An antibiotic (antibacterial drug, antimicrobial agent) is a drug that is effective in treating bacterial infections. Its effect is to directly affect the bacterium, it kills it. Its effect may also be to slow down the proliferation of bacteria, which allows the immune system to cope with it. The high prevalence of infections, a large selection of antibiotics for children, and the unjustified prescription of these drugs for diseases in children and adults have led to threatening consequences for human life—antibiotic resistance. According to the Eurasian recommendations, 25,000 deaths annually in the EU are associated with antibiotic resistance. At the moment, antimicrobial agents are an irreplaceable resource for humanity. Antibacterial resistance can be considered a threat to national security.
Before moving on to the choice of a children's antibiotic, consideration of dosage, duration of use, it is necessary to analyze and explain the main points in the formation of resistance to antibacterial agents. Only after this can one adequately judge the choice and approach to prescribing these medications.
Antibiotic resistance
Antibiotic resistance is the term for resistance to antibiotics. Who is to blame for this? The main reason is the excessive and uncontrolled use of antimicrobial agents. This applies not only to medicine.
Prescribing antibiotics should always be justified.
Causes
- Application in medicine. Unjustified prescription on an outpatient basis, in a hospital, self-medication (over-the-counter). The main emphasis is on counteracting the unjustified prescription of antibiotics in primary care (at the outpatient stage). For this purpose, clinical recommendations and algorithms for prescribing antibiotics to children are specially developed and implemented in practical healthcare. Also, through the media, explanations are provided to the population about the need for the judicious use of antimicrobial agents and the dangers of their independent use.
- Use of antibiotics in veterinary medicine.
- Application in the agricultural industry.
Basic rules for the correct use of antibacterial drugs
- An antimicrobial agent is taken only in the presence of a bacterial infection that is suspected or documented.
- When using the drug, you must adhere to the optimal regimen. The first is the correct choice of medicine. Otherwise, it is necessary to maintain an adequate dose and duration of use.
- When choosing a drug, it is necessary to take into account the regional situation regarding antibiotic resistance of the most common pathogens and take into account the likelihood of infection of the patient with these bacteria.
- Do not use low quality antibiotics with unproven effectiveness.
- Do not use antibiotics for prophylactic purposes.
- The effect of using an antibacterial agent is assessed 48-72 hours after the start of treatment.
- Explain the harm of non-compliance with the medication regimen, and also explain the dangers of self-medication.
- Promote the correct use of the drug by the patient.
- In each case, it is necessary to use methods to determine the cause of the infection.
- When prescribing an antibacterial drug, doctors must adhere to recommendations based on evidence-based medicine.
Symptoms
The main signs of the disease, regardless of the type of infection, are constant diarrhea. It is significantly different from the usual disorder. The stool is copious, liquid, and may contain blood and mucus. The urge is very frequent and does not bring relief.
Other symptoms may include:
- muscle weakness;
- increased body temperature;
- cutting pain in the abdomen;
- lack of appetite;
- nausea;
- rumbling in the stomach.
In half of the cases, frequent vomiting, problems with urination, and dehydration are also observed. If the disease is mild, then these symptoms may not be observed, but in an aggravated situation, the symptoms may become more pronounced.
Indications for antibiotics
A fairly common mistake is the use of antibiotics for diseases that develop as a result of a non-bacterial infection.
Antibiotics should not be used for viral infections.
Among these diseases:
- Acute pharyngitis.
- Acute laryngotracheitis.
- Rhinitis.
- SARS, only.
- Acute bronchitis. It is permissible to use antibiotics when bronchial constriction develops, as well as when fever lasts more than 5 days.
In these cases, the prescription of antibiotics is not justified, since the cause that led to these diseases is often viruses.
There are also controversial points when both viruses and bacteria can lead to the development of the disease. Such diseases include:
- Acute rhinosinusitis.
- Acute otitis media.
- Acute tonsillitis.
In such cases, an antibiotic is prescribed only after examination and observation by a doctor of the patient.
