Compound
The tablets contain the active ingredient ibuprofen (200/400/500 mg) and excipients: potato starch, magnesium stearate, aerosil, vanillin, beeswax, food gelatin, azorubine dye, magnesium hydroxycarbonate, wheat flour, low molecular weight povidone, sucrose, dioxide titanium.
In the ointment and gel, the active substance is contained in a concentration of 50 mg/g, in the suspension - in a concentration of 20 mg/ml.
Auxiliary components of the gel: ethanol, propylene glycol, dimexide, carbomer 940, triethanolamine, neroli and lavender oil, methyl parahydroxybenzoate, purified water.
Auxiliary components of the ointment: dimethyl sulfoxide, macrogol 400 and 1500.
Ibuprofen in suppository form contains 60 mg of active substance and solid fat.
Pharmacodynamics and pharmacokinetics
The effects of the drug are due to the suppression of Pg biosynthesis by inhibiting the COX enzyme.
Suppresses platelet . It has no effect on proteins that are involved in blood clotting. Slightly increases bleeding time.
When applied externally, the patient experiences a decrease in joint pain at rest and during movement; reducing morning stiffness, swelling and swelling of the joints, increasing flexibility and range of motion of the joints.
When taken orally, it is well (80%) absorbed into the gastrointestinal tract. Concomitant use with food slows down absorption, but does not affect its volume. TSmax - 2-4 hours.
The hypothermic effect develops 1 hour after administration. T1/2 - from 2 to 4 hours. Communication with plasma proteins is 90-99%.
It penetrates into the joint cavities slowly, lingers in the synovial tissue, where it accumulates in higher concentrations than in the plasma.
Achieving an anti-inflammatory effect requires from several days to 2 weeks of systematic use of the drug.
Biological activity is associated with the S-enantiomer.
After absorption, the pharmacologically inactive R-form (about 60%) is slowly transformed into the S-form. Metabolic products are excreted primarily by the kidneys and, partly, with bile. In its pure form, no more than 1% of ibuprofen is excreted.
The substance is not detected in breast milk. Complete removal occurs within 24 hours.
Safety of ibuprofen in clinical practice
B
ol is the body’s main reaction to any tissue damage, so its relief is a problem for doctors of any specialty.
According to modern ideas about the mechanisms of development and transmission of the pain signal, a comprehensive approach using various groups of pharmacological agents is considered a reasonable treatment for pain, the mechanism of action of which is primarily aimed at suppressing the synthesis of inflammatory mediators and limiting the flow of nociceptive information from the periphery to the central nervous system.
Analgesics are widely used throughout the world. In England, more than 20 million people receive prescriptions for non-steroidal anti-inflammatory drugs (NSAIDs), and in one year (1999–2000) more than 100 million prescriptions were written for COX-2 inhibitors [18].
NSAIDs are most in demand primarily in rheumatic diseases for the relief of articular syndrome, in trauma, postoperative conditions, renal colic, migraine, dysmenorrhea, neurological diseases, and recently their preventive effect in colon cancer and Alzheimer's disease has been discussed. According to a survey conducted in Western European countries, NSAIDs are prescribed by more than 80% of general practitioners
[5,18].
The leading place in sales is occupied by over-the-counter analgesics, which are used as antipyretics and pain relievers of various origins: headaches, dental pain, dysmenorrhea, etc.
In 1998, 16.1 billion over-the-counter NSAIDs were sold in the United States, compared with 2.9 billion prescription ones. Of particular concern is the violation of the drug dosage regimen (about 1/3 of patients take prescription NSAIDs in larger doses than recommended by the doctor).
Given the predicted “aging” of the planet, the number of people needing to take NSAIDs will steadily increase. This poses a challenge for physicians to ensure the safety of NSAID treatment. In the United States, more people die each year from medical errors than from street injuries, lung cancer, and AIDS [22]. One of the reasons for this is ignorance of the mechanism of action of drugs, especially when used in combination, and possible adverse reactions.
Currently, the issue of safety of NSAIDs comes first. Possible side effects when using NSAIDs include damage to the gastrointestinal tract, impaired platelet aggregation, renal function, and a negative effect on the cardiovascular system. Gastrointestinal disorders are the most common side effects with NSAID use. Among the frequently used NSAIDs, we can highlight drugs that are particularly unfavorable in this regard - indomethacin, piroxicam, flurbiprofen; relatively safe drugs are ibuprofen, diclofenac, ketoprofen, as well as selective COX-2 inhibitors [4,9].
A number of researchers explain the clinical effect and the development of adverse reactions by the half-life of NSAIDs, with the more dangerous of them being long-lived ones (Table 1).
The development of side effects is often dose-dependent, as shown in Table 2, from which it follows that the analgesic dose of ibuprofen (1200 mg/day) is as safe as placebo. The main mechanism determining the safety of the drug is its ability to suppress the activity of cyclooxygenase-2 (Table 3). However, a direct relationship between the anti-inflammatory and analgesic effect and the severity of COX-2 inhibition was not identified. The most common side effects caused by inhibition of COX-1 and 5-lipoxygenase [19] are gastrointestinal damage, renal dysfunction, platelet aggregation, etc. (Table 4). It is believed that gastrointestinal side effects are one of the most common adverse events when using NSAIDs [27]. However, there was a clear dose dependence of the risk of developing NSAID gastropathy [14,16] (Table 5). A dose of ibuprofen 1200 mg/day is regarded as one of the safest in relation to gastrointestinal complications.
OTC NSAIDs are especially often used not only as analgesics, but also as antipyretics, competing with acetaminophen. A comparison of the effect of 400 mg of ibuprofen and 1000 mg of acetaminophen in the treatment of 113 patients with sore throat caused by tonsillitis-pharyngitis [10] showed that ibuprofen was significantly more effective, especially during the first 6 hours. With short-term use of these drugs, tolerability was equal.
