Author: Skatov B.V., urologist-andrologist. Experience since 1996. September, 2021.
Male diseases, especially pathologies of the prostate (prostate gland), are in the area of close attention of both patients and doctors. The term “prostate adenoma” hurts the ears of a modern man, and the disease itself is surrounded by implausible myths, rumors and misconceptions. Let's try to debunk some of these myths and orient the reader to the correct actions when unpleasant symptoms are detected.
Synonyms: prostate adenoma, prostate adenoma, benign prostatic hyperplasia (BPH) - the last term is most used in international medical practice.
Prostate adenoma is the growth of the prostate gland from the inside, leading to obstruction of the urethra and a deterioration in the outflow of urine from the bladder.
As a result of disturbances in the prostatic zone of urine outflow, a man experiences frequent urge to urinate, difficulty emptying the bladder, up to complete cessation of urine outflow.
Prostate adenoma, prostatitis and oncology
Prostate adenoma differs fundamentally from prostatitis:
- Prostate adenoma is a neoplastic process, i.e. process with the formation of additional connective tissue.
- Prostatitis is a disease with pronounced signs of inflammation, primarily inflammatory changes in the tissues of the prostate itself.
Often a combination of these diseases is detected in the prostate gland - both prostatitis and prostatic hyperplasia.
BPH has nothing to do with varicocele - these diseases do not provoke each other and do not affect one another (as some believe), these are independent urological diseases.
Scientists have not fully figured out the connection between prostate hyperplasia and cancer, but studies are being conducted all over the world and the data is quite contradictory. Nevertheless, prostate adenoma is conventionally considered a precancerous disease and requires constant oncological vigilance with annual PSA monitoring.
What causes prostate hyperplasia?
Until now, the exact causes of this disease are not known. There is no clear relationship between the occurrence of prostate adenoma and excessively high or low sexual activity, alcohol abuse and smoking. The main role is played by imbalance in the levels of androgens and estrogens.
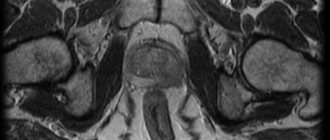
With age, against the background of hormonal imbalance, paraurethral glands grow in the central zone of the prostate. Histologically (under a microscope), the number of not only the glands themselves, but also the connective tissue may increase, so histologists distinguish glandular, stromal and glandular-stromal forms of prostate adenoma. Macroscopically, a nodule (or many nodules) forms in the prostate gland, which grows and gradually deforms not only the prostate gland itself, but also compresses the urethra. At the same time, the middle and lateral lobes are formed in the prostate depending on the number of nodes and their direction of growth. Therefore, the main symptom of the disease is primarily a deterioration in the quality of urination. Prostate hyperplasia itself is a benign process. It does not metastasize or grow into other organs, like prostate cancer. However, one way or another, the risk of the cells inside it degenerating into malignant ones exists. Therefore, it is necessary to monitor PSA levels and be sure to undergo regular examinations with a urologist.
Causes of prostate adenoma
Risk factors for developing prostatic hyperplasia include:
- age over 50 years,
- the level of prostate-specific antigen (PSA) in the blood is above 1.5 ng/ml,
- an increase in the volume of the prostate gland of more than 30 cm3, the presence of diabetes mellitus.
The main reason for the development of prostate adenoma is the increased activity of a specific enzyme - 5-alpha reductase. Under the influence of female sex hormones - estrogens (their concentration increases in men with age), the concentration of 5-alpha reductase increases. In turn, under the influence of this factor, testosterone in the prostate gland is converted into its byproduct - dihydrotestosterone, which leads to increased division of prostate cells, causing its growth.
Causes of prostate adenoma before 40 years of age
At a young age, men rarely acquire prostatic hyperplasia, but such cases do occur.
It's connected with
- genetic predisposition,
- low levels of the main sex hormone – testosterone,
- obesity,
- diabetes mellitus
Prevention of the prostate gland in men
There are certain rules for the prevention of prostate adenoma, following which you can maintain the health of this important organ:
- Follow a diet - reduce consumption of red meat and fatty foods. A man's diet should be dominated by vegetables, fruits, and omega acids;
- Increase physical activity – physical exercise has a positive effect on prostate health;
- Control your body weight – this will significantly reduce the risk of developing prostate adenoma;
- Minimize stress – will improve hormonal levels and slow down the development of the disease;
- Have an active sex life;
- After 45-50 years, be systematically examined by a urologist and take an analysis of the dog’s blood level.
Prostate adenoma, detected in the early stages of development, can be corrected with medication and non-surgically without any problems.
Timely contacting a urologist and unquestioningly following all his instructions for treating the disease in almost all cases guarantees stopping the growth of the gland and preventing urinary disorders. Late stages of the disease with symptoms that significantly reduce a man’s quality of life will require the use of surgical treatment methods. Therefore, early diagnosis of prostate adenoma is of great importance, which can be done in the modern medical center of Moscow - the Yusupov Hospital. The clinic’s high-tech diagnostic equipment ensures the most accurate research results, thanks to which Yusupov Hospital specialists select an effective individual treatment regimen for each patient, whenever possible, giving preference to non-surgical, gentle treatment methods.
Make an appointment
Symptoms of adenoma
The manifestations of BPH depend not only on the size of the prostate gland, but also on the location of the nodes in the prostate. The most severe obstruction of the urinary tract occurs when the nodes are localized in the middle lobe of the gland, close to the passage of the upper part of the urethra.
