbic acid. The main share of absorbed iron in the transport protein, transferrin, is transferred to the bone marrow, where it is used for the synthesis of heme-containing compounds (hemoglobin, myoglobin, enzymes), non-heme enzymes (for example, NADH dehydrogenase), and metalloproteins. In tissues, iron is deposited in the form of ferritin and hemosiderin, with predominant deposition in the liver, spleen and muscles. Iron deficiency in the body develops when iron losses exceed 2 mg/day. [9]. However, not every iron deficiency is accompanied by anemia; prelatent and latent iron deficiency are also distinguished [2,5]. Prelatent deficiency develops when the intake of iron from food does not meet physiological needs (body growth, menstruation, pregnancy), but the insufficient intake of iron is covered by its reserves. At the same time, iron reserves are depleted. Latent deficiency is the next stage at which the supply of iron to the cells of the erythroid germ is reduced and the production of red blood cells is limited. IDA with hypochromia and microcytosis develops as a result of a long-term negative iron balance, when hemoglobin synthesis decreases. Most often, anemic syndrome associated with the development of IDA occurs in the practice of a general practitioner, general practitioner (family doctor), hematologist, obstetrician-gynecologist. According to currently accepted standards of higher professional and postgraduate professional education, these specialists are competent to suspect IDA syndrome based on the clinical picture and peripheral blood picture, develop a program of diagnostic and therapeutic measures, justify a program of preventive measures in patients with IDA, taking into account the presence of factors the risk of relapse. The clinical picture of IDA depends on the stage of iron deficiency. Stages of iron deficiency (ID): • pre-latent iron – characterized by a decrease in iron reserves, but without a decrease in the amount spent on erythropoiesis (reserve iron deficiency); • latent iron deficiency – characterized by complete depletion of iron stores in the depot, a decrease in the level of ferritin in the blood serum, an increase in the total iron-binding capacity of the serum (TIBC) and the level of transferrin, but still without signs of the development of anemia (transport iron deficiency); • IDA is the final stage of iron deficiency, which occurs when the hemoglobin pool of iron decreases and is manifested by symptoms of anemia and hyposiderosis (obvious iron deficiency). There is a classic clinical symptomatology of IDA in the body, consisting of general symptoms of anemia caused by hemic hypoxia, as well as signs of tissue iron deficiency (sideropenic syndrome) (Table 1). Anemia that develops during pregnancy has an adverse effect on the intrauterine state of the fetus, contributing to the occurrence of fetal growth retardation syndrome and complications of the early neonatal period. In children during the newborn period, there is a large loss of body weight and a slower recovery, delayed loss of the umbilical cord remnant and delayed epithelization of the umbilical cord wound, and a long course of physiological jaundice [10,11]. Diagnostics. To diagnose iron deficiency in the body, indicators characterizing various funds of iron metabolism are determined: transport, functional, reserve and iron regulatory (Table 2). Laboratory signs that allow one to suspect and verify IDA are a low color index, a decrease in the MSI index (below 27 pg, normally 27–35 pg), hypochromia and microcytosis of erythrocytes, a decrease in serum iron levels, an increase in the TI value, a decrease in serum ferritin levels . Differential diagnosis for IDA is also carried out with anemia in chronic diseases, megaloblastic anemia associated with deficiency of vitamin B12 or folic acid, hemolytic and aplastic anemia (possible, among other things, due to the toxic effects of various classes of drugs, occupational hazards, such as lead, benzene) [ 12]. The differential diagnosis of IDA and anemia in chronic diseases is presented in Table 3. The most common causes of anemia in chronic diseases are chronic infections (diseases of the respiratory system, urinary tract, osteomyelitis), chronic non-infectious diseases (diffuse connective tissue diseases, rheumatic fever), malignant tumors ( cancer, lymphogranulomatosis, non-Hodgkin's lymphoma, leukemia). The hypochromic nature of anemia makes it very likely that it is iron deficiency (all IDA are hypochromic). However, the hypochromic nature of anemia does not exclude other pathogenetic variants of anemia (not all hypochromic anemias are iron deficiency). In this regard, differential diagnosis of IDA with other, less common hypochromic anemias (sideroachrestic anemia, thalassemia) is