A randomized trial of 3 analgesics: acetylsalicylic acid (ASA), acetaminophen, and ibuprofen was conducted in France and England with the participation of 1108 general practitioners. The study included 8677 adult patients with pain of musculoskeletal origin, throat, and acute respiratory infections [23]. Treatment was carried out for 1–7 days in doses: ASA and acetaminophen 3 g/day, ibuprofen up to 1.2 g/day. The frequency of significant adverse events when taking ASA was 18.7%, ibuprofen – 13.7%, acetaminophen – 14.5%. The total number of gastrointestinal complications was noted in 5.8% of those treated with ibuprofen, 7.3% with acetaminophen, and 10.6% with ASA. Gastrointestinal bleeding was absent in patients receiving ibuprofen, but was diagnosed in 4 patients on acetaminophen (which does not inhibit COX-1) and in 2 patients on ASA.
In terms of the time of development of gastrointestinal complications, treatment with ASA was the most unfavorable, because they appeared already on the first day after taking 1-2 tablets. Commission conclusion: General practitioners should give preference to ibuprofen over ASA and acetaminophen
due to the poorer tolerability of ASA and the potential for acetaminophen overdose.
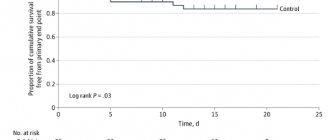
The high safety of ibuprofen is also evidenced by the fact that it has been an over-the-counter drug for more than 20 years in the country where it was created in 1962 by S. Adams et al., who worked at Boots (UK) (Fig. 1) .
Rice. 1. Risk of upper gastrointestinal bleeding associated with NSAID use [17]
Undesirable complications include complications from the cardiovascular system, in particular, heart failure, the risk of which is higher in patients with arterial hypertension, heart and kidney diseases (Table 6) [24]. According to the ANA, the frequency of these events when using NSAIDs in patients with hypertension exceeds 25%. The likelihood of developing heart failure is higher when using NSAIDs with a long half-life (piroxicam) than with a short half-life (ibuprofen, diclofenac). The risk of developing heart failure is higher in people over 55 years of age, especially in those taking diuretics. A randomized study of 8059 patients with rheumatoid arthritis and osteoarthritis receiving celecoxib 400 mg/day, ibuprofen 800 mg/day, diclofenac 75 mg/day. showed an equal frequency of cardiovascular complications [1].
A study of the effect of NSAIDs on blood pressure in 1213 hypertensive patients showed that when taking ibuprofen, mean blood pressure decreased by 0.3 mmHg. and increases by 6.1 mm Hg. when taking naproxen [25].
Neither classical NSAIDs nor selective COX-2 inhibitors provide cardioprotection, with the exception of low-dose ASA, which irreversibly inhibits COX-1 activity in platelets. The work [13] showed that taking ibuprofen before ASA can block the inhibition of platelet COX-1 and reduce platelet aggregation caused by ASA, without affecting the level of serum thromboxane B2. This fact should be taken into account when treating patients receiving ASA for the prevention of vascular complications, and its use should be recommended before ibuprofen, because this sequence does not cancel the effect of acetylsalicylic acid.
With the advent of a new class of NSAIDs—selective COX-2 inhibitors—the issue of their analgesic effectiveness compared to classical NSAIDs is being actively discussed [21]. The authors of this review indicate that in the literature, clinical studies of the effectiveness of selective COX-2 inhibitors in the treatment of non-arthritic diseases either give ambiguous results or are absent. Analgesia for postoperative dental pain with rofecoxib at a dose of 50 mg was equal to 400 mg of ibuprofen, and 200 mg of celecoxib was weaker. With regard to acute tonic pain, there is no evidence of equality between these two groups of NSAIDs. The authors believe that to achieve the maximum analgesic effect, inhibition of both COX isoforms is necessary, because There is evidence of a temporal and dynamic relationship between COX-1 and COX-2 and their participation in the formation of Pg E2 and subsequent clinical manifestations of pain [23].
The relative risk of developing edema in clinical practice among hypertensive patients in the United States is presented in Figure 2 [28]. As we see, ibuprofen has a clear advantage over the compared drugs.
Rice. 2. Relative risk of developing edema in clinical practice [31]
The
CLASS
[14], which compared the effect and tolerability of celecoxib and ibuprofen, showed that ibuprofen is inferior to celecoxib in the incidence of edema and increased blood pressure, but is safer than rofecoxib (Fig. 3).
Rice. 3. Hypertension and edema [14]
In rheumatology, NSAIDs are prescribed for almost all diseases, given their triple mechanism of action. In the foreign literature, the algorithm for the treatment of osteoarthritis is widely discussed, in which acetaminophen is placed in first place. A double-blind randomized study conducted [11] showed that in patients with gonarthrosis, the anti-inflammatory dose of ibuprofen was 2.4 g/day. was more effective than analgesic – 1.2 g/day. and 4.0 g/day. acetaminophen, which was confirmed by a decrease in joint pain and improvement in motor function.
An analysis of Medline data on the effect of various analgesics (meloxicam, naproxen, diclofenac, ibuprofen, celecoxib, rofecoxib, codeine, morphine [8]) on the severity of pain in osteoarthritis (OA) showed that the best clinical effect was achieved with the use of ibuprofen, diclofenac and naproxen.
A review [12] on the treatment of OA presents the results of a double-blind study of ibuprofen and benoxyprofen in a 4-week study, indicating a reduction in pain by 21% in both groups. Similar results were obtained when comparing fenoprofen calcium and ibuprofen.
Data [15,26] indicate equal effectiveness for gonarthrosis of ibuprofen at a dose of 1.2–2.4 g/day. and tramadol 200–400 mg/day, which once again confirms the high analgesic effect of ibuprofen.
A common reason for visiting a doctor and an equally common disability is low back pain (LBP), in which the acute phase of pain is usually limited to 7–8 days. NSAIDs are the drugs of choice for the management of this pain [6]. A comparative randomized study in which 48.3% of patients suffered from LBP showed that 1200 mg/day. ibuprofen is equivalent to 3 g of acetaminophen, more effective than 3 g of ASA and safer than ASA and acetaminophen [6].
The analgesic effect of 1200 mg ibuprofen for LBP was confirmed in one study [2], where it was shown that the average pain intensity according to VAS decreased by more than half on the second day, and by the sixth day it completely or significantly decreased in 73% of patients.