Symptoms of prostate adenoma may be associated with bladder filling disorders:
- frequent, sometimes unproductive, urge to urinate;
- frequent night urination (several times a night);
- unexpected leakage of urine (incontinence in various everyday situations - when coughing, laughing, etc.).
In addition, with prostatic hyperplasia there are a number of symptoms that reflect problems in emptying the bladder:
- difficulty starting to urinate;
- weak (sluggish) stream of urine;
- feeling of incomplete emptying of the bladder;
- the need to strain the lower abdomen at the beginning of urination;
- splashing stream of urine;
- urine dripping at the end of urination;
- interruption of the urine stream;
- An interesting symptom - urinary retention in combination with urinary incontinence (so-called paradoxical ischuria), indicates an advanced nature of the disease.
Also, with prostate adenoma, there are symptoms that occur after a person has urinated (post-mictional):
- feeling of incomplete emptying of the bladder;
- characteristic dripping of urine after completion of urination.
Among the unobvious, but often encountered symptoms, the following should be highlighted:
- discomfort, pain in the rectum, especially with large adenomas, when it puts pressure on the rectum - many patients complain about this;
- Pain during bowel movements and constipation are possible.
Pain due to prostatic hyperplasia
In addition to the above symptoms, a man may experience pain of varying nature and intensity in the perineum, rectum, and lower abdomen.
Pain in the lumbar region is not typical for prostate adenoma, but a pulling sensation may appear in the later stages of the disease, when the kidneys are damaged.
If an infectious process occurs in the area of the prostate or bladder, the body temperature may increase.
What is the clinical picture?
All symptoms of this disease are usually called lower urinary tract symptoms (LUTS) and are divided into storage symptoms and emptying symptoms.
Symptoms of accumulation:
- Urgent (urgent) urge to urinate;
- Frequent urination at night (nocturia);
- Frequent urination during the day (polyuria);
Symptoms of bowel movement:
- Sluggish stream of urine;
- Delay in starting urination;
- The need to tense the muscles of the anterior abdominal wall to begin urination;
- Intermittent urination (“urination in several passes”);
- Feeling of incomplete emptying of the bladder.
Obstruction of the normal flow of urine leads to overstrain of the bladder muscle, which is involved in the expulsion of urine (detrusor). This leads first to its hypertrophy (thickening of the muscle layer), then, when its capabilities “exhaust,” the bladder ceases to adequately expel urine and over time its wall can become thin, like “papyrus paper.”
According to the type of growth, they are distinguished:
- Intravesical form (the tumor grows towards the bladder).
- Retrotrigonal form in which the tumor is located under the triangle of the bladder.
- Subvesical form (the tumor grows towards the rectum).
The type of growth of the adenoma, and not its size, has a major role in the severity of this or that symptomatology. Also, in the presence of an adenoma and its practically asymptomatic course, errors in diet (abuse of spicy foods and alcohol), hypothermia or excessive overheating can provoke a sharp deterioration in symptoms, up to acute urinary retention.
Stages of development
Conventionally, there are three stages of manifestations of prostate adenoma. The main criteria are the volume of the prostate and the presence of “residual urine” - the amount that remains in the bladder after complete urination (determined by ultrasound).
Symptoms of the disease are grouped according to the International Index of Prostate Symptoms (IPSS), presented in points:
- minor symptoms - 0–7 points;
- moderate - 8–19 points;
- pronounced - 20–35 points
In stage I - the volume of the gland is 30-40 cm3, residual urine is insignificant, up to 40 ml.
In stage II - the volume of the gland reaches 40-60 cm3, residual urine can be up to 100 ml.
In stage III - the volume of the gland is very large, 60-80 cm3 or more, residual urine reaches a volume of more than one liter. At this stage, paradoxical ischuria develops, when, through a very weak external sphincter, urine randomly leaks from an overstretched bladder.
It should be understood that the stage of prostate adenoma does not always depend on the size of the prostate gland; the location of the gland in relation to the area of the urethra, as well as the time at which the process is neglected, is of great importance.
Possible complications
Self-medication, ignoring early symptoms of the disease, and neglecting doctor’s recommendations lead not only to a deterioration in the quality of life, but can also significantly affect the functions of many body systems.
- Acute urinary retention is possible in stages I and II of the disease. Most often, it is provoked by “overaccumulation” of urine in the bladder (when it is no longer able to contract adequately), excessive hypothermia or overheating, and errors in diet (alcohol, spicy foods).
- Bladder diverticula, hydronephrosis (expansion of the renal pyelocaliceal system, which leads to the progression of renal failure).
- Hematuria (blood in the urine) is caused by damage to varicose veins in the bladder neck (occurs in 20-30% of patients).
- Bladder stones are formed as a result of a constant large amount of residual urine.
Examinations and tests
Screening (primary) examination of the prostate includes:
- visiting a urologist;
- digital rectal examination;
- general urine analysis;
- PSA blood test;
- TRUSY;
- additional methods as needed.
Urologist
If you suspect a prostate adenoma and identify similar symptoms, the examination should begin with a visit to a urologist, who will first perform a digital rectal examination of the prostate gland.
Blood PSA
At the first stage of the examination, it is necessary to determine the level of PSA (prostate-specific antigen) in the blood to exclude oncological processes.
- You should be wary if the reading is above 1.5 ng/ml.