necessary. Determination of serum iron levels makes it possible to distinguish between these conditions at the stage of diagnostic search. Serum iron levels can be influenced by a number of factors: taking iron medications (vitamin preparations containing small amounts of iron, certain medications (oral contraceptives, allopurinol)), red blood cell transfusions, time of serum iron testing, thereby masking the true iron content in the serum , which should be taken into account when interpreting the results obtained. Treatment. In accordance with the etiological and pathogenetic factors of IDA, treatment should be comprehensive, aimed at eliminating the cause that caused the disease, and include adequate intake of microelements, vitamins, proteins and correction of iron deficiency. Iron is absorbed most effectively from foods in which it is contained in the form of heme, when it is actively captured and absorbed by the cells of the intestinal mucosa in unchanged form (beef tongue, rabbit, turkey, chicken, beef). The processes of heme absorption in the intestine do not depend on the acidity of the environment and inhibitory nutrients. As already mentioned, in cereals, fruits and vegetables, iron is in non-heme form, and absorption from them is much worse. The presence of oxalates, phosphates, tannin and other ferroabsorption inhibitors also contributes to a decrease in absorption (Table 4). It should be borne in mind that a complete and balanced diet in terms of the main ingredients allows only to “cover” the physiological need of the body for iron, but does not eliminate its deficiency, and should be considered as one of the auxiliary components of therapy. Currently, the indications for parenteral use of iron preparations have been narrowed: they are used in the presence of intestinal pathology with malabsorption (various enteritis, malabsorption syndrome, resection of the small intestine, Billroth II gastric resection with the formation of a “blind loop”). Parenteral iron supplements may be the treatment of choice if oral iron supplements are poorly tolerated. Currently, in the treatment of IDA, the oral use of combination drugs (containing both iron salts and other components), the leading of which is Ferro-Folgamma, seems promising. Ferro-Folgamma (Wörwag Pharma, Germany) is a multifactorial hematopoietic that includes all the necessary components (1 capsule contains 112.6 mg of iron sulfate (equivalent to 37 mg of iron ion), 5 mg of folic acid, 0.010 mg of cyanocobalamin), providing stimulation of the structural synthesis of Hb and increasing the reproduction of red blood cells by the red sprout of the bone marrow. The drug also contains ascorbic acid. The versatility of the drug is associated with its selective stimulating effect on the synthesis of the iron-containing and protein parts of hemoglobin. Ferrous sulfate has a high absorption rate in the gastrointestinal tract and practically does not form inaccessible complex compounds in it. The absorption coefficient is significantly enhanced by the presence of ascorbic acid in the preparation [12]. Sulfate replenishes iron deficiency in the body. Iron is part of hemoglobin, myoglobin and a number of enzymes. Being a structural component of heme, it takes part in erythropoiesis. Ascorbic acid helps improve the absorption of iron in the intestines. Cyanocobalamin (vitamin B12) and folic acid are involved in the formation and maturation of red blood cells. The active components of the Ferro-Folgamma drug are in a special neutral shell, which ensures their absorption, mainly from the upper part of the small intestine. The absence of local irritation on the gastric mucosa contributes to good tolerability of the drug in the gastrointestinal tract. Ferro-Folgamma is prescribed 1 capsule 3 times a day. The best effect is obtained by using the drug after meals. For mild anemia, it is recommended to take 1 capsule 3 times a day. within 3–4 weeks; for moderate forms – 1 capsule 3 times a day. within 8–12 weeks; in severe cases - 1 capsule 3 times a day. within 16 weeks. and more. The good clinical effect of the drug is confirmed by data from numerous clinical studies. Thus, in the studies of A.L. Vertkina et al. [14] have proven the high effectiveness of the drug Ferro-Folgamma (compared to other ferrodrugs) in the treatment of IDA. The authors observed 83 people (22 men and 61 women) aged from 17 to 92 years (average age – 57.7±1.4 years). In the group, the average hemoglobin level was reduced to 87.8±0.4 g/l, the average duration of anemia was 1.5±0.1 years. The causes of anemia were: acute or chronic blood loss - in 54.3% of cases, malabsorption - in 28.3%, other or combined causes - in 17.3% of cases. When using the drug Ferro-Folgamma, more pronounced positive dynamics