In the United States, up to 30% of visits to the doctor are related to fever in children [7]. Ibuprofen is allowed to be used as an antipyretic at a dose of 5–20 mg/kg, which is comparable to the effect of acetaminophen.
Issues of the effectiveness and safety of ibuprofen in pediatric practice are covered in the review of Prof. Geppe HA [3]. Pediatricians consider ibuprofen to be the best-tolerated NSAID in children
. Prof. Antret-Leca [3] concluded: “Compared with acetaminophen and ASA, ibuprofen has less toxicity in overdose and therefore a wider therapeutic range.”
The safety of ibuprofen is evidenced by the fact that it is approved for the treatment of children under 2 years of age. An analysis of treatment (double-blind study) of 84,000 children under 2 years of age for febrile illness with ibuprofen at a dose of 5–10 mg/kg and acetaminophen 12 mg/kg showed that ibuprofen did not increase the risk of hospitalization in children [20].
The presented data indicate that ibuprofen has a high analgesic effect at a dose of up to 1200 mg/day, is well tolerated by adults and children, is used in infants and premature infants, and is not inferior in tolerance to selective COX-2 inhibitors.
Literature:
1. Belousov Yu.B., Gurevich K.G. The effect of NSAIDs and paracetamol on the cardiovascular system. Wedge. pharmacological therapy, 2002, 5, 5–7
2. Vein A.M., Danilov A.B. The effectiveness of solpofex in the treatment of low back pain. Wedge. Pharmacol. Therapy, 1999, 8, 2, 47–78
3. Geppe NA First international conference on the use of ibuprofen in pediatric breast cancer, 2002, t10, no. 18, 831–835
4. Nasonov E.L. NSAIDs for rheumatic diseases: standard of treatment. RMZh, 2001, t9, no. 7–8, 265–270
5. Nasonov E.L. Use of NSAIDs: therapeutic aspects. RMJ, 2002, t10, no. 4, 206–212
6. Nasonova V.A. NSAIDs for acute pain in the lower back. Consilium medicum, 2002, v4, no. 2, 102–106
7. Tabolin V.A., Osmanov I.M., Dlin V.V. The use of antipyretics in childhood. Wedge. pharmak. therapy, 2002, t11, no. 5, 12–14
8. Babul N., Peloso PM Comparative Pharmacologic Response of analgesic agents on key outcome variables in osteoarthritis. X World Congress on Pain, USA, 2002 P 211
9. Biarnason IT The effects on NSAIDs on the small intestine: clinical implications. New Standards in Arthritis Care, 1997, v6, N 2, p2
10. Bourean F., Pelen F., ea Evaluation of Ibuprofen is Paracetamol Analgesic Activity using a Sore Throat Pain Model. Clin. Drug Invest., 1999, 17(1), 1–8
11. Brodley ID, Brandt KD, Kats BP ea Comparison of anti–inflammatory dose of ibuprofen, an analgesic dose of ibuprofen and acetomenofen in the treatment of patients with osteoarthritis. N.Eugl. J. med., 1991, 325, 87–91
12. Brandt KD The role of Analgesics in the Management of OA Pain Amer. J. Therapeutics, 2000, v7 N2, 75–90
13. Catella–Lawson F. E a Cyclooxygenase inhibitors and the Antiplatelet effects of Aspirin. The New Eugr. J.Med., 2001, v345, 25, 1809–17
14. CLASS Advisory Committee Briefing Document FDA Arthritis Advisory Committee Meeting 2001, Maryland, Gaithersburg
15. Dalgin P. Comparison of tramadol HCL and ibuprofen for the chronic pain of OA. Arthr. Rheum., 1997, 40, 586
16. Gabriel SE, Iaakkimainen L. ea Risk for serious gasthrointestinal complications related to use of NSAID. A meta-analysis. Am. Yntern. Med., 1991, 115: 787–796
17. Guthann S., Rodrigues G., Raiford FS Individual NSAIDs and other risk factors for Upper gastrointestinal bleeding and perforation. Epidemiology, 1997, 8, 18–24
18. Hillis WS Areas of Emerging interest in analgesics: cardiovascular complications. Am. J. Therapeutics, 2002, 9, 259–69
19. Laufer S., Tries S. Pharmacological profile of a new pyrrolizine derivative inhibiting the Enzymes COX and 5-lipoxygenase. Arzneim-Forsch Drug Res., 1994, 44: 629–636
20. Lesco SM The safety of acetaminophen and ibuprofen children less than two years old/ Pediatrics, 1999, 104, 4, 1–5
21. McCormack K., Twycross R. Are COX–2 selective inhibitors effective analgesics? Pain Reviews, 2001, 8, 13–26
22. Medical errors in the USA WHO pharmaceuticals Newsletter, 2000, N2, 13–14
23. Moore N. ea The pain study: paracetamol, aspirin, ibuprofen: New tolerance. Clinical Drug Invest., 1999, 18(2), 89–98
24. Page J., Henry D. Development of congestive heart failure in elderly patients: an under recognized public health problem. Arch. Int. Med., 2000, 160, 777–84
25. Pope JE, Anderson II, Felson DTA meta–analysis of the effects of NSAIDs on blood pressure. Arch. Int. Med., 1993, 153, 477–84
26. Reid E. Tramadol in Musculoskeletal Pain—a Survey. Clin. Rheumat., 2002, v21(suppl. 1), 9–12
27. Singh G. Gastrointestinal complications of prescription and over the counter NSAID; A view from the ARAMIS Database. Am. J. of Therapeutics, 2000, 7, 115–121
28. Zhao S. ea Comparison of edema clines associated with rofecoxib, celecoxib, and traditional NSAIDs among stable hypertensive patients in the US insured population. Am. Rheum. Dis., 2002, v 61, suppl 1, p 346
Indications for use
Ibuprofen - what is it?
Ibuprofen is a non-narcotic analgesic that belongs to the NSAID group. Has pronounced anti-inflammatory activity.
These properties allow the drug to be used for heat and pain (mild and moderate intensity), polymyalgia rheumatica , and inflammatory and degenerative diseases of the musculoskeletal system.
Ibuprofen is included in the WHO list of essential medicines.