You should donate blood for PSA before performing TRUS, since due to possible microdamage to the prostate, the analysis may be unreliable. It is possible to donate blood a week after TRUS, when everything is restored.
OAM
At the same stage, they suggest taking a general urine test with sediment microscopy (SAM), which will allow you to identify inflammatory phenomena and obtain other important information.
TRUSY
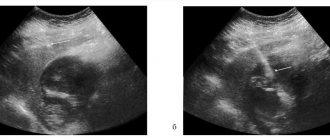
The next diagnostic step is the mandatory implementation of a transrectal ultrasound examination of the prostate gland - TRUS. Here the shape, size, consistency of the prostate, and the amount of residual urine are determined.
TRUS is performed with a full bladder, and after urination, the residual volume of urine is assessed. The main ECHO signs of the disease are the presence
- adenomatous nodes of the prostate gland,
- areas of hyperplastic (changed) tissue,
- increase in prostate size.
Sometimes in the TRUS report you can read the following terms:
- hyperplasia and diffuse changes in the prostate gland;
- prostatic hyperplasia with a heterogeneous structure.
There is nothing dangerous about this. This means that areas free from hyperplasia are changed, there are signs of concomitant prostatitis (inflammation), which requires additional therapy.
Additional Methods
Of particular importance in the diagnosis of prostate adenoma is the assessment of urination using uroflourometry (measurement of urine flow rate).
If an oncological process of the prostate gland and bladder, narrowing of the urethra and bladder neck, or urolithiasis is suspected, an in-depth examination is carried out using diagnostic measures such as:
- A biopsy (targeted sampling) of a section of the prostate gland is performed if cancer is suspected, with PSA above 4 ng/ml.
- The biopsy is performed by specialist urologists-oncologists.
- under TRUS control, through the anus, under local anesthesia, a sample is taken from questionable areas of the prostate gland, from at least 12 points, followed by examination of this tissue under a microscope.
Important! It should be noted that concomitant hemorrhoids (enlargement and inflammation of the hemorrhoids of the anus) sharply worsens the possibilities of examining patients with prostate adenoma and requires priority treatment, and if the examination cannot be postponed, then parallel treatment.
Benign prostatic hyperplasia (adenoma)
Authors:
- Doctor of Medical Sciences, Professor I.A. Aboyan
- Ph.D. S.V. Pavlov
- Ph.D. YES. Romodanov
- A.N. Tolmachev
The information presented here concerns one of the most common diseases in men - prostate adenoma. More than 1.5 million men in Russia consult urologists every year about this disease.
We believe that familiarity with this information will allow you and your relatives to better understand the disease and your condition.
If you have prostate adenoma...
In ordinary life, the question of the prostate gland does not arise in conversations, so you may have very little information about this internal organ. Like most men, you may only feel the need to learn about it if your urination patterns have changed or if you have learned that men over 40 are more likely to have “prostate problems.”
There are two good reasons to get information about your prostate and its diseases:
- “Prostate problems” can cause unpleasant symptoms; they do not necessarily accompany aging. With normal diagnosis and treatment, most of these symptoms can be eliminated.
- Prostate cancer, which is treatable if detected early, does not cause symptoms in the early stages of the disease. Early prostate cancer can only be detected through regular prostate examinations.
We want to highlight a specific prostate disease: a non-cancerous enlargement of the prostate called ADENOMA or benign prostatic hyperplasia (BPH), which begins to develop after age 40. If you are in this age group, then this information will help you.
What is the prostate?
The prostate is a gland of the male reproductive system. It is located in front of the rectum, under the bladder and surrounds the urethra (urethra). The prostate is small in size, weighing about 28g. both in size and shape resembles a walnut.
What is DGP?
BPH is a benign tumor that primarily affects the deep inside part of the prostate through which the urethra passes. The development of BPH leads to compression of the urethra and urination disorders.
It is important to note that BPH is not cancer and does not lead to cancer, although men can have both BPH and prostate cancer.
What is prostate cancer?
Prostate cancer is a malignant tumor (usually adenocarcinoma) that develops from the tissue of the prostate glands, which, like other malignant tumors, has a tendency to metastasize (spread throughout the body).
At what age and how often does prostate cancer occur?
Before the age of 40-45, prostate cancer is extremely rare. Over the age of 50, an average of 17% of men (one in six to seven) may have prostate cancer. And the older a man gets, the more likely he is to get prostate cancer; component at the age of 70 years – 30-40%.
What are the symptoms of BPH?
For many men, this disease may not have significant symptoms. Adenoma primarily affects the urethra, then the bladder. When it begins to interfere with urination, symptoms of irritation and difficulty appear.
Symptoms of difficulty:
- weak stream;
- difficulty starting to urinate;
- jet intermittency;
- difficulty stopping urination;
- "dripping" after urination;
- feeling of incomplete emptying of the bladder;
- urinary retention, i.e. complete inability to urinate.
Symptoms of irritation:
- frequent urination;
- urgent need to urinate, inability to delay it;
- frequent interruption of night sleep to urinate;
At the onset of the disease, symptoms are mild because the powerful muscles of the bladder are able to increase contractions to push urine out. This compensates for the narrowing of the urethra.
Gradually, the effectiveness of these efforts decreases and tangible difficulties arise. Over time, the muscles of the bladder hypertrophy, that is, they become larger, and muscle tone increases noticeably. Then symptoms of irritation begin to appear. The capacity of the bladder decreases. When the pressure of the prostate on the urethra exceeds the compensatory force of the bladder muscles, it is not possible to completely empty it. This is accompanied by situations requiring treatment.
