Pneumosclerosis is a lung disease that is characterized by the replacement of normal lung tissue with connective tissue. The process is the result of an inflammatory process and degeneration of organ tissue, as a result of which there is a violation of elasticity and gas transport in the affected areas.
- Causes
- Pathogenesis
- Classification of pneumosclerosis
- Symptoms
- Consequences of pneumosclerosis
- Diagnostics
- Treatment
The extracellular matrix grows in the respiratory organs, deforms the branches of the windpipe, and the lung itself shrinks and becomes denser. The lungs lose air and become smaller. The disease is equally common in the population of all ages. Men get sick more often than women.
Pneumosclerosis is divided according to the severity of connective tissue proliferation into:
- fibrosis
- sclerosis
- pulmonary cirrhosis
If pneumosclerosis manifests itself in the form of fibrosis, then cicatricial changes in the organ are moderately pronounced. In the second form, there is a more severe replacement of the lungs with connective tissue. In cirrhosis, the third form, the alveoli are completely replaced, and the bronchi and blood vessels are also partially replaced by disorganized connective tissue. Pneumosclerosis is not only an independent nosological form, but the outcome of other diseases, as well as a symptom.
Causes
Pneumosclerosis quite often accompanies the diseases listed below or is formed as a result of them:
- chronic bronchitis, chronic obstructive pulmonary diseases, inflammation of the tissue surrounding the bronchi
- diseases provoked by foreign substances in the lungs, infectious in nature, viral pneumonia, mycoses, tuberculous processes in the organ
- allergic and fibrosing alveolitis
- pneumoconicosis, the cause of which is prolonged inhalation of gases and dust, industrial and radiation pneumoconicosis
- genetically transmitted lung diseases
- lung injuries, wound consequences
- Beck's disease in pulmonary form
If acute and chronic processes in the respiratory organs were ineffectively treated or a sufficient course of treatment was not followed, this creates the ground for the development of pneumosclerosis.
Among the provoking factors of the disease in question:
- LV heart failure
- pulmonary circulation defects due to narrowing of the left atrioventricular orifice
- pulmonary thrombosis
- taking toxic pneumotropic drugs
- influence of ionizing radiation on the body
- weakening of general and local immunity
If the pulmonary inflammatory process is not completely resolved, then the inflammation of the lung tissue is also incomplete, connective tissue scars grow, alveolar lumens narrow, which leads to pneumosclerosis. It is noted that the disease often occurs in those who have suffered staphylococcal pneumonia, which was accompanied by the formation of necrotic areas of lung tissue and an abscess. After the abscess healed, fibrous tissue began to grow.
If the disease in question is a consequence of pulmonary tuberculosis, then connective tissue may appear in the organ, which leads to the development of peri-scar emphysema. A complication of chronic inflammation in the bronchi, such as bronchitis and bronchiolitis, is the occurrence of perilobular and peribronchial pneumosclerosis. Pleurogenic pneumosclerosis can begin after repeated inflammation of the pleura, in which the superficial layers of the lung join the inflammatory process, its parenchyma is compressed by exudate.
Radiation and Hamman-Rich syndrome in frequent cases are provoking factors for the development of pulmonary sclerosis of diffuse origin. A lung is formed that looks like a shoulder honeycomb. Mitral valve stenosis and left heart failure can cause fluid to leak from blood vessels, leading to cardiogenic pneumosclerosis. P. can be caused by bronchial, vascular, or pulmonary pathologies when the flow of lymph and blood is disrupted.
Other causes of pathology include:
- chronic bronchitis accompanied by peribronchitis
- chronic pneumonia, untreated acute pneumonia, bronchiectasis
- congestion in the lungs in some heart diseases, mainly with mitral valve defects
- pneumoconiosis of various origins
- prolonged and severe exudative pleurisy
- pulmonary atelectasis
- tuberculosis of the lungs and pleura
- traumatic injury to the chest and lungs
- systemic connective tissue diseases
- treatment with drugs such as apressin or cordarone
- effects of chemical warfare agents on the lungs
- effects of ionizing radiation on the human body
- idiopathic fibrosing alveolitis
Treatment
Photo: sanatoriy-kirova.ru
To prevent the development of pneumosclerosis, you should promptly treat respiratory diseases, take precautions when interacting with pneumotoxic substances, and do not delay going to the doctor if characteristic symptoms occur. When working in hazardous industries, it is important to use respirators that prevent dust and chemicals from entering the respiratory tract. In addition, the immediate production management must take care of the proper operation of exhaust ventilation.