What is Ibuprofen tablets for?
Tablets are prescribed for:
- inflammatory diseases of the spine and joints ( ankylosing spondylitis , gouty and rheumatoid arthritis , osteoarthritis , etc.);
- moderate pain of various etiologies (the medicine helps with pain during menstruation, toothache, headache, migraine attack , myalgia , neuralgia , post-traumatic and postoperative pain, etc.);
- fever due to infectious or colds.
It should be remembered that tablets (like other dosage forms) are intended for symptomatic therapy, reducing pain intensity and relieving inflammation; the medicine has no effect on the progression of pathology.
Indications for use of gel and ointment
Gel and ointment with ibuprofen are effective for inflammatory and degenerative diseases of the musculoskeletal system:
- psoriatic , gouty and rheumatoid arthritis ;
- humeroscapular periarthritis;
- osteoarthritis;
- radicular syndrome in osteochondrosis ;
- ankylosing spondylitis;
- bursitis;
- sciatica;
- lumbago;
- radiculitis;
- myalgia;
- tendovaginitis;
- tendonitis;
- worsened gout;
- injuries in which the integrity of soft tissues is not compromised (rupture/sprain of ligaments, dislocation, bruise, post-traumatic swelling, etc.).
Indications for use of suppositories and syrup
Ibuprofen syrup and suppositories are dosage forms that were developed specifically for use in pediatric practice. They are prescribed to children for:
- reducing temperature during acute respiratory viral infections , childhood infections, influenza and other infectious and inflammatory diseases ;
- decrease in temperature during post-vaccination reactions;
- reducing the intensity of mild/moderate pain (the product can be used for toothache and headache, ear or throat pain, ligament damage, neuralgia, etc.).
Suppositories are intended for children 3-24 months, Ibuprofen syrup is used to treat children from 3 months to 12 years.
What is Ibuprofen used for injection?
Injections are used to treat congenital heart disease in premature newborns.
Relevance
The results of the PRECISION-ABPM study were presented at the European Congress of Cardiology held in Barcelona.
The analysis found that ibuprofen was associated with increased blood pressure (BP) and hypertension compared with celecoxib in patients with osteoarthritis and rheumatoid arthritis. Nonsteroidal anti-inflammatory drugs (NSAIDs), both selective COX-2 inhibitors and non-selective drugs, are widely prescribed by doctors of all specialties. Thus, in developed countries, about 20% of individuals take at least one NSAID on a regular basis, and if we remember that the incidence of arterial hypertension in the general population is 40%, then the problem becomes of great importance.
Contraindications
General contraindications:
- complete or partial combination of symptoms of the Fernand-Vidal triad (including a history);
- the presence of erosions and ulcers in the digestive canal;
- hemostasis disorders ;
- active gastric/intestinal bleeding ;
- severe liver failure;
- progressive kidney pathologies;
- renal failure in which Clcr does not exceed 30 ml/min;
- conditions after CABG ( coronary artery bypass grafting );
- chronic inflammatory processes in the intestines;
- confirmed hyperkalemia ;
- 3rd trimester of pregnancy;
- hypersensitivity.
In pediatrics, suspension and suppositories are used from 3 months, tablets - from 6 years of age.
Caution should be exercised when prescribing Ibuprofen for:
- liver cirrhosis , which is complicated by portal hypertension ;
- gastritis;
- colitis;
- enteritis;
- history of stomach/duodenal ulcer
- nephrotic syndrome;
- insufficiency of heart, kidney or liver function;
- IHD;
- arterial hypertension;
- cerebrovascular diseases;
- dys- or hyperlipidemia ;
- peripheral arterial diseases;
- the presence of Helicobacter pylori infection ;
- severe somatic pathologies;
- blood diseases of unknown etiology.
The drug is also prescribed with caution to persons suffering from alcoholism , long-term use of NSAIDs, taking oral corticosteroids, SSRIs, antiplatelet agents and anticoagulants, in the first 26-27 weeks of pregnancy, and lactating women.
Children under one year of age should be given the drug only on the recommendation of a pediatrician.
Contraindications and adverse reactions
Contraindications for all forms of medications include:
- stomach ulcers;
- problems with liver function;
- bearing a child (3rd trimester);
- internal bleeding;
- progressive kidney disease;
- chronic intestinal diseases;
- hypersensitivity to the constituent components.
It should be taken with caution for the following conditions and problems: liver cirrhosis, gastritis, stomach ulcers, problems with the cardiovascular system, liver and kidneys.
Children under 12 months can be given medicine only as prescribed by a doctor and under his supervision.
When using suppositories and tablets, the following adverse reactions may occur;
- irritation and dryness in the mouth;
- dyspnea;
- blurred vision;
- headache;
- confused thinking;
- disturbed sleep;
- high blood pressure;
- excessive sweating.
Side effects
The annotation for dosage forms for oral use and rectal suppositories lists the following side effects:
- NSAID gastropathy , dryness, irritation and/or ulceration of the oral mucosa, pain in the mouth, pancreatitis , aphthous stomatitis ;
- hepatitis;
- bronchospasm , shortness of breath ;
- noise/ringing in the ears, hearing loss;
- double vision or decreased clarity of visual images, irritation and dry eyes, toxic damage to the optic nerve , scotoma , swelling of the eyelids, swelling of the conjunctiva;
- nervousness, headache, anxiety, confusion, insomnia/drowsiness, dizziness, mental and motor agitation, hallucinations, depression, aseptic meningitis (rare and mainly in patients with autoimmune diseases );
- decreased contractility of the heart muscle, increased blood pressure, tachycardia ; acute renal failure, polyuria , nephrotic syndrome , allergic nephritis , cystitis ;
- hypersensitivity reactions;
- anemia , thrombocyto- and leukopenia , Werlhof's disease , agranulocytosis ;
- increased sweating.
The likelihood of visual impairment, development of gastric/intestinal bleeding and ulceration of the walls of the digestive canal increases with long-term use of high doses of Ibuprofen.
The drug affects laboratory parameters, namely:
- increases bleeding time;
- reduces serum glucose concentration, Clcr, hematocrit and hemoglobin ;
- increases the activity of liver transaminases;
- increases the concentration of creatinine in the blood serum.