How is BPH diagnosed?
First of all, you need to consult a specialist doctor - a urologist and tell about the history of your illness and the characteristics of your urination. The examination necessarily includes palpation of the prostate through the rectum, a PSA blood test - this is a special test that suggests the presence of prostate cancer, ultrasound examination of the prostate gland both cutaneously and through the rectum, uroflowmetry - a hardware determination of the characteristics and nature of your urination. After performing these studies, the doctor can make a conclusion about your illness and the need for treatment.
What tests are performed if prostate cancer is suspected?
If prostate cancer is suspected, you may be offered a transrectal ultrasound examination of the prostate (TRUS) and a prostate biopsy.
What should you do if your prostate biopsy does not reveal cancer and your PSA continues to be high?
In this case, you will need a repeat biopsy, usually no earlier than after 3 months. Unfortunately, a prostate biopsy is not able to detect a small tumor in one hundred percent of cases. A repeat biopsy significantly increases the likelihood of detecting an existing tumor.
When should BPH be treated?
BPH requires treatment if symptoms are severe, bothersome, or if urinary tract function is seriously impaired. If you have BPH but your symptoms aren't bothersome, you and your doctor may want to take a watch-and-watch program, in which you get tested one or more times a year to make sure your BPH isn't causing complications.
Treatment
Only a urologist will decide what treatment you need. Treatment of BPH can be conservative, i.e. medication, or through surgery - open surgical or transurethral endoscopic.
Drug treatment of benign prostate hyperplasia (adenoma)
Drug therapy occupies an important place in the treatment of BPH and is based on the results of the latest research into the pathogenesis of the disease and the mechanisms of action of drugs. Currently, there are no clear generally accepted indications for choosing one or another type of medication.
At the stage of examining the patient, it is necessary to answer the following questions:
- Can the patient undergo drug therapy or does he have indications for surgery?
- What is the state of the patient’s cardiovascular system and how great is the risk during surgical treatment?
- does the patient agree to the operation?
- What is the severity of BPH symptoms?
- what is the PSA level and are there any signs of prostate cancer?
The answers to these questions, obtained during a detailed urological examination, make it possible to resolve the question of the possibility and effectiveness of drug therapy.
At the stage of drug treatment, it is important to determine (agreed with patients) the duration of the upcoming drug treatment, this could be:
- long-term (many months, sometimes lifelong) use of medications to reduce symptoms of the disease and improve quality of life.
- a time-limited course of treatment carried out to ensure a better quality of life while preparing the patient for surgical treatment.
1. α-adrenergic receptor blockers.
OMNIK (capsules) is the first original prostate-selective blocker of α1A receptors in the prostate and bladder. The drug is characterized by high safety, is used once a day, the therapeutic effect occurs quickly after taking the first capsule.
Currently, there is an innovative dosage form of Omnic - OMNIK OKAS - these are tablets with controlled release of the active substance. They create a constant therapeutic concentration throughout the day, which provides the patient with a restful sleep and gives more strength for an active day. The dosage form of OKAS has no analogues.
Other α-blockers: Dalfaz, Dalfaz 10 mg CP, Cardura, Setegis.
During treatment, patients experience an increase in the rate of urination, a decrease in the amount of residual urine, and a decrease in the frequency of urination at night - during sleep.
2. 5-α-reductase inhibitors.
- Avodart is used 1 tablet 1 time per day. The effectiveness of Avodart can be assessed no earlier than after 6 months; Avodart is one of the rare drugs that cause the reverse development of BPH and lead to its reduction:
- Proscar.
3. Herbal preparations.
Herbal medicines can be used in urological practice as prophylactic agents in patients with the initial stage of BPH, as an alternative to long-term follow-up.
It is necessary to note the high effectiveness of the combination of Omnic and Avodart - improving the patient’s quality of life and reducing the volume of BPH.
The effectiveness of a particular drug does not always depend on the size of the BPH. You never need to prescribe medicine to yourself, only after examination by a urologist can the patient be prescribed one or another drug, and the dose of the drug is individually selected.
How do you prepare for surgery?
Before surgery, all patients must undergo a comprehensive examination, including not only special urological examinations, but also blood and urine tests, an electrocardiogram, fluorogram, examination by a cardiologist, therapist, anesthesiologist, and often, if necessary, a surgeon, gastroenterologist, neurologist, or psychotherapist. Based on the examination results and examination data, the anesthesiologist determines the type of anesthesia - epidural (“injection in the back”) or general anesthesia.
The evening before the operation, a cleansing enema is performed and the hair below the navel is shaved. From the late evening before the operation, and especially in the morning, you should not eat or drink.
What operations are there to treat prostate adenoma?
The purpose of any operation for prostate adenoma is to remove excess tissue that narrows the lumen of the urethra, preventing normal urination. That is, we are not talking about removing the entire prostate, but only the tissue that compresses the urethra.
There are two main operations for the surgical treatment of prostate adenoma:
- Transurethral resection of the prostate (TUR);
- Adenomectomy.
What is the difference between the operations?
- Transurethral resection of the prostate.
TUR of the prostate (or endoscopic resection of the prostate) is a high-tech intervention. During the operation, the patient lies on his back with his legs spread and bent at the knees. Through the external opening of the urethra, the doctor inserts a special instrument into the bladder - a resectoscope.
