Translation of materials from the Muscular Dystrophy UK website
A link to the original, as well as a saved pdf file with the original article, can be found at the end.
Duchenne muscular dystrophy
Penny Southall, Dan Hanson's mom
“My son Dan was diagnosed with Duchenne muscular dystrophy at the age of three. I know from experience what a crushing blow such a diagnosis can be. “Just like us, you must be trying to figure out how you can even come to terms with this. We found our way to cope, and you can too. I told myself that he was still the same person, but I saw him from a different side. This thought helped me move forward. If he feels good, then I will feel good too. “When I learned of Dan’s diagnosis, the first thing I did was look for research into what life is like for people with Duchenne muscular dystrophy. I learned that he can live as full and happy a life as anyone else. At that moment, this became a great consolation for me, and years later, I was already convinced of this. “Dan has close friends, is a good student, plays sports and is confident about his future. Nowadays, so much help and support is provided to people with disabilities. They can try themselves in sports and get the necessary education. “I asked my son, now 15, what he would like to say to families who received news of this diagnosis. He replied, “It seems terrible at first, but it will get better.”
What is Duchenne muscular dystrophy?
Duchenne muscular dystrophy is a muscle wasting caused by a deficiency of a protein called dystrophin . Usually only boys are affected by this disease. Around 100 boys with Duchenne muscular dystrophy are born in the UK each year, and there are currently 2,500 boys and young people with Duchenne muscular dystrophy in the UK. There is a risk that out of 3500-5000 male babies, one will have Duchenne muscular dystrophy.
Duchenne muscular dystrophy is a serious disease that causes progressive muscle weakening. Due to a lack of dystrophin, muscle fibers weaken and give way to fibrous or fatty tissue, causing gradual muscle breakdown.
Prof. Dr. Jörg Müller
Neurology – Parkinson's, MS
Head of the Department of Neurology
Specialization
- Recognized international expert in Parkinson's disease, dystonia and tremor
- Neuromuscular diseases
- Multiple sclerosis
- Treatment using butolotoxin (dystonia, spasticity)
- Deep brain stimulation treatment
- Author of more than 70 scientific publications, is a member of international expert councils
Show doctor's personal profile
What are the causes of Duchenne muscular dystrophy?
Duchenne muscular dystrophy is a genetic disorder caused by an abnormality or mutation in the genetic code (DNA). In Duchenne muscular dystrophy, the mutation occurs in a gene called dystrophin , which is located on the X chromosome or sex chromosome (girls have two X chromosomes, boys only one). In half of cases, the disease is transmitted from the mother who is the “carrier,” but it can also result from a new mutation in the child’s genes.
If a mutation occurs in a woman’s body, she is called a “carrier.” Female carriers are usually not affected by this disease because they have a second X chromosome where dystrophin can be produced. A small number of women have some degree of muscle weakness and are called "clear carriers".
Each son of a carrier has a 50% risk of developing the disease, and each daughter has a 50% risk of being a carrier.
Genetic counseling and screening of other family members for risk of being carriers should occur as soon as possible once a boy is diagnosed with Duchenne muscular dystrophy. You can contact your consultant doctor or family doctor.
Prof. Dr. Bettina Schmitz
Neurology – Epilepsy
Head of the Department of Neurology
Specialization
- Epilepsy
- Differential diagnosis of non-epileptic paroxysms
- Long-term EEG - video monitoring
- Medical and non-medical care for paroxysms and complications associated with epilepsy
- Member of the British Medical Association
- Instructor and member of the European Academy for the Study of Epilepsy (EUREPA)
- Member of the Commission on Psychobiology and the International League Against Epilepsy (ILAE)
- Psychoorganic syndrome, World Federation of Societies of Biological Psychiatry (WFSBP)
- Video consultation
Show doctor's personal profile
How is Duchenne muscular dystrophy recognized?
Most boys with Duchenne muscular dystrophy are not diagnosed with Duchenne muscular dystrophy until symptoms appear, unless there is a family member with the condition. The first signs of Duchenne muscular dystrophy usually appear between the ages of one and three years and are usually associated with impaired muscle function. Boys may start walking later than their peers, fall more often, or have difficulty running, jumping, or climbing. They may have enlarged calf muscles.