Side effects when applied topically in gel/ointment form:
- tingling/burning sensation;
- skin hyperemia.
With long-term use of external therapy, the systemic effects inherent in all NSAIDs may develop.
Ibuprofen-Hemofarm (tablets)
The risk of side effects can be minimized if the drug is taken in a short course, at the minimum effective dose required to eliminate symptoms.
Elderly people experience an increased incidence of adverse reactions with NSAID use, especially gastrointestinal bleeding and perforation, in some cases fatal.
Side effects are predominantly dose-dependent.
The following adverse reactions were observed with short-term use of ibuprofen in doses not exceeding 1200 mg/day (6 tablets). When treating chronic conditions and with long-term use, other adverse reactions may occur.
The frequency of adverse reactions (ARs) listed below is listed according to the following classification: very common (≥ 10%), common (≥ 1% but < 10%), uncommon (≥ 0.1% but < 1%) , rare (≥ 0.01% but < 0.1%), very rare (< 0.01%), frequency unknown - frequency cannot be estimated from available data.
Blood and lymphatic system disorders
Very rare:
hematopoietic disorders (anemia, leukopenia, aplastic anemia, hemolytic anemia, thrombocytopenia, pancytopenia, agranulocytosis). The first symptoms of such disorders are fever, sore throat, superficial oral ulcers, flu-like symptoms, severe weakness, nosebleeds and subcutaneous hemorrhages, bleeding and bruising of unknown etiology.
Immune system disorders
Uncommon:
hypersensitivity reactions - nonspecific allergic reactions and anaphylactic reactions, reactions from the respiratory tract (bronchial asthma, including its exacerbation, bronchospasm, shortness of breath, dyspnea), skin reactions (itching, urticaria, purpura, Quincke's edema, exfoliative and bullous dermatoses, including toxic epidermal necrolysis (Lyell's syndrome), Stevens-Johnson syndrome, erythema multiforme), allergic rhinitis, eosinophilia.
Very rare:
severe hypersensitivity reactions, including swelling of the face, tongue and larynx, shortness of breath, tachycardia, arterial hypotension (anaphylaxis, Quincke's edema or severe anaphylactic shock).
Gastrointestinal disorders
Uncommon:
abdominal pain, nausea, dyspepsia (including heartburn, bloating).
Rare:
diarrhea, flatulence, constipation, vomiting.
Very rare:
peptic ulcer, perforation or gastrointestinal bleeding, melena, hematemesis, in some cases fatal, especially in elderly patients, ulcerative stomatitis, gastritis.
Frequency unknown:
exacerbation of colitis and Crohn's disease.
Disorders of the liver and biliary tract
Very rare:
liver dysfunction (especially with long-term use), increased activity of “liver” transaminases, hepatitis and jaundice.
Renal and urinary tract disorders
Very rare:
acute renal failure (compensated and decompensated), especially with long-term use, in combination with an increase in the concentration of urea in the blood plasma and the appearance of edema, hematuria and proteinuria, nephritic syndrome, nephrotic syndrome, papillary necrosis, interstitial nephritis, cystitis.
Nervous system disorders
Uncommon:
headache.
Very rare:
aseptic meningitis.
Cardiovascular disorders
Frequency unknown:
heart failure, peripheral edema, with long-term use there is an increased risk of thrombotic complications (for example, myocardial infarction), increased blood pressure.
Disorders of the respiratory system and mediastinal organs
Frequency unknown:
bronchial asthma, bronchospasm, shortness of breath.
Laboratory indicators
- hematocrit or hemoglobin (may decrease);
- bleeding time (may increase);
- plasma glucose concentration (may decrease);
- creatinine clearance (may decrease);
- plasma creatinine concentration (may increase);
- activity of “liver” transaminases (may increase).
If any of the side effects indicated in the instructions get worse, or you notice any other side effects not listed in the instructions, tell your doctor.
Instructions for use of Ibuprofen (Method and dosage)
Ibuprofen tablets, instructions for use
The optimal dosage for children over 12 years of age and adults is 3-4 tablets of 200 mg. To achieve the desired effect, the dose can be increased to 1.2 g/day. (it should be divided into 3 doses).
When the required therapeutic effect is achieved, the daily dose should be reduced to 3-4 tablets of 200 mg per day.
The first dose is taken in the morning before meals, with a sufficient amount of liquid (this will allow the drug to be absorbed more quickly into the gastrointestinal tract). Later throughout the day, tablets are taken after meals.
The highest single dose is 400 mg (2 tablets of 200 mg), daily dose is 1.2 g (no more than 6 tablets of 200 mg within 24 hours). It is not recommended to take a repeat dose earlier than after 4 hours. Without medical advice, the drug should be taken for no more than 5 days in a row. Also, consultation with a specialist is necessary in cases where the tablets are used to treat a child under 12 years of age.
A child 6-12 years old can be given 1 tablet up to 4 times a day. A prerequisite is a weight of more than 20 kg. An interval of at least 6 hours should be maintained between tablet doses. The highest dose for this group of patients is 30 mg/kg/day.
There is no difference in how to take drugs from different manufacturers (for example, Ibuprofen-Belmed, Ibuprofen-Hemofarm or Ibuprofen-Darnitsa).
Instructions for candles
Suppositories are used rectally.
For pain and fever, the drug should be dosed based on the age and weight of the child. A single dose varies from 5 to 10 mg/kg. Frequency of applications - 3-4 rubles/day. The highest dose is 30 mg/kg/day.
The instructions for use for children indicate that patients weighing from 5.5 to 8 kg (3-9 months) should be administered 60 mg (1 suppository) every 6-8 hours, but no more than 3 suppositories per day. day. The highest dose for patients weighing from 8 to 12.5 kg (9-24 months) is 240 mg/day. (4 suppositories of 60 mg each).
To relieve fever, which is a consequence of immunization, in children under 12 months. 1 suppository of 60 mg should be administered and, if necessary, another 1 after 6 hours.
Ibuprofen suppositories can be used as an antipyretic for children for no more than 3 days. in a row, and as an analgesic - no more than 5 days. contract.