When diagnosing pneumosclerosis, treatment begins with lifestyle changes. First of all, it is recommended to stop smoking, as cigarettes can aggravate bronchial obstruction. All family members must understand that there is a concept of passive smoking, so it is important not only for the patient himself to forget about cigarettes, but also for the people living in the same living area. Meals should be fractional, complete, sufficiently filled with vitamins and microelements. Despite the fact that pneumosclerosis is accompanied by shortness of breath, especially when playing sports, you should not completely give up physical exercise. It is necessary to arrange long distance walks and perform therapeutic exercises.
Considering that with pneumosclerosis, the lungs cannot fully provide the body with the necessary amount of oxygen, oxygen therapy is used. This treatment helps saturate the blood plasma with oxygen, which leads to a decrease in the severity of shortness of breath. However, safety rules should be observed, since frequent or excessive use of pure oxygen or inhalation mixtures with high oxygen concentrations can lead to oxygen intoxication.
For the symptomatic treatment of cough, expectorants are used to promote the separation of sputum. For the same purpose, mucolytic agents are prescribed, which dilute sputum, thereby facilitating its removal.
Pathogenesis
The development of the disease in pathogenetic terms depends very much on the causes (provoking factor). But still, in the pathogenesis of any form of pneumosclerosis, disruption of pulmonary ventilation, drainage function of the bronchi, blood and lymph circulation is important. The proliferation of connective tissue causes disruption of the structure and destruction of specialized morphofunctional elements of the lung parenchyma. Blood and lymph circulation disturbances that occur during pathological processes in the bronchopulmonary and vascular systems contribute to the development of pneumosclerosis.
Pneumosclerosis, according to the characteristics of its pathogenesis, is divided into diffuse and focal (or local). And focal can be large- and small-focal.
The use of exercise therapy and physiotherapy
Physiotherapeutic procedures play a significant role in this disease. They are aimed at stopping the inactive form of pneumosclerosis. If there is no significant pulmonary insufficiency, iontophoresis with calcium chloride or Novocaine is used. The Warmel system is used for slow sputum production.
Physical therapy is prescribed to all patients without exception. It is aimed at strengthening the respiratory system. With a compensated form of the disease, breathing exercises are prescribed. Exercises are performed at a slow pace.
Classification of pneumosclerosis
Classification according to the degree of replacement of lung tissue with Pischinger's space:
- fibrosis with alternation of limited affected areas in the form of cords with healthy air-filled tissue
- pneumosclerosis itself (connective tissue replaces pulmonary tissue, tissues of a denser consistency than normal lung tissue are noted)
- complete replacement of pulmonary connective tissue, compaction of the alveoli and pleura, as well as blood vessels; displacement of the mediastinal organs to the affected side. This is the stage of cirrhosis.
There is a special form of focal pneumosclerosis - carnification, in which the pulmonary parenchyma in the inflamed area resembles raw meat in consistency and appearance. Microscopically, areas of fibrinous exudate, sclerosis and suppuration, fibroatelectasis, etc. are detected. Limited pneumosclerosis differs from diffuse pneumosclerosis in that gas exchange does not deteriorate, the lung is as elastic as before the disease. In the diffuse form, ventilation is reduced and the affected lung is rigid.
Pneumosclerosis, based on the predominance of affected structures, is divided into the following forms:
- peribronchial
- alveolar
- perilobular
- interstitial
- perivascular
Classification according to the reasons for the formation of the disease:
- postnecrotic
- discirculatory
- dystrophic
- post-inflammatory
Innovative techniques
A modern method of therapy is the use of stem cells. This allows the structure of the organ to be completely restored and its functioning to be normalized. Stem cells can transform into cells of any tissue. But the procedure is expensive, since it is very difficult to obtain the material.
Stem cells are injected into the patient's body intravenously. They move with the blood to the affected organ, where they replace tissue. Over time, the lungs acquire normal size, and their original elasticity and firmness return. At the same time, the functioning of the heart muscle and nervous system is normalized, the immune system is strengthened, and hormonal levels become balanced.
Another new technique that does not promote tissue regeneration, but is aimed at improving metabolism in cells, is oxygen therapy. The essence of the procedure is that the body is saturated with oxygen using special masks, tubes and catheters.
Symptoms
Signs of the underlying disease causing pneumosclerosis:
- chronic pneumonia
- Chronical bronchitis
- bronchiectasis
Dyspnea with diffuse pneumosclerosis, which at the beginning of the disease is observed only during exertion, but then appears when the person is at rest. A productive cough is characterized by the production of mucopurulent sputum. Severe diffuse cyanosis is typical.