All manipulations are performed under visual control. Using a resectoscope, pieces of prostate tissue are removed and coagulation (cauterization) of bleeding vessels is performed.
The resulting tissue is sent for histological examination. At the end of the operation, a catheter is inserted into the bladder through the urethra.
With this type of operation there is no external incision. It should be emphasized that TUR of the prostate is one of the most complex and precious operations in transurethral surgery. The amount of tissue removed during the operation is determined by the urologist performing the operation, and his decision depends on many factors - the size of the adenoma, the severity of the symptoms of the disease, the patient’s age, the presence and identification of concomitant diseases, etc.
- Transvesical adenomectomy.
Adenotomy is an open operation during which an incision is made between the navel and pubis in the skin of the anterior abdominal wall, subcutaneous fat, muscles and the anterior wall of the bladder, after which the doctor removes the prostate adenoma using a finger. A catheter and an additional drainage tube (cystostomy tube) are installed into the bladder through the urethra, which is drained out through the surgical wound.
How does the postoperative period proceed?
Immediately after the operation, you will be installed with a system for continuous lavage of the bladder (with a special solution or furatsilin), the rinsing liquid enters through one of the internal channels of the catheter into the bladder and is released through another channel or cystostomy tube out into the urine bag along with small blood clots. The duration of operation of such a system is determined by the doctor and can range from several hours to 2-3 days.
It is possible that in the near future after the operation you will have the feeling that you really want to urinate - this is due to the presence of a catheter in the bladder, the balloon of which can irritate the neck of the bladder.
1.5-2 hours after the operation, if there is no nausea, you can drink (in small portions; until the evening you are allowed to drink about 200-300 ml of still water). It is better to resume eating the next morning.
After surgery, avoid eating salty, fried, smoked foods, try to drink at least 2000 ml of liquid per day (water, tea, fruit drink, juice, etc.). In any case, it is better to check your diet and fluid intake with your doctor.
Antibacterial therapy usually lasts up to 2-3 months - it depends on the nature of the disease and the characteristics of tissue healing.
After a TUR of the prostate, the urethral cautery is removed after 2-4 days. After adenometomy - after 7-10 days, if the bladder was sutured “tightly”. If during the operation the doctor decided to install an additional drainage tube, then the catheter from the urethra is removed within 2-3 days, and the cystostomy tube - after 15-20 days from the day of the operation.
After removing the catheter, the urine may be light or mixed with blood. You may urinate frequently, in small portions, feel a burning sensation and pain in the urethra and perineum when urinating, and a strong urge to urinate. These phenomena are caused by the surgery and usually disappear within 6-8 weeks. To reduce the severity and duration of discomfort when urinating, taking α-adrenergic receptor blockers helps.
Episodes of the appearance of blood after a TUR of the prostate can persist for up to three weeks, when the patient, as a rule, is already at home. In this case, you should increase the amount of fluid you drink and avoid heavy physical activity, and if you think that the bleeding is threatening, you should immediately contact your doctor or go to the hospital.
A conclusion from a pathologist on the results of a microscopic examination of the tissue removed during surgery can be expected in 7-10 days (depending on where the histological examination is performed). You should definitely find out the histological conclusion and final diagnosis from your attending physician.
Complications after surgery.
Any operation and anesthesia are always associated with a certain risk of complications, including life-threatening ones, which is associated with your illness, age, individual characteristics and possible reactions of the body, which cannot always be foreseen.
Possible complications include:
- Bleeding during surgery or in the immediate postoperative period, which may require a blood transfusion or reoperation;
- With TUR, damage to the bladder wall is possible, which may require open surgery;
- Exacerbation of urinary infection - inflammation of the prostate, testicles, kidneys;
- Development, after 1.5-2 months, of narrowing (stricture) of the urethra;
After the operation, a histological examination of all tissues removed during the operation is required.
Detection of cancer cells among the removed tissue is possible even with a normal PSA value and a negative prostate biopsy.
You must obtain the results of histological analysis from your doctor and, if necessary, continue treatment.
After the operation, no later than 3 months, we recommend undergoing a follow-up examination, including a general urine test, uroflowmetry, ultrasound with determination of residual urine, and a PSA blood test.
Conclusion.
Benign prostate hyperplasia (adenoma), unfortunately, is an inevitable disease for men, but one should not despair and take the disease for granted. Timely regular examinations and a timely diagnosis make it possible, if not to prevent the disease, then to either cure it or, through treatment, provide a man with a decent quality of life.
Forms of BPH
Nodular form of prostate adenoma
- indicates that changes in prostate tissue are presented in the form of nodes.
Diffuse form
- implies that the process is evenly distributed throughout the prostate gland.
Focal prostatic hyperplasia
- may mean that the process is localized in a certain area,
Hyperplasia of the transition zones of the prostate
- indicates a shift in emphasis to the transitional areas of different lobes to the area of the upper urethra.
Antispasmodics and painkillers for exacerbation of the disease
The main purpose of antispasmodic and analgesic drugs during exacerbation of prostate adenoma is to alleviate the general condition of the patient and eliminate pain.
Non-steroidal anti-inflammatory drugs (Diclofenac, Ibuprofen) have an anti-inflammatory and analgesic effect. They help fight not only the pain that occurs during urination, but also the constant pain in the groin and perineum. Thanks to the action of non-steroidal anti-inflammatory drugs, the inflammatory process is reduced, swelling of the prostate gland is reduced, body temperature is normalized, and unpleasant symptoms are eliminated. Non-opioid analgesics, available in the form of tablets or suppositories, help relieve pain during exacerbation of prostate adenoma. The most accessible of them is Analgin. However, this drug is intended rather for one-time use, since it can only affect mild pain. In addition, analgesics with lidocaine, benzocaine, anesthesin and novocaine (Ichthyol, Anestezol, Procto-Glivenol) are effective.