If fever persists after this time, consult a doctor.
Ibuprofen gel, instructions for use
Adults and children over 12 years of age should squeeze out a strip of gel 4-10 cm long and rub the drug with light movements until completely absorbed into the area of pain projection.
The procedure can be repeated no earlier than 4 hours later. Ibuprofen is used no more than 4 times during the day. The dose depends on the extent of the painful area and varies from 50 to 125 mg.
For children 6-12 years old, a single dose is equal to the volume of a gel strip 2 to 4 cm long. The drug can be used no more than 3 times a day.
Treatment is continued for 2 to 3 weeks.
Ibuprofen ointment, instructions for use
The ointment is applied externally in the same way as the gel. The medicine is applied to the painful area 3 or 4 times a day. within 2-3 weeks. A single dose is equal to the volume of a gel strip 5 to 10 cm long.
How to take children's Ibuprofen (suspension)?
The suspension is given to children 3 times a day. at a dose of 5-10 mg/kg.
Children under one year of age can be given the drug only as prescribed by a pediatrician. The highest dose for infants is 10 ml/day. (2.5 ml 4 times/day).
Syrup for children from one to 12 years old is given 3 rubles per day. in a dose of 5 to 15 ml.
If pain and fever in a 3-6 month old child are a consequence of vaccination, 2 times a day should be given per 5-7.6 kg of body weight. 2.5 ml of suspension. After the first dose, the drug is repeated no earlier than 6 hours later.
Instructions for Ibuprofen solution for children
Ibuprofen injections are prescribed exclusively to premature infants with heart pathologies (in particular, with an unclosed ductus arteriosus).
Treatment is carried out in the intensive care unit and under the supervision of a neonatologist. Ibuprofen is administered intravenously 3 times at intervals of 24 hours. The dosage is selected depending on the child’s weight.
The first dose is 10, the second and third are 5 mg/kg.
The drug is infused slowly (over 15 minutes), preferably undiluted. If necessary, the injected volume is adjusted with 0.9% NaCl solution (or 5% glucose). The remaining unused solution is disposed of.
When determining the volume of injected solution, the total daily volume of prescribed fluid is taken into account.
If, after the child receives 1 or 2 doses, he develops overt oliguria or anuria , the next dose is administered only after restoration of normal diuresis .
If the botal duct is open 24 hours after the last dose or opens again, a repeat course is allowed, which also consists of 3 doses of the drug. If in this case it is not possible to achieve closure of the duct, the child may require surgical treatment.
PRECISION-ABPM Study
The PRECISION-ABPM study is part of the larger PRECISION study. The researchers assessed the effect of the NSAIDs celecoxib, naproxen and ibuprofen on blood pressure levels over a 4-month period.
PRECISION-ABPM is a double-blind, randomized, non-inferiority study. The study was conducted at 60 centers in the United States and included 444 patients, of whom 408 (92%) had osteoarthritis and 36 (8%) had rheumatoid arthritis.
Patients were randomized in a 1:1:1 ratio to receive celecoxib (100–200 mg twice daily), ibuprofen (600–800 mg three times daily), or naproxen (375–500 mg twice daily).
The primary endpoint was the change in blood pressure after 4 months of therapy (outpatient 24-hour blood pressure monitoring).
Overdose
Overdose is accompanied by:
- abdominal pain;
- lethargy;
- nausea/vomiting;
- tinnitus;
- drowsiness;
- headache;
- depression;
- metabolic acidosis;
- coma;
- surge arrester;
- bradycardia;
- hypotension;
- atrial fibrillation;
- stopping breathing.
Treatment: gastric lavage (advisable within 1 hour after taking the drug), administration of enterosorbents, forced diuresis, abundant alkaline drinking, symptomatic therapy, the purpose of which is the correction of gastric and intestinal bleeding, blood pressure, blood pressure levels, etc.
Interaction
Drugs that induce microsomal oxidation increase the production of hydroxylated active metabolic products and thus increase the risk of developing serious hepatotoxic reactions. Drugs that inhibit microsomal oxidation, on the contrary, reduce it.
Ibuprofen reduces the sodium and diuretic activity of hydrochlorothiazide and Furosemide , the effectiveness of antihypertensive and uricosuric drugs (including ACE inhibitors and BMCC), and the antiplatelet and anti-inflammatory effects of ASA.
Potentiates the effect of antiplatelet agents, indirect anticoagulants, fibrinolytics, Insulin and oral forms of hypoglycemic drugs, ulcerogenic effect with bleeding of GCS and MCS.
Absorption of the drug is reduced in combination with cholestyramine and antacids. Caffeine enhances the analgesic effect . In combination with thrombolytics and anticoagulants, it increases the risk of bleeding.
Cefotetan , Cefoperazone , Cefamandole , Plicamycin and valproic acid prothrombin (clotting factor) deficiency
Myelotoxic drugs enhance the hematotoxicity of Ibuprofen. The drugs Au and Cyclosporine enhance the effect of the drug on the synthesis of Pg in the kidneys, resulting in increased nephrotoxicity. In turn, Ibuprofen increases the concentration of Cyclosporine in the blood plasma and its hepatotoxicity.
Drugs that block tubular secretion increase the concentration of ibuprofen in the blood plasma and reduce its excretion.
IBUPROFEN-CHEMOPHARM
Interaction
Concomitant use of ibuprofen with acetylsalicylic acid and other NSAIDs is not recommended.
When administered simultaneously, ibuprofen reduces the anti-inflammatory and antiplatelet effects of ASA (an increase in the incidence of acute coronary insufficiency in patients receiving small doses of ASA as an antiplatelet agent is possible after starting ibuprofen).
When prescribed with anticoagulant and thrombolytic drugs (alteplase, streptokinase, urokinase), the risk of bleeding simultaneously increases.
Concomitant use with serotonin reuptake inhibitors (citalopram, fluoxetine, paroxetine, sertraline) increases the risk of developing serious gastrointestinal bleeding. Cefamandole, cefaperazone, cefotetan, valproic acid, plicachycin increase the incidence of hypoprothrombinemia.