of both clinical and laboratory parameters were observed compared with other ferrocontaining drugs [14] (Tables 5 and 6). The use of Ferro-Folgamma in the correction of IDA in chronic heart failure (CHF) has also been proven to be highly effective [15]. The authors selected for examination and treatment 42 patients with CHF combined with IDA (in the whole group Hb = 97.1 ± 3.7 g/l; serum Fe = 5.84 ± 0.51 mmol/l): in II FC HF – Hb = 102.3±3.6 g/l, with FC III HF – Hb = 97.6±3.3 g/l, with FC IV HF – Hb = 84.4±3.5 g/ l. During the treatment of CHF (ACE inhibitors, cardiac glycosides, diuretics), relief of anemic syndrome was carried out by prescribing Ferro-Folgamma (a complex of 100 mg of anhydrous Fe sulfate with 5 mg of folic acid, 10 μg of cyanocobalamin and 100 mg of ascorbic acid) in the total dose for the whole group –137.75±7.5 mg Fe. By the end of treatment (23.7±3 days), the hemoglobin level in general in the group of patients with CHF increased by 9.8%, serum Fe increased by 95.5%, exercise tolerance increased by 47.6%, ejection fraction ( EF) increased by 32.2%, stroke volume (SV) increased by 51.7%; Before treatment, 31 patients with CHF with IDA (73.8%) had HF class III–IV; after treatment, 23 patients (54.8%) switched to HF class I; 19 patients (45.2%) had class II HF. FC SN. Thus, all of the above suggests that correction of even a mild degree of anemia in patients with CHF can lead to a significant improvement in the pumping function of the heart and a decrease in the functional class of HF (NYHA). The use of Ferro-Folgamma in the treatment of anemia in pregnant women has also been proven to be highly effective. So, under the leadership of Professor V.A. Burlev and academician of the Russian Academy of Medical Sciences, professor V.N. Serov at the Federal State Institution “Scientific Center of Obstetrics, Gynecology and Perinatology named after. Academician V.I. Kulakov" conducted a number of studies on the problem of iron deficiency in pregnant women, postpartum women and gynecological patients [16–19]. The clinical effectiveness of the drug Ferro-Folgamma has been most fully studied, which has been successfully used for the treatment of latent iron deficiency (LDI) and manifest iron deficiency (MID) in obstetric and gynecological patients, both alone and in combination with recombinant erythropoietin preparations. The results obtained showed that the unique ratio between the optimal content of ferrous iron, folic acid and cyanocobalamin in one Ferro-Folgamma capsule allows one to achieve excellent results in the treatment of pregnant women, postpartum women and gynecological patients with not only mild, but also moderate and severe MID. The presence of folic acid and cyanocobalamin in the Ferro-Folgamma preparation is its additional advantage, since with MID in pregnant women there is often a deficiency of many vitamins, especially those involved in hematopoiesis. According to the data obtained, if there are indications for the use of recombinant erythropoietin, the optimal oral iron preparation for the combined treatment of MAD in women outside and during pregnancy, as well as after childbirth, is currently Ferro-Folgamma. The use of Ferro-Folgamma in pregnant women with anemia and when it is combined with gestosis leads to an improvement in the clinical condition, a significant increase in hematological (hemoglobin - by 15%, erythrocytes - by 10%, hematocrit - by 9%) and ferrokinetic parameters (serum iron - by 32%, ferritin – by 53%), folic acid level – by 24% and vitamin B12 – by 21.7% [18,19]. The effectiveness of using Ferro-Folgamma in the treatment of anemia in pregnant women was also proven in a study by V.A. Petrukhin and V.L. Grishin [19]. According to researchers, the use of Ferro-Folgamma 1 capsule 2 times a day. within 6 weeks. led to the normalization of clinical and laboratory indicators in all observed patients with the SDA syndrome developed during pregnancy [20]. Thus, in the treatment of UDA and latent iron deficiency, it is optimal to use the drug Ferro -folgamma, which allows you to achieve good and quick results. The presence of folic acid and vitamin B12 in the drug is its additional advantage, since in iron deficiency conditions there is often a deficiency of these vitamins. The presence of ascorbic acid improves the absorption and absorption of iron. The microcapsulated form of the drug excludes local irritation of the stomach and intestines. Scientific and practical experience convinces us of the appropriateness and high efficiency of use in therapeutic, hematological, obstetric and gynecological practice in the treatment of iron deficiency states of ferro -pholgamma as a drug with proven efficiency and non -punishment, which has the optimal ratio of cost and efficiency.