Some boys with Duchenne muscular dystrophy have slow speech, which may be the first sign of the disease. A blood test reveals high levels of a protein called creatine kinase (CK). KK usually appears in the muscles, but when they are damaged, as is the case with Duchenne muscular dystrophy, it enters the blood. Liver enzymes (aminotransferases, ALT and AST) are also often high as a consequence of muscle damage rather than liver problems.
Duchenne muscular dystrophy must be confirmed by a genetic blood test . Different types of genetic tests provide specific and detailed information about DNA mutations.
Genetic confirmation of the disease is critical. This allows families to conduct prenatal diagnosis in future pregnancies, as well as screen other family members in case they carry a mutation in the dystrophin gene. Moreover, genetic testing will help determine whether a boy is eligible to participate in a clinical trial that is starting or planned.
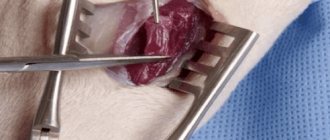
Your doctor may also recommend a muscle biopsy , where a small sample of muscle is removed for analysis. Such studies can provide information about how much dystrophin protein is present in muscle cells, and in some cases help distinguish Duchenne muscular dystrophy from a milder form of the disease known as Becker muscular dystrophy. However, clinical signs and genetic analysis are usually sufficient to distinguish the two forms, without the need for a muscle biopsy.
Literature
- van Putten M., Hulsker M., Nadarajah VD, van Heiningen SH, van Huizen E., van Iterson M. et al. (2012). The effects of low levels of dystrophin on mouse muscle function and pathology. PLoS One. 7 , e31937;
- Russo FB, Cugola FR, Fernandes IR, Pignatari GC, Beltrão-Braga PC (2015). Induced pluripotent stem cells for modeling neurological disorders. World J. Transplant. 5, 209–221;
- Falzarano M. S., Scotton C., Passarelli C., Ferlini A. (2015). Duchenne muscular dystrophy: from diagnosis to therapy. Molecules. 20, 18168–18184;
- Bushby K., Finkel R., Birnkrant DJ, Case LE, Clemens PR, Cripe L. et al. (2010). Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and psychosocial management. Lancet Neurol. 9, 77–93;
- Bushby K., Finkel R., Birnkrant DJ, Case LE, Clemens PR, Cripe L. et al. (2010). Diagnosis and management of Duchenne muscular dystrophy, part 2: implementation of multidisciplinary care. Lancet Neurol. 9, 177–189;
- Long C., Amoasii L., Mireault A.A., McAnally J.R., Li H., Sanchez-Ortiz E. et al. (2016). Postnatal genome editing partially restores dystrophin expression in a mouse model of muscular dystrophy. Science. 351, 400–403;
- Nelson CE, Hakim CH, Ousterout DG, Thakore PI, Moreb EA, Castellanos Rivera RM et al. (2016). In vivo genome editing improves muscle function in a mouse model of Duchenne muscular dystrophy. Science. 351, 403–407;
- Tabebordbar M, Zhu K, Cheng JK, Chew WL, Widrick JJ, Yan WX et al. (2016). In vivo gene editing in dystrophic mouse muscle and muscle stem cells. Science. 351, 407–411;
- Elements: “The prokaryotic immune system will help edit the genome”;
- Gallagher J. (2016). Scientists get 'gene editing' go-ahead. BBC News;
- CRISPR systems: immunization of prokaryotes;
- Mutagenic chain reaction: genome editing on the verge of science fiction;
- Shouldn't we try to… change the genome?;
- Nobel Prize in Physiology or Medicine (2012): induced stem cells;
- Alzheimer's disease: the gene I'm crazy about;
- How to save Thirteen? (Prospects for the treatment of Huntington's disease);
- McGreevy JW, Hakim CH, McIntosh MA, Duan D. (2015). Animal models of Duchenne muscular dystrophy: from basic mechanisms to gene therapy. Dis. Model. Mech. 8, 195–213;
- Singh S. M., Kongari N., Cabello-Villegas J., Mallela K. M. (2010). Missense mutations in dystrophin that trigger muscular dystrophy decrease protein stability and lead to cross-β aggregates. Proc. Natl. Acad. Sci. USA. 107, 15069–15074;
- Goyenvalle A., Seto J. T., Davies K. E., Chamberlain J. (2011). Therapeutic approaches to muscular dystrophy. Hum. Mol. Genet. 20 , R69–R78.