Treatment of prostate adenoma
The essence of treatment for prostate hyperplasia is, on the one hand, to eliminate symptoms that reduce a man’s quality of life (frequent, difficult urination, pain in the lower abdomen and perineum, etc.), on the other hand, to restrain the growth of the prostate and slow down the process of hyperplasia in the early stages of the disease.
In the later stages of the disease, we are talking about partial resection or complete removal of the prostate gland itself, which threatens to completely block the flow of urine from the bladder.
Behavioral therapy
In mild cases with minor manifestations of prostate adenoma, treatment comes down to behavioral therapy , which includes :
- Dynamic observation every six months: regular visits to the urologist
- performing TRUS in dynamics,
- blood sampling for PSA
- passing a general urine test.
- fruits - including melon, watermelon,
The simplest and most effective exercises:
- Kegel exercises: squeezing and unclenching the anal sphincter - as often as possible if possible;
- Voluntary interruption of the act of urination, its resumption after an ever-increasing pause - at every opportunity;
- Half squats - up to 50 times a day;
- Walking “on the buttocks” around the room, both forward and backward, at least 20 passes per day.
What stages of the disease are distinguished for prostate adenoma?
First stage
Unfortunately, only a small percentage of men consult a urologist at the initial stage of the disease. A sluggish stream during urination, especially in the morning, frequent trips to the toilet at night - men perceive this as a natural process of aging and try to “live with it.” Thanks to the great compensatory capabilities of the detrusor (the muscle that is involved in expelling urine from the bladder), the bladder is almost completely emptied. Kidney function is usually not affected.
Second stage
When compensatory capabilities are exhausted, the bladder stops emptying fully. Its wall becomes hypertrophied (thickened), and the formation of diverticula (“bladder hernia”) is possible.
In this case, men experience incomplete emptying of the bladder. The frequency of trips to the toilet increases during the daytime. Often in the morning, patients have to urinate in 2-3 doses. The stream of urine becomes vertical, interrupted by drops, the patient is forced to push, which can lead to the formation of a hernia or prolapse of the rectum. With hypertrophy of the bladder wall, rough folding is formed, which prevents the flow of urine from the upper urinary tract, causing it to stagnate in the ureters and kidneys. Gradually, thinning and atony of the detrusor muscle fibers occurs. The part of the bladder wall free from muscle fibers stretches, forming bags - false diverticula of the bladder. Residual urine is 100-200 ml, and sometimes up to a liter or more. Signs of renal dysfunction develop: dry mouth, increased thirst, etc.
Third stage
The amount of residual urine will increase significantly. The bladder expands greatly. The patient complains of intermittent urination, often in extremely small portions. Severe thickening of the bladder wall deforms the orifices of the ureters, thereby disrupting the adequate outflow of urine from the kidneys. Also, a large volume of residual urine contributes to the development of a focus of chronic infection.
At this stage, there is an extremely high risk of developing acute urinary retention, which requires immediate qualified medical care. After all, the impaired outflow of urine from the body poisons it and can lead to the death of the patient.
Drug therapy
Drug therapy for prostate adenoma is designed to solve several important problems:
- eliminating difficulty urinating,
- decreased frequency of urination,
- reducing the size of the prostate gland and inhibiting its growth.
The therapy is developed by a urologist who weighs all the pros and cons when prescribing each specific drug, otherwise the drugs can only do harm and worsen the condition.
First stage
“First-line therapy” in the treatment of prostate adenoma is alpha-blockers, which eliminate obstruction of the lower urinary tract and improve urination and bladder emptying. They can be taken for life or until the cause of the obstruction is eliminated.
This group includes 5 drugs that have approximately the same effect:
- Tamsuzolin at a dose of 0.4 mg/day is the most popular drug in Russia; the drug does not require dose selection.
- alfazosin – at a dose of 10 mg/day – has a safe profile.
- silodosin - dose 8 mg/day - have greater selectivity in terms of eliminating unpleasant symptoms.
- Terazosin - the dose is increased gradually - from 1 to 10 mg, it can reduce blood pressure, so it is better to take it at night.
- doxazosin - the dose is selected individually from 1 to 8 mg, significantly reduces blood pressure.
Second phase
The next stage of drug therapy for prostate adenoma is the prescription of drugs from the group of 5-alpha reductase inhibitors, the only drugs that can actually reduce the size of the prostate gland (by an average of 30%). These are the two main medications:
- finasteride - 5 mg per day, course 12 months;
- dutasteride – 0.5 mg per day, course 6 months.
When taking these drugs, the condition can significantly improve: signs of compression of the urethra decrease, the risk of surgery and acute urinary retention are reduced.
Some foreign experts recommend prescribing reductase inhibitors as early as possible in order to early prevent the growth of hyperplasia and eliminate undesirable effects, but this issue is under study.
In addition, 5-alpha reductase inhibitors have a very unpleasant side effect - impaired sexual function, so the use of the drug is limited in young patients.
Important! During therapy with finasteride and dutasteride, PSA levels should be monitored.