References 1. WHO. Official annual report. Geneva, 2002. 2. Zakharova N.O., Nikitin O.L. Iron deficiency anemia in elderly and senile patients: a scientific and practical guide for doctors. Samara, 2008. 60 p. 3. Gorodetsky V.V., Godulyan O.V. Iron deficiency conditions and iron deficiency anemia: treatment and diagnosis. M.: Medpraktika-M, 2004. pp. 1–28. 4. Dvoretsky L.I. Treatment of iron deficiency anemia // Russian Medical Journal. 2006. T. 6. No. 20. P. 1312–1316. 5. Kryukov N.N., Kachkovsky M.A., Verbovoy A.F., Babanov S.A. Therapist's handbook. Diagnostic reference book. M.: Astrel, 2012. 672 p. 6. Hillman R. Iron deficiency and other hyporegenerative anemias. Internal medicine according to Tinsley R. Harrisson // Difficult Patient. 2005. No. 2. P. 770. 7. Shekhtman M.M. Iron deficiency anemia and pregnancy // Ginekol. 2000. T. 2. No. 6. P. 164–171. 8. Serov V.N., Shapovalenko S.A., Flaks G.A. Diagnosis and treatment of iron deficiency in women at different periods of life // Atmosphere. Cardiology. 2008. No. 2. pp. 17–20. 9. Kosarev V.V., Babanov S.A., Verbovoy A.F. Handbook of clinical pharmacologist. Rostov-on-Don: Phoenix, 2011. 476 p. 10. Podzolkova N.M., Nesterova A.A., Nazarova S.V., Sheveleva T.V. Iron deficiency anemia in pregnant women // Russian Medical Journal. 2003. No. 11 (5). pp. 326–32. 11. Smirnova O.V., Chesnokova N.P., Mikhailov A.V. Iron deficiency anemia in pregnant women. Etiology and pathogenesis of metabolic and functional disorders. Saratov, 1994. 12. Kosarev V.V., Babanov S.A. Clinical pharmacology and rational pharmacotherapy. M.: Infra-M, 2012. 236 p. 13. Dvoretsky L.I., Zaspa E.A., Litvitsky P.F., Bolevich S.B., Menshova N.I. Free radical processes in patients with iron deficiency anemia during treatment with iron supplements // Therapeutic archive. 2006. No. 78 (1). pp. 52–57. 14. Vertkin A.L., Godulyan O.V., Gorodetsky V.V., Skotnikov A.S. Iron deficiency anemia and the choice of drug for its correction // Russian Medical Journal. 2010. No. 5. 15. Shilov A.M., Melnik M.V., Retivykh O.N., Kim I.R. Correction of iron deficiency anemia in chronic heart failure // Russian Medical Journal. 2005. No. 19. pp. 1254–1257. 16. Burlev, V.A., Konovodova E.N., Ordzhonikidze N.V., Serov V.N., Elokhina T.B., Ilyasova N.A. Treatment of latent iron deficiency and iron deficiency anemia in pregnant women // Russian Bulletin of Obstetrician-Gynecologist. 2006. No. 1. P. 64–68. 17. Konovodova E.N., Burlev V.A. Ferro-Folgamma + Erythropoietin - new possibilities for the treatment of anemia in patients with uterine fibroids // Farmateka. 2004. No. 15 (92). pp. 70–73. 18. Konovodova E.N., Burlev V.A., Kravchenko N.F., Karibdzhanov O.K., Murashko L.E., Sopoeva Zh.A. Transferrin saturation coefficient with iron in pregnant women // Problems of reproduction. 2002. No. 6. P. 45–47. 19. Murashko L.E., Konovodova E.N., Burlev V.A., Sopoeva Zh.A. Volumetric oxygen transport in pregnant women with anemia and gestosis during treatment with Ferro-Folgamma // Russian Medical Journal. 2002. T. 10. No. 7. pp. 364–367. 20. Petrukhin V.A., Grishin V.L. Treatment of anemia in pregnant women using the drug ferro-foil // Problems of reproduction. 2002. No. 6.