Is there a treatment or cure?
No cure has yet been discovered for this disease, but there is encouraging research in this area. A multi-professional approach, including physical therapists and occupational therapists (specialists who help people with disabilities adjust to life), is the best way to manage Duchenne muscular dystrophy.
Having access to specialists from a variety of disciplines is vital to providing a person with Duchenne muscular dystrophy with all the comprehensive support they need. This means that the patient should have the opportunity to consult with specialists in different fields during one visit to a specialized center: receive advice on the respiratory system, cardiovascular system and physiotherapy. By working together, these professionals will provide more effective care.
It is important to have regular check-ups with specialists in order to make decisions about new treatments at the most appropriate time, and perhaps anticipate and prevent problems. It is recommended that you see your primary care physician every six months and your physical therapist every three to four months.
The physiotherapist will make recommendations regarding interventions (such as flexibility exercises) that may be needed. It is important to allow your son to be as active as possible, with your physiotherapist helping you.
Steroids ( prednisone or deflazacort ) are often prescribed for Duchenne muscular dystrophy because they temporarily slow down the process of muscle weakening and loss of mobility and prevent or delay the development of complications. However, there are many possible side effects that need to be carefully monitored.
Other drugs for Duchenne muscular dystrophy have begun to emerge, including Translarna (ataluren), which is now available in some European countries and can slow the progression of symptoms in boys with Duchenne muscular dystrophy. Translarna only affects a small group of boys who carry a specific mutation in the dystrophin gene (a "nonsense" mutation , where a point mutation in the DNA sequence results in a stop codon). Your doctor will tell you whether this medicine will be effective for your son. Other treatments for specific mutations may soon be approved.
Intensive research into possible treatments for Duchenne muscular dystrophy continues. Some drugs are currently undergoing clinical trials.
It is helpful to have a copy of the genetic report (showing the type and location of the dystrophin gene mutation found in your child). This will help determine which medicine or trial is best for your child.
The Duchenne Muscular Dystrophy Registry will provide up-to-date information on the progress of clinical trials and can help determine which children are likely to be eligible for specific clinical trials. Your doctors will tell you how to register your child on this registry.
The North Star Adult Network, made up of expert neuromuscular disease consultants, allied health professionals, Duchenne muscular dystrophy patients themselves and Muscular Dystrophy UK, works to improve standard care and support for adults across the UK. Kingdoms. There is also a pediatric version, the North Star Project, which is working to improve care for children with Duchenne muscular dystrophy.
If you would like to find out more about the team's latest research, please contact the Research Department on 020 7803 4813 or by mail
Prof. Dr. Bruno-Marcel Mackert
Neurology
Head of the Department of Neurology
Specialization
- Internationally recognized specialist in stroke, peripheral nervous system diseases and clinical electrophysiology
- Author of over 40 original publications
- Board of Directors of the Berlin Stroke Society (BSA)
- Member of the Board of Directors of the Berlin Center for Stroke Research (CSB)
Show doctor's personal profile
Prof. Dr. Jörg Wissel, MD, FRCP
Neurological rehabilitation
Head of the Department of Neurological Rehabilitation and Physiotherapy, Department of Neurology and Rehabilitation Center
Specialization
- Neurological rehabilitation after stroke, traumatic brain injury and spinal cord injury
- Rehabilitation therapy for Parkinson's disease and dystonia
- Botulinum therapy
- Treatment of spasticity
- Neurological rehabilitation using intrathecal baclofen therapy and deep brain stimulation
- Author of more than 90 scientific publications, member of several expert commissions
Show doctor's personal profile