Combination therapy
To improve the results of treatment of prostate adenoma, combination therapy tactics are used, which affects various pathological links in the pathogenesis of the disease.
The combination of adrenergic blockers and 5-alpha reductase inhibitors is quite effective. This is the optimal therapy for patients at high risk of further development of prostate adenoma.
Another combination has also proven itself well: muscarinic receptor inhibitors in combination with the same adrenergic blockers. This therapy significantly improves the quality of life of patients with concomitant urinary incontinence.
When prostatic hyperplasia is combined with prostatitis, anti-inflammatory drugs and antibiotics are added to the treatment for adenoma, taking into account the current microflora.
Drugs to normalize urination
With frequent, painful urge to urinate, including at night, the issue of prescribing muscarinic receptor blockers, represented by such drugs as:
- solifenacin,
- tolterodine.
Important! You need to know that the use of antimuscarinic drugs is limited in case of large prostate glands and a significant volume of residual urine, since their use can cause the opposite effect and lead to acute urinary retention.
Desmopressin
With a painful urge to urinate at night, more than 5 times a night, a person is practically deprived of sleep. In this case, it is promising to use an analogue of the antidiuretic hormone - the drug desmopressin, which reduces urination.
But this medicine is prescribed very carefully, by a urologist together with a therapist, under the control of sodium levels in the blood.
Drugs to improve erection in prostate adenoma
An interesting question is the use of a drug similar to the famous Viagra - a phosphodiesterase type 5 inhibitor (PDE-5):
- Tadalafil at a dose of 5 mg per day, in addition to improving erection, has a positive effect on the process of emptying the bladder - it eliminates difficulty urinating and prevents inflammation of the prostate gland.
Important! Tadalafil (Cialis) is used exclusively. Viagra has a different active ingredient (siddenafil), which in this case will not have a therapeutic effect. Levitra (vardenafil) is also not used.
Treatment
There are absolute and relative indications for the treatment of prostate adenoma. Absolute indications usually include acute urinary retention, persistent hematuria and urinary tract infections - conditions that, without treatment, sharply worsen the patient's condition. Absolute indications are available only in a small proportion of patients.
Relative indications include prostatism, increased residual urine volume and obstruction. In themselves, these complications do not threaten serious consequences, even if they cause significant inconvenience to the patient. It is necessary to determine how much urinary disorders interfere with normal life and what risks it makes sense to take to alleviate your condition. Treatment recommendations from different doctors vary greatly.
"Ethnoscience
Many patients with prostate adenoma use herbal preparations for therapy. Herbal preparations undoubtedly have some effect, but extensive clinical international studies have not been conducted on them! Therefore, the use of these drugs is of an auxiliary nature. In Russia, products isolated from African palm trees are widely used: Serenoa repens (Prostamol UNO, Permixon), Pigeum Africanum (Pidgeum), Hypoxisrooperi (Hypoxis).
Of the domestic traditional medicines, the following are most often used as additional restorative therapy for prostate adenoma:
- Beekeeping products (honey, bee bread, dead bees, propolis) - inside;
- A decoction of young aspen bark;
- Decoction of fireweed (angustifolia fireweed);
- Red root decoction (Altai endemic - forgotten kopeck) decoction;
- Pumpkin seeds (contain zinc, so necessary for the prostate) up to 50 pieces per day orally;
- Burdock root decoction.
In addition, in Russia, products from animal raw materials are actively used - the prostate of bulls, in suppositories and injections.
Such drugs as Vitaprost, Prostatilen, Prostakor and Samprost. There are only Russian studies on these drugs, and a certain effect occurs, especially with concomitant prostatitis, but, again, there have been no broad international research programs.
Hirudotherapy (leech treatment), which reduces inflammatory edema and improves blood circulation in the prostate area, is of some importance in terms of symptomatic treatment of prostate adenoma. However, such therapy is fraught with bleeding and should be carried out only by qualified specialists.
Important! It should be clearly understood that all of the above remedies have a rather uncertain effect, therefore, if symptoms of prostate adenoma develop, a visit to a urologist is mandatory!
Useless remedies and contraindications
The following have a completely incomprehensible effect: shock wave therapy, Sytin's moods, salt dressings, urine therapy, Thermex, magnetotherapy, microenemas, Vitafon, Almag, hydrogen sulfide baths, phonation, Chinese urological patch, radon baths, various dietary supplements, homeopathy, treatment salt according to the method of Professor Okulov, hydrogen peroxide according to Neumyvakin, beaver stream, indigal, adenorphine and other “exotic” agents.
Important! In case of prostate adenoma, are contraindicated , otherwise this can lead to progression of the disease and even the development of oncology.
Surgery
The purpose of surgery in the late stages of prostate adenoma is to eliminate compression at the level of the prostatic urethra.
Indications for surgical treatment :
- severe compression of the urethra;
- ineffectiveness of taking medications;
- painful symptoms of adenoma (for example, frequent debilitating urge to urinate);
- complications of adenoma (renal failure, urinary stones, blood in the urine, chronic urinary retention).
Indications for emergency hospitalization in a urological hospital :
- Acute urinary retention - manifested by a complete cessation of urine flow from the urethra, bloating of the lower abdomen, and an increase in pain in the bladder area;
- The development of acute renal failure, which is clinically manifested by a sharp decrease in urination, an increase in edema, deterioration of the condition, up to loss of consciousness, an increase in the concentration of potassium, urea, and creatinine in the blood;
- Blood in the urine and the possibility of blockage of the bladder with clots.