Auscultatory and percussion signs:
- shortening of percussion sound
- limited mobility of the pulmonary edge
- fine wheezing
- weakened vesicular breathing with a hard tint
- dry scattered wheezing
Along with the symptoms of pneumosclerosis, the clinic of emphysema and chronic bronchitis often appears. Diffuse forms of pneumosclerosis are accompanied by precapillary hypertension of the pulmonary circulation and manifestations of cor pulmonale.
The following symptoms indicate lung cirrhosis::
- partial atrophy of the pectoral muscles
- severe deformation of the chest
- tracheal displacement
- shrinkage of intercostal spaces
- displacement of large vessels and heart to the affected side
- sudden decrease in breathing
- dull sound when percussing
- dry and moist rales detected by auscultation
With a limited form of pneumosclerosis, the patient does not complain of anything. Only a slight cough with minimal phlegm may bother you. When examining the affected side, it is discovered that the thorax in this place has a kind of depression.
Pneumosclerosis of diffuse origin has a symptom such as shortness of breath. At later stages it is present, even if the person is not taking any action at the moment (sitting or lying). The alveolar tissue is poorly ventilated, which is why the skin has a bluish tint. The Hippocrates finger sign is recorded, which indicates increasing respiratory failure. The patient complains of cough. At first it appears rarely, but then it becomes intrusive, purulent sputum is released. The course of pneumosclerosis aggravates the underlying disease.
In some cases, aching pain in the thoracic area is noted, patients may lose weight, look weakened, and causeless fatigue is likely. Symptoms of pulmonary cirrhosis may develop:
- atrophy of intercostal muscles
- gross deformity of the thorax
- displacement of the throat, large vessels and heart to the affected side
With diffuse pneumosclerosis, the cause of which is a violation of the hemodynamics of the small bloodstream, clinical symptoms of cor pulmonale sometimes appear. The severity of any form of pneumosclerosis correlates with the size of the affected areas.
Stages of the disease:
- compensated
- subcompensated
- decompensated
Emphysema and pneumosclerosis
A sign of pulmonary emphysema is the accumulation of increased amounts of air in the lung tissues. Pneumosclerosis, which is the result of chronic pneumonia, has very similar symptoms. The development of emphysema and pneumosclerosis is affected by infection of the bronchial wall, the influence of inflammation of the branches of the windpipe, and obstructions to the patency of the bronchi. Sputum accumulates in the small bronchi. Ventilation in this area of the lung can cause emphysema or pneumosclerosis. Diseases that are accompanied by bronchospasm, for example, bronchial asthma, can accelerate the development of these diseases.
Hilar pneumosclerosis
Connective tissue can grow in the hilar regions of the lung, then hilar pneumosclerosis is diagnosed. It is preceded by processes of inflammation or dystrophy, when the elasticity of the affected area is lost and gas exchange disturbances occur in it.
Local pneumosclerosis
Local pneumosclerosis, as already indicated, can be called limited by some authors. Symptomatically, it can be hidden for a long period, but upon auscultation, hard breathing and fine rales can be heard. It is detected by x-ray methods. The image shows an area of compacted lung tissue. Local pneumosclerosis may not cause pulmonary failure.
Focal pneumosclerosis
Focal pneumosclerosis can be a consequence of the destruction of the lung parenchyma, and the cause of the latter, in turn, is a lung abscess or cavities. The proliferation of connective tissue can be observed both at the site of existing and at the site of healed cavities and lesions.
Apical pneumosclerosis
In the apex of the lung in the apical form of the disease there is a lesion. As is typical for pneumosclerosis, the lung tissue at the apex is replaced by connective tissue. At first, the process is similar to bronchitis, and most often bronchitis precedes and becomes the cause of apical pneumosclerosis. It can be detected by x-ray.
Age-related pneumosclerosis
Age-related pneumosclerosis becomes the result of changes associated with the aging process of the human body. This form, as the name implies, develops only in elderly people if they have congestive phenomena due to pulmonary hypertension. The disease mainly affects men; smokers are at increased risk. If an x-ray reveals pneumosclerosis in an 80-year-old (or older) person, but the patient has no complaints, this is the norm.
Reticular pneumosclerosis
As the amount of connective reticular tissue increases, the lungs become less clean and clear, and the tissue acquires a mesh-like structure resembling a spider's web. For this reason, the normal pattern is almost not visible; it looks weakened. CT scan clearly shows compaction of connective tissue.