For viral infections (pharyngitis, rhinitis, laryngitis, tracheitis), the effectiveness of antibiotics is equal to the placebo effect. It is important to remember that the prescription of antibacterial agents does not prevent the development of bacterial superinfection (that is, the addition of a bacterial infection to an existing viral one). There are no effective remedies against ARVI. The use of antiviral immunostimulating agents common in pharmacy chains often does not have any effect. In this case, the antiviral agent can be considered as ascorbic acid or garlic. In such cases, adequate pathogenetic and symptomatic treatment is prescribed, which allows eliminating and eliminating the symptoms of ARVI. Used: paracetamol, ibuprofen, mucolytics (ambroxol, acetylcysteine, carbocysteine), vasoconstrictor nasal drops for a runny nose, nasal corticosteroid for rhinosinusitis. If there is a disease with a viral or bacterial cause (tonsillitis, sinusitis, otitis media), then in this case antibacterial therapy delayed by 2-3 days is recommended. Delayed antibiotic prescribing for upper respiratory tract infections has reduced the frequency of antibiotic prescriptions by 40%.
These statements are of an evidentiary nature and are described in more detail in the training manual “ Rational use of antimicrobial agents in the outpatient practice of doctors , written on the basis and evidence base of the 2021 Eurasian recommendations.
Types of intestinal infections
Pathologies differ in localization in the gastrointestinal tract and the severity of the course. The mucous membrane of the stomach may become inflamed, digestion processes may be disrupted, and a person’s general well-being may deteriorate. Almost 90% of infections disappear on their own, meaning there is no need to take medications. But this is only possible with a sufficient amount of salts and water in the body. Otherwise, even a mild form of the disease can lead to serious consequences.
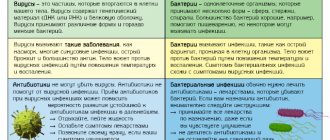
Viral infections
When a viral infection occurs, the walls of the stomach, intestines, and respiratory organs are affected; in rare cases, other organs may be affected. The infection can be transmitted in several ways: fecal-oral, airborne, contact-household.
Viral diseases mainly appear in autumn and winter. It takes about a week to recover. But for the next 3-4 weeks the person is a carrier of the virus and others can become infected from him.
It is especially important for the patient to adhere to a strict diet, drink as much fluid as possible and take appropriate medications against the virus.
Bacterial infections
These diseases are considered much more serious than viral ones, since there is a high probability of severe complications. You can become infected through fecal-oral and household contact. The infection affects the gastrointestinal tract and urinary tract. Dangerous are toxic substances that are formed as a result of the spread and destruction of bacteria. When a huge number of bacteria die, a lot of poison enters the body, which can result in toxic shock or even death.
The patient will need complex treatment. It is necessary not only to get rid of harmful microorganisms, but also to cleanse the body of toxic substances, as well as eliminate symptoms. All this together will make the patient feel much easier. In such cases, antibiotics are usually prescribed.
Bacteria can adapt to antibiotics over time if they are not taken as directed.
Protozoal infections
Compared to the infections described above, protozoal infections are considered less common, but very dangerous. They are transmitted not only through fecal-oral and household contact, but also during sexual intercourse. Despite the active spread in the stomach and intestines, the disease may not make itself felt for a long time, which will complicate the treatment process in the future.
The main types of antibiotics and their common representatives on the market
Below we consider the most popular and frequently used groups of antibacterial agents:
- Beta-lactams . Among them are penicillins, cephalosporins, and carbapenems. Among the penicillins, it is worth highlighting: amoxicillin, ampicillin, ticarcillin, carbenicillin, mezlocillin, mecillam. The most popular cephalosporins are: cefazolin, cephalexin, cefuroxime, cefotaxime, ceftriaxone, cefepime, ceftobiprole. Carbapenems are used much less frequently. Meropenem can be isolated.
- Macrolides . Macrolides include: clarithromycin, azithromycin (sumamed), josamycin.
- Tetracyclines . The most common: tetracycline, doxycycline, oxytetracycline.
- Aminoglycosides . Popular ones: gentamicin, amikacin, isepamycin.
- Levomycetins . Trade names: chloramphenicol, chloromycetin.
- Glycopeptide antibiotics . The most commonly used: vancomycin, bleomycin.
- Lincosamides . Used in medicine: lincomycin, clindamycin.
- Fluoroquinolones . Among them, the most commonly used are: ciprofloxacin, levofloxacin, gemifloxacin. They are a broad-spectrum antibiotic for children. These antibiotics are not contraindicated in pediatric practice, but their use in children is sharply limited.