Types of surgical interventions
Prostate TOUR
Transurethral resection of the prostate gland.
It is the “gold standard” for surgical treatment of BPH. TUR is the main type of surgical intervention for medium-sized prostate adenoma.
It is used for prostate volume from 30 to 80 cm3.
Performed under general anesthesia or spinal anesthesia, it is a very gentle method of surgical treatment in terms of complications. It involves burning out the prostate tissue that has blocked the lumen of the urethra using a special device using an electric resectoscope.
The average operation time is up to 1 hour. Rehabilitation may require 4 to 6 weeks. In the postoperative period, discomfort may appear during urination, blood in the urine, signs of inflammation, and sexual activity may be delayed.
In the postoperative period, the patient takes tablets: adrenergic blockers and anti-inflammatory drugs, antibiotics.
Open adenomectomy
Removal of the prostate gland. The operation is performed through the bladder, but an operation through the perineum is also possible.
It was first performed more than 100 years ago, but is still used in patients with large prostate sizes greater than 80 cm3.
Open adenectomy is recommended as the standard of care for such adenomas by the European Association of Urology.
Prostate removal is performed under general anesthesia or spinal anesthesia. This type of operation is more traumatic, but the effect is more lasting and there are no relapses. The operation time is more than 1.5 hours, longer than with TUR, the recovery period is up to 3 months.
During the operation, a catheter is inserted into the abdomen to drain urine, which is removed after 2 weeks. Time spent in hospital is 2-3 weeks.
Laparoscopy
Gentle surgical techniques for large prostates are becoming increasingly popular - laparoscopic removal of the prostate gland using special instruments and several small holes in the abdomen. Such operations reduce the operation time and the likelihood of complications.
One of the options for laparoscopic surgery is robot-assisted radical prostatectomy (RARP) using the Da Vinci robot. RARP is actively “displacing” open prostatectomy in the treatment of large prostate adenoma throughout the world.
With RARP, compared with conventional adenomectomy, the volume of blood loss is significantly reduced, and there are advantages in assessing the restoration of urinary continence and erectile function.
Alternative treatments for prostate adenoma :
All these methods have a certain significance and can constitute a worthy alternative to surgical treatment of the prostate gland.
- Stenting of the prostatic part of the urethra with temporary and permanent devices - stents;
- Hyperthermic effects on the prostate gland with temperatures from 40 to 100 degrees;
- Laser technologies: vaporization (evaporation) of the prostate gland with a “green” laser beam,
- laser resection of the prostate,
- laser coagulation,
- holmium enucleation HoLAP - a variant of evaporation of the affected prostate gland with two different laser radiations, developed by New Zealand urologists;
Despite their good effectiveness, alternative methods of treating prostate adenoma are quite expensive, are not included in the compulsory medical insurance system, and there are few clinics performing these methods in Russia.
Advantages of contacting MEDSI
- Experienced doctors.
Our specialists have been involved in the diagnosis and treatment of prostate pathologies for a long time. They have the necessary knowledge and skills to carry out a wide range of manipulations - Possibilities for quick diagnostics.
Our specialists use expert-class equipment. It allows you to make a diagnosis on the day of treatment - Individual approach to therapy.
Treatment of prostatitis and prostate adenoma is provided taking into account the type and stage of the disease, the characteristics of the patient, as well as his existing concomitant diseases - Conservative therapy using modern techniques
- Modern methods of surgical treatment.
At MEDSI, surgical interventions are performed using a laser and a da Vinci robot. Laparoscopic operations and TUR (transurethral resection) are performed. This allows you to reduce the risks of interventions and the duration of the rehabilitation period - Comfort of visiting clinics.
They are located near the metro. In addition, we have made sure there are no queues and are ready to receive patients at a time convenient for them.
To undergo treatment for prostate adenoma or prostatitis and find out the difference between these diseases, we advise you to make an appointment with a doctor at the MEDSI clinic by calling (495) 7-800-500. Our specialist will answer all questions. Recording is also possible through the SmartMed application.
Specialized centers
- Standards of the International Association of Urology
- High-precision diagnostics using cutting-edge equipment
- Modern high-tech operating rooms and hospitals
More details
What happens if BPH is left untreated?
If the symptoms of prostate adenoma are ignored or self-medication, which, as a rule, is incorrect in 99% of cases, the following processes can be added to prostatic hyperplasia, in addition to aggravating the disease itself:
- sleep disturbances, mental disorders;
- erectile dysfunction (impaired erection and potency);
- “neurogenic bladder” - uncontrollable frequent urination;
- acute urinary retention is the most serious complication when a sharply enlarged prostate gland completely blocks the lumen of the urinary tract. This is an emergency. If medical care is not provided in a timely manner (emergency urine drainage by catheterization of the bladder through the anterior abdominal wall - cystostomy), uremic coma develops;
- pyelonephritis (inflammation of the kidneys as a result of infection ascending to the upper urinary tract);
- prostatitis (inflammation of the prostate);
- urethritis (inflammation of the urethra);
- urolithiasis (formation of stones in the kidneys and bladder);
- Hematuria (the presence of blood in the urine) occurs quite rarely with edestate adenoma, in cases of damage to significant muscle layers of the prostate by adenomatous nodes. Basically, this is a characteristic symptom of prostate cancer and urolithiasis;
- to some extent, an adenoma can cause infertility, because leads to a decrease in the secretion of the prostate gland, which is the environment for the existence of sperm.