Basal pneumosclerosis
When connective tissue begins to grow in the basal parts of the lung, then pneumosclerosis is classified as basal. It is often preceded by lower lobe pneumonia. The radiograph shows increased clarity of the lung tissue in the basal regions, enhancing the pattern.
Moderate pneumosclerosis
At the onset of the disease, the proliferation of connective tissue replacing the pulmonary tissue is moderate. Changed lung tissue alternates with healthy parenchyma. An x-ray reveals this picture, but the patient has no complaints, nothing bothers him.
Postpneumonic pneumosclerosis
This form of the disease is a complication of pneumonia. The inflamed area looks like raw meat. Macroscopically, the affected area is more compacted; this area of the lung is smaller in size than normal.
Interstitial pneumosclerosis
In this form, the connective tissue mainly covers the interalveolar septa, tissues, surrounding vessels and bronchi. Interstitial pneumosclerosis is a consequence of interstitial pneumonia.
Peribronchial pneumosclerosis
Connective tissue grows, surrounding the bronchi. The cause of this form of pneumosclerosis is the transfer of bronchitis in a chronic form. For a long period of time, the patient does not feel any changes in the body; he may only be slightly bothered by a cough. Over time, sputum appears.
Post-tuberculosis pneumosclerosis
In post-tuberculosis pneumosclerosis, the proliferation of connective tissue occurs after recovery from pulmonary tuberculosis. This condition can develop into “post-tuberculosis disease,” in which there may be different nosological forms of nonspecific diseases, for example, COLD.
Folk remedies
Photo: s3-ap-southeast-1.amazonaws
It should be understood that pneumosclerosis is an irreversible process, therefore it is impossible to completely cure it, but you can improve your overall well-being. To improve the function of external respiration and strengthen the body, physical therapy exercises are recommended. Classes should be conducted in the morning, duration is 20 – 40 minutes. Particular attention should be paid to breathing exercises that train the inhalation and exhalation phases. General strengthening exercises are performed with the involvement of various muscle groups participating in the exercises alternately. The pace of classes should be slow with a gradual increase to medium; a fast pace is contraindicated. Physical therapy begins with a minimum load and gradually increases to the maximum tolerated. Patients with pneumosclerosis get tired faster than healthy people, so they independently indicate the maximum tolerated load, referring to subjective sensations.
To reduce the severity of shortness of breath and cough, there are various traditional medicine recipes. In the fight against shortness of breath, tea made from reeds (brooms) has proven itself well. To prepare it you will need 1 glass of crushed raw materials, which is poured with 1 liter of boiling water. After steeping, the tea is ready to drink. It is recommended to take 1 glass three times a day. The course is at least 3 weeks.
There is a recipe for a tincture based on honey, lemon and garlic. To prepare, you will need 1 liter of liquid honey, 10 lemons and 10 heads of garlic. Honey should be mixed with peeled and minced garlic, add lemon juice. This mixture must be thoroughly mixed, closed in a jar and allowed to brew in a dark place for 1 week. Take 4 teaspoons per day once. A special feature of the application is the fact that the mixture should not be swallowed immediately, it should be kept in the mouth, slowly dissolving. The full course of use is 2 months; after a break, you can repeat the dose if necessary.
The most popular folk recipe for cough is a glass of warm milk with honey. You can drink this drink during the day at any time convenient for you; it is especially recommended to take it at night so that coughing attacks do not disturb your sleep.
There is another assistant that alleviates the general condition and eliminates cough. To prepare it, you need to boil 1 lemon for 10 minutes, after which it should be cut in half, squeeze out the juice and combine with 2 tablespoons of glycerin. Next, honey is added in such an amount that the glass is filled almost to the top. The resulting syrup is used 1 teaspoon several times a day.
The information is for reference only and is not a guide to action. Do not self-medicate. At the first symptoms of the disease, consult a doctor.
Consequences of pneumosclerosis
With this disease, the alveoli, bronchi and blood vessels of the lungs change morphologically, therefore among the complications of the lungs the following are likely:
- reduction of the vascular bed
- impaired ventilation
- chronic respiratory failure
- arterial hypoxemia
- addition of pulmonary emphysema
- association with inflammatory lung diseases
- cor pulmonale
Medicines
There are no special medications developed for the treatment of basal pulmonary pneumosclerosis. Drug therapy is aimed at eliminating the disease that caused the pathological changes. Most often, the following groups of drugs are used in treatment:
- antibiotics;
- cardiac glycosides (Digoxin, Isoniazid, Strophanthin);
- mucolytic drugs (“Lazolvan”, “Erespal”, “Acc”, “Ascoril” and others);
- glucocorticoids;
- angioprotectors (to improve blood supply);
- hormones (to stop the inflammatory process);
- syrups and tablets with expectorant properties;
- detoxification drugs ("Penicillamine")
- anti-inflammatory drugs.