It is important to remember that these drugs have their own indications and contraindications, and are also used against certain infections.
These drugs have their own indications and contraindications, and have a narrow or broad spectrum of activity against bacteria. Some of the listed drugs can be used by children under one year of age. Children's antibiotics are available in tablets, suspensions, and ampoules for intravenous and intramuscular administration. Calculation of the dose, dilution of antibiotics and administration of the required dose to the child should be carried out by medical personnel in order to avoid unwanted reactions, as well as complications during injections. They should be prescribed exclusively by a doctor.
Indications for use
Antibiotics are prescribed to treat infectious diseases caused by microorganisms sensitive to this antibiotic. A characteristic feature of infectious diseases, in contrast to non-infectious ones, is contagiousness - the ability to be transmitted from person to person and not only. Not all bacteria have the same sensitivity to a particular antibiotic.
In order to choose the right drug, a test is carried out to determine the sensitivity of the pathogen to this drug. In many cases, when it is impossible to identify the causative agent of the disease or there is no time for this, antibiotics are prescribed empirically, using broad-spectrum drugs, hoping to capture as wide a range of potential causative agents of the infectious disease as possible.
Duration of use of antibacterial agents
Parents often ask questions: “How many days are antibiotics given to children? What is the best antibiotic for children? What should I give my child when taking antibiotics? In most cases, 5-7 days of use are sufficient. There are exceptions in which the duration of use may increase to 10–28 days. The second question cannot be answered unambiguously. Each drug has its own indications and contraindications, so the use of a particular drug depends on the situation (age, diagnosis, concomitant pathology, etc.). To the third question, many doctors will answer the same: “Probiotics.” A probiotic will restore normal intestinal microflora that has been affected by an antibacterial agent. As a rule, they are prescribed in a course of 2 weeks to 1 month.
You can always consult your doctor if you have any questions regarding treatment.
According to the Eurasian recommendations, in order to overcome antibiotic resistance, experts emphasize the need to draw the attention of patients to strict adherence to the drug use regimen. It is necessary to use optimal dosage forms of antibiotics with high bioavailability, in particular, Solutab dispersible tablets, which is consistent with the current position of WHO and UNICEF. Advantages of Solutab dispersible tablets:
- Completely absorbed in the intestines. As a result, the effect is equal to the intravenous effect.
- Create a high concentration at the site of infection.
- Better portability.
- Good organoleptic properties.
- The ability to dissolve tablets, which allows the use of this dosage form in children.
- A minimal amount of liquid is required for swallowing.
- They have an advantage over a suspension - errors in preparation are eliminated.
Dispersible tablets recommended by WHO and UNICEF:
- Flemoxin Solutab
- Flemoklav Solutab
- Suprax Solutab
- Vilprofen Solutab
- Unidox Solutab
Parents of children should remember that an incomplete course of prescribed antibiotic treatment leads to the formation of bacterial resistance and a prolonged presence of the microbe in the body.
Rational antibacterial therapy of intestinal infections
00:00
Oksana Mikhailovna Drapkina , professor, doctor of medical sciences:
– In this section we have direct coverage from St. Petersburg. Professor Zakharenko Sergei Mikhailovich.
"Rational antibacterial therapy of intestinal infections."
Sergey Mikhailovich Zakharenko , professor, doctor of medical sciences:
– Good afternoon, dear colleagues! It's warm here in St. Petersburg. Intestinal infections are not yet rampant. But we must be mentally prepared for the fact that the problem, no matter how it was solved before we came into the world, will probably not be solved in the near future.
If you look at the estimates of the World Health Organization (WHO), intestinal infections occupy a fairly high place as a cause of death in the world. Fourth place in low-income countries. Sixth place overall in countries around the world.
(Slide show).
The most interesting is probably the very bottom line on this slide. The proportion of the population dying due to intestinal infections in developed countries and throughout the world differs by literally 0.001%. If compared with countries that are considered highly developed, the difference will be only 0.006%.
Both for Russia and for the United States or some countries of the African continent, the problem remains relevant for many years.