Cyclosporine and gold preparations enhance the effect of ibuprofen on the synthesis of prostaglandins in the kidneys, which is manifested by increased nephrotoxicity. Ibuprofen increases the plasma concentration of cyclosporine and the likelihood of developing its hepatotoxic effects.
Drugs that block tubular secretion reduce excretion and increase plasma concentrations of ibuprofen.
Inducers of microsomal oxidation (phenytoin, ethanol, barbiturates, rifampicin, phenylbutazone, tricyclic antidepressants) increase the production of hydroxylated active metabolites, increasing the risk of developing severe hepatotoxic intoxications.
Microsomal oxidation inhibitors reduce the risk of hepatotoxicity.
Reduces the hypotensive activity of vasodilators (including slow calcium channel blockers (SCBC), angiotensin-converting enzyme (ACE) inhibitors), natriuretic and diuretic activity - furosemide and hydrochlorothiazide.
Reduces the effectiveness of uricosuric drugs, enhances the effect of indirect anticoagulants, antiplatelet agents, fibrinolytics (increasing the risk of hemorrhagic complications), enhances the ulcerogenic effect with bleeding of mineralocorticosteroids (MCS) and glucocorticosteroids (GCS), colchicine, estrogens, ethanol.
Enhances the effect of oral hypoglycemic drugs (including sulfonylurea derivatives) and insulin.
Antacids and cholestyramine reduce the absorption of ibuprofen.
Increases the blood concentration of digoxin, lithium and methotrexate.
Caffeine enhances the analgesic effect.
Myelotoxic drugs increase the manifestations of hematotoxicity of the drug.
special instructions
In case of severe pathologies of the musculoskeletal system, it is advisable to combine external therapy with oral forms of NSAIDs.
During the period of use of Ibuprofen, it is necessary to monitor changes in renal/liver function and peripheral blood patterns.
If signs of NSAID gastropathy , the patient requires a blood test to determine the hematocrit number and Hb, a stool test for occult blood, and esophagogastroduodenoscopy. To prevent the development of gastropathy , Ibuprofen should be combined with PgE medications.
If it is necessary to determine 17-KS, the drug is discontinued 48 hours before the study.
Patients taking Ibuprofen should refrain from any activity that requires high concentration and speed of mental/motor reactions.
It should be remembered that this remedy should be used in the minimum effective dose and for the shortest possible course to reduce the likelihood of developing undesirable reactions from the digestive system.
Instructions for use IBUPROFEN
Inducers of microsomal oxidation (phenytoin, ethanol, barbiturates, rifampicin, phenylbutazone, tricyclic antidepressants) increase the production of hydroxylated active metabolites, increasing the risk of severe hepatotoxic reactions.
Microsomal oxidation inhibitors reduce the risk of hepatotoxicity. Reduces the hypotensive activity of vasodilators (including slow calcium channel blockers and angiotensin-converting enzyme inhibitors), natriuretic and diuretic activity of furosemide and hydrochlorothiazide. Reduces the effectiveness of uricosuric drugs, enhances the effect of indirect anticoagulants, antiplatelet agents, fibrinolytics (increasing the risk of hemorrhagic complications).
When interacting with mineralocorticosteroids. glucocorticosteroids, colchicine, estrogen, ethanol can cause an ulcerogenic effect with bleeding. Enhances the effect of oral hypoglycemic drugs and insulin. Antacids and cholestyramine reduce the absorption of ibuprofen. Increases the blood concentration of digoxin, lithium and methotrexate.
Caffeine enhances the analgesic effect of ibuprofen. When administered simultaneously, ibuprofen reduces the anti-inflammatory and antiplatelet effect of acetylsalicylic acid (an increase in the incidence of acute coronary insufficiency in patients receiving small doses of acetylsalicylic acid as an antiplatelet agent is possible after starting ibuprofen).
When prescribed with anticoagulant and thrombolytic drugs (alteplase, streptokinase, urokinase), the risk of bleeding simultaneously increases.
Cefamandole, cefaperazone, cefotetan, valproic acid, plicamycin increase the incidence of hypoprothrombinemia.
Myelotoxic drugs increase the manifestations of hematotoxicity of the drug. Cyclosporine and gold preparations enhance the effect of ibuprofen on the synthesis of Pg in the kidneys, which is manifested by increased nephrotoxicity.
Ibuprofen increases the plasma concentration of cyclosporine and the likelihood of developing its hepatotoxic effects.
Drugs that block tubular secretion reduce excretion and increase plasma concentrations of ibuprofen.
When using ibuprofen simultaneously with potassium-sparing diuretics, there is a risk of developing hyperkalemia; with other non-steroidal anti-inflammatory drugs - the risk of side effects from the gastrointestinal tract increases.
Ibuprofen analogs
Level 4 ATC code matches:
Artrum
Brustan
Ketonal Duo
Nurofen Plus
Nurofen Express
Nurofen Forte
Nurofen Express Lady
Nurofen for children
Nurofen
Ibuprom
Advil
MIG 400
Has
Ketoprofen
Vimovo
Naproxen
Flexen
Nalgesin
Flamax
Novigan
Synonyms (analogs of Ibuprofen with the same active ingredient):
- Ibuprofen-Hemofarm
- Nurofen
- MIG 400
- Ibuprom
- Faspik
- Solpaflex
- Advil
Generic dosage forms for external therapy are the following drugs:
- Dolgit
- Ibalgin
- Nurofen
- Ibuprofen-Verte
Ibuprofen or Nurofen - which is better?
Nurofen is a medicine based on ibuprofen. That is, the drugs are generics. They are distinguished from each other by manufacturer, price and composition of auxiliary components.
Ibuprofen during pregnancy and lactation
Ibuprofen is the drug of choice for pain and fever during pregnancy, since during this period of time it is safer for the woman’s body than most other analgesics and antipyretics.
In the first 2 trimesters of pregnancy, it does not have a negative effect on the development of the fetus, does not provoke bleeding (unlike Aspirin ) and does not create a threat of miscarriage.
In the last trimester of pregnancy, taking Ibuprofen is contraindicated.