In what forms are iron supplements available?
For ease of use by both adults and children, manufacturers produce medications in different forms.
For oral administration we offer:
- pills. The main active ingredients are gradually released in the stomach, the tablets do not irritate the mucous membrane. Pros: the effect is independent of food intake, you can take it with you, it’s convenient to take. The downside is that iron from tablets has lower absorption compared to other forms. It is better to find out from your doctor which iron tablets are best to choose;
- syrups. Suitable for babies and older children. The viscous consistency promotes envelopment of the stomach walls and rapid and complete absorption. Disadvantages - they may have an unpleasant taste, and with a high iron content they can stain teeth. Contains sugar and is not suitable for people with diabetes;
- capsules. They are convenient for adults to take, but dissolution in the stomach can cause discomfort. The capsule is indivisible and is not suitable for use by small children.
- hematogen. Can be used by children and adults, has a pleasant taste and is well absorbed. Abuse must be avoided and age-specific dosages must be observed.
Iron is also available in the form of chewable tablets, drops, and powders for preparing solutions.
In a hospital setting, treatment can be carried out by injection into a vein, into a muscle, or using systems using iron-containing solutions. The choice in favor of parenteral administration is made in situations that threaten the patient’s life, as well as when it is impossible or ineffective to use drugs for oral administration.
Review of drugs for anemia
Pharmacies offer a wide range of medicines that increase hemoglobin. The most frequently prescribed by doctors are:
- Fenyuls in capsules. Indicated for regular blood loss, to replenish iron deficiency. Contains B vitamins and ascorbic acid. You can buy capsules inexpensively in the online store. The price for a pack of 30 pieces starts from 250 rubles;
- Ferrum-Lek in the form of chewable tablets, syrup, solution for intramuscular administration. Intended for the treatment of hidden iron deficiency, the treatment of anemia, and is suitable for preventing the development of anemia in pregnant women. The syrup is allowed for small children. You can reserve medications on the store’s website. Information about prices, promotions, discounts and available drugs is also available there;
- Maltofer in drops, tablets, syrup, solution for intramuscular administration. In the form of drops, it is used to treat anemia in newborns and premature babies. Tablets are allowed from 12 years of age;
- Ferretab capsules. They have a prolonged effect and contain folic acid. Suitable for pregnant women. One capsule per day is enough. The cost of 30 pieces starts from 380 rubles. You can quickly order and pay for your purchase directly on the website at a time convenient for you.
- Sorbifer Durules tablets. It is prescribed for anemia and iron deficiency, and is also indicated for preventive purposes for pregnant, lactating women and donors. Can be used in children from 12 years of age. For prevention, one tablet per day is enough. Additionally contains ascorbic acid.
The choice of an iron-containing drug should be entrusted to a doctor, who will prescribe a blood test and, based on the results, choose the appropriate medication.
Stages of iron deficiency
Currently, there are several stages of iron deficiency:
1. Predisposition to the development of iron deficiency (vegetarianism, adolescence in combination with menstrual irregularities in girls, frequent childbirth, the presence of chronic diseases of the gastrointestinal tract or female reproductive system associated with blood loss).
2. Pre-latent iron deficiency. At this stage there are no laboratory criteria for iron deficiency, however, an increase in the absorption of 59Fe3+ in the gastrointestinal tract can be determined, which can exceed 50% (normally 10-15%).
3. Latent iron deficiency. It is characterized by the development of sideropenic syndrome, a decrease in iron reserves in the body according to laboratory tests.
4. WAITING. The diagnosis is established when the hemoglobin concentration decreases to less than 120 g/l in women and 130 g/l in men.