Vitamin therapy is an obligatory component of drug treatment. It is necessary to strengthen the immune system and improve the functioning of internal organs, improve the general condition of the body. For a patient with basal pneumosclerosis, vitamins A, C, E, and group B will be useful.
Patients are often prescribed physical therapy. The most popular in the treatment of the disease in question are electrophoresis and ultrasound with novocaine. Such techniques can be used only in the absence of pulmonary insufficiency, otherwise severe complications will arise. Positive dynamics at almost any stage of the disease can be achieved using inductothermy, electrophoresis with iodine, and ultrasound irradiation.
Diagnostics
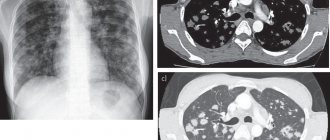
The X-ray picture is polymorphic, because it shows manifestations not only of pneumosclerosis itself, but also of associated diseases: emphysema, bronchiectasis, chronic bronchitis, etc. Typical looping, enhancement and deformation of the pulmonary pattern along the bronchial branches, as the bronchial walls become denser, sclerosis and infiltration of peribronchial tissue occur.
Bronchography shows deviation or convergence of the bronchi, narrowing and absence of small bronchi, and deformation of the walls. Spirography is an effective diagnostic method for suspected pneumosclerosis; it reveals a decrease in VC, FVC, and Tiffno index.
Over the affected area, physical examinations reveal decreased breathing, dry or moist rales, and dullness of percussion sound. Lung examination is also a reliable diagnostic method. Even if there are no symptoms, x-rays help to detect changes if they are present, their nature, prevalence, and how pronounced they are. Magnetic resonance imaging, bronchography, and CT scan of the lungs can more accurately assess the condition of unhealthy areas of lung tissue.
An x-ray shows the following changes in the affected lung:
- reducing it in size
- increased pulmonary pattern along the branches of the bronchi
- the pulmonary pattern is reticulated and looped due to deformation of the bronchial walls
- "honeycomb lung" in the lower sections
Fluorography for pneumosclerosis
If you have any complaints of cough or any respiratory symptoms, you must undergo a fluorographic examination of the chest organs. Every year, in order to prevent and early detect pneumosclerosis, tuberculosis and other similar diseases, all persons over 14 years of age must undergo a medical examination. With pneumosclerosis, the vital capacity of the lungs decreases, and the Tiffno index (which is an indicator of bronchial patency) is low.
Medicines
Photo: proizjogu.ru
Medicines are not able to relieve the patient of pneumosclerosis; they only alleviate the symptoms of the disease. Cough with pneumosclerosis is unproductive; to correct this, expectorants and mucolytics are prescribed. Ambroxol is the most common drug due to its low cost and sufficient effectiveness. The drug achieves its effect by stimulating the glands of the bronchial mucosa. This increases the content of the mucous component of sputum, which facilitates its release. The drug is well tolerated, side effects are extremely rare. For example, in case of individual intolerance to the components of the drug, an allergic reaction develops, which can manifest itself as urticaria or angioedema. Other side effects observed less frequently are: nausea, vomiting, diarrhea, abdominal pain, headaches, general weakness.
Bromhexine is another drug that is used to thin phlegm. Not for use in children under 3 years of age and pregnant women (1st trimester). In all other cases, there are no strict contraindications to the use of the drug. People who have an allergic reaction to the active substance, bromhexine hydrochloride, should be treated with caution. Such people should notify their doctor in advance about the presence of an allergy to a previous drug intake, so that the doctor can select another drug with the desired effect.
Disease prevention
There are several methods of prevention: primary preventive measures are aimed at preventing the development of pneumosclerosis, and secondary ones are aimed at preventing the worsening of the disease and the development of relapses when the disease is put into stable remission.
Preventive methods are mainly aimed at the formation of nonspecific immunity. It is recommended to consume sufficient amounts of proteins, carbohydrates and fats, think through your diet, provide walks in the fresh air and other ways to strengthen the immune system.
It is equally important to undergo an annual fluorographic or x-ray examination in a timely manner. These techniques make it possible to suspect the development of pneumosclerosis in the early stages, as well as monitor the effectiveness of treatment.
To prevent the spread of this lung pathology, it is important to strictly adhere to the regimen of taking medications prescribed by a pulmonologist for treatment.