Firstly, the drug inhibits the contraction of the uterine muscles. Secondly, its use can cause closure of the ductus botellus and the development of pulmonary hypertension in a child. Thirdly, the medicine tends to block the hormones responsible for the birth process.
Ibuprofen during breastfeeding does not affect the quality and secretion of milk, therefore it can be used to treat nursing women.
How to take Ibuprofen
Pills
Adults and children over 14 years of age can be given no more than 4 tablets per day. Depending on the condition, the dose can be adjusted and increased to 6 tablets (the dose is divided into several doses). When improvement is noted, the dose should be reduced to the original. The first tablet should be taken in the morning before meals with a glass of water. Then take 1 tablet after meals.
Without consulting a doctor, tablets can be used for no more than 5 days.
Candles
The suppositories are placed rectally. For pain and fever, the dose is determined taking into account the age and body weight of the baby. You can use no more than 10 mg per 1 kg at a time. Candles can be lit up to 4 times per day. The optimal duration of use is 3 days. If suppositories are used as an analgesic, they can be administered for 5 days.
If after the allotted time the fever has not disappeared, then you should consult your pediatrician.
Gel
You can use a 5-9 cm strip of gel at a time. Using smooth, light movements, rub the gel into the problem area until the composition is completely absorbed. It is allowed to use the gel no more than 4 times per day, with repeated use no earlier than after 4 hours.
The duration of the treatment course can be 15-20 days.
Ointment
The scheme for using the ointment is in all respects similar to applying the gel. The drug is rubbed into the problem area of the skin 3-4 times a day. Can be used within 15-20 days.
Children's suspension
Ibuprofen in the form of a suspension can be given to a child no more than 3 times a day. If your child is under one year old, you should definitely consult a specialist before use. If the fever appears as a result of vaccination, then the suspension is given 2 times a day. There should be a break of at least 6 hours between doses.
Reviews of Ibuprofen
It is probably impossible to find bad reviews about Ibuprofen in tablets, suppositories or syrup. The drug is considered to be an effective and fairly safe remedy.
Its advantages are:
- possibility of use for the treatment of pregnant women and children of any age;
- a large number of dosage forms (this allows you to correctly select the minimum effective dose);
- low price;
- quick effect.
As disadvantages, reviews usually mention the presence of contraindications and the risk of developing side effects characteristic of NSAIDs.
Reviews of doctors about the ointment/gel allow us to conclude that for postoperative and post-traumatic pain, as well as for pain caused by severe hypothermia, drugs containing NSAIDs are the most fast-acting and effective.
However, they should be used in short courses and not exceeding the dose recommended by the instructions.
Ibuprofen price, where to buy
The price of Ibuprofen in tablets is from 40 to 100 rubles. How much tablets cost depends on their quantity in the package and the manufacturer’s pricing policy. Syrup can be bought for 100 - 150 rubles. The price of Ibuprofen ointment is from 40 rubles, the price of Ibuprofen gel is from 70 rubles. Candles for children cost an average of 80 rubles (package No. 10).
The average cost of Ibuprofen tablets in Kharkov, Kyiv and other cities of Ukraine is about 30 UAH, suspensions are about 100 UAH, for ointment and gel the price varies from 30 to 50 UAH.
- Online pharmacies in RussiaRussia
- Online pharmacies in UkraineUkraine
- Online pharmacies in KazakhstanKazakhstan
ZdravCity
- Ibuprofen-Akrikhin orange suspension.
for internal approx. 100mg/5ml vial. 100g (with dispenser syringe) Medana Pharma A.O. 96 RUR order - Ibuprofen Welfarm tab. p/o captivity. 200mg No. 50Velfarm LLC
RUB 242 order
- Ibuprofen gel for external use. approx. 5% 50gOzon LLC
74 RUR order
- Ibuprofen-AKOS tab. p/o captivity. 400 mg No. 50Sintez OJSC
124 RUR order
- Ibuprofen Welfarm tab. p/o captivity. 400 mg No. 10 Velpharm LLC
105 rub. order
Pharmacy Dialogue
- Ibuprofen-Akrikhin suspension 100mg/5ml bottle 100ml OrangeMedana Pharma
89 rub. order
- Ibuprofen tablets 400 mg No. 30 Hemofarm
66 RUR order
- Ibuprofen 5% gel tube 50gVertex
93 RUR order
- Ibuprofen (tab.p/v.200mg No. 20 (blister)) Biosynthesis OJSC
23 RUR order
- Ibuprofen Welfarm (tab.p.pl/vol. 400 mg No. 30) Welfarm LLC
RUB 219 order
show more
Pharmacy24
- Ibuprofen-Darnitsa 200 mg No. 20 tablets PrAT" Pharmaceutical company "Darnitsa", Ukraine
15 UAH. order - Ibuprofen-Darnitsa 0.2 g No. 50 tablets PrAT” Pharmaceutical company “Darnitsa”, Ukraine
28 UAH order
- Ibuprofen 200 mg N50 tablets PAT"Vitamin" Ukraine
27 UAH order
- Ibuprofen 200 mg No. 50 tablets PrAT "Technolog", Uman, Cherkasy region, Ukraine
22 UAH order
- Ibuprofen 200 mg No. 50 tablets PAT NEC "Borshchagivsky chemical and pharmaceutical plant", Kiev, Ukraine
24 UAH order
PaniPharmacy
- Gel Ibuprogel for joints ibuprofen with bodyaga 75 ml Ukraine, Euro plus state of emergency
32 UAH order
- IBUPROFEN tablets Ibuprofen-Darnitsa tablets 0.2g No. 50 Ukraine, Darnitsa ChAO
28 UAH order
- Ibuprofen tablets Ibuprofen tablets. p/o 200 mg No. 50 Ukraine, Tekhnolog ChAO
25 UAH order
- IBUPROFEN tablets Ibuprofen tablets. 0.2g No. 20 Ukraine, Darnitsa ChAO
16 UAH order
show more





![Table 1. Complications when taking NSAIDs and their diagnosis [1]](https://miass-medis.ru/wp-content/uploads/tablica-1-oslozhneniya-pri-prieme-npvp-i-ih-diagnostika-1-330x140.jpg)