It is generally accepted that infections caused by viruses are of greatest relevance today. But if we look at the results of a European study on the effectiveness of diagnosing bacterial enteric agents, we see that for every case of campylobacteriosis that is diagnosed in Europe, there are on average 274 undiagnosed cases.
This applies to salmonellosis, shigelliosis and escherichiosis. We must be aware that about half of the cases may be due to viruses. But about half of the cases are bacterial agents that require specific attention.
(Slide show).
This house of health and the path to recovery for a patient with an intestinal infection is based on the diet. 4 pillars in the form of etiotropic therapy, rehydration, pathogenetic therapy and symptomatic therapy must be fully presented, but competently and balanced for each patient.
Today we are talking about only one extreme pillar - etiotropic therapy, which has its own problems. There is no single scheme that can be learned to cure every patient. There is no drug that can be given a 100% advantage in all cases. The problem of antibiotic resistance has not yet been solved for any pathogen or antibiotic.
02:45
A particular nuisance is due to the fact that resistance is initially formed as multi-resistance.
In conditions where patients and doctors have recommendations that equally position both first-line drugs (2-3 drugs) and second-line drugs (3-4 drugs), we must have some basis for an additional positive or negative decision in favor of one drug or another.
In addition to the antimicrobial effect, it makes sense to take into account other effects, which we will now try to talk about.
It is of fundamental importance to separate diarrhea into cases that occur in residents (those who live in the region) and non-residents (or traveler's diarrhea). It is important to identify groups of patients in whom the disease occurs with or without hemocolitis.
Speaking of traveler's diarrhea, here are some things to consider. The main etiological agents that interfere with the lives of our travelers are E. coli. The main pathogen is enterotoxigenic bacilli. Please note the dependence on studies of the host country and time of year. The proportion of enteroaggregative and enterohemorrhagic strains varies.
WHO and classicists involved in the treatment of traveler's diarrhea previously recommended 4 groups of drugs with varying degrees of evidence. Today it is Trimethoprim, Sulfamethoxazole due to the increase in global resistance. With a good level of evidence, we can operate with three groups of drugs: fluoroquinolones, Rifaximin (a non-absorbable drug) and Azithromycin.
04:28
(Slide show).
If they are comparable in terms of the level of evidence, then you see in the comments that for fluoroquinolones one should not forget about side effects and the formation of extraintestinal resistance. For Rifaximin, with a good level of safety, the question of therapy with hemocolitis is not removed. Azithromycin, despite all its charm, still cannot be used for absolutely all infections and infections occurring with hemocolitis. There are problems with the formation of resistance.
(Slide show).
This is what the current recommendations for the treatment of traveler's diarrhea look like. Antibiotics are not recommended for treating mild cases. Even Loperamide, which is actively proposed in these cases, is not necessary.
The middle part of the slide is devoted to four drugs that cost sequentially and equally. The question arises: how to choose them.
Comparing the effectiveness, we see that Rifaximin is not inferior in its effectiveness to fluoroquinolones, both in terms of choice of dosage (can be used twice) and in terms of obtaining the final result in the form of cessation of diarrhea.
What factors can be taken into account? If we look at the first line, we see that fluoroquinolones cannot escape photodermatitis in a number of cases. There is no escape from restrictions on age, pregnancy and the problem of the formation of extraintestinal resistance.
For macrolides, most restrictions have been lifted, except that resistant strains form quite quickly in adults. They register.
Rifaximin occupies a position that is quite favorable from a comparison point of view based on these restrictions. At the same time, there is a certain wariness regarding resistance, which can be overcome by the data we receive on the survival of mutants resistant to Rifaximin.
When discussing the problem of resistance of emerging mutant strains to Rifaximin, several factors should be taken into account. The first is the frequency of formation of this resistance. The second is the consequences. Ciprofloxacin gives a resistance of 10-8 against E. coli. Rifaximin differs by approximately one order of magnitude from the test drug.
06:41
It is quite rare that resistance develops in clastridians, anaerobic or aerobic cocci and bacteria. But the most interesting thing is that the formation of resistance to Rifaximin is not accompanied by the formation of resistance to other antibacterial drugs. Multidrug resistance in a complex is not typical.
The formation of chromosomal type resistance reduces the viability of strains and reduces the likelihood of horizontal transmission of resistance genes to other related microorganisms.
A wide range of inhibitory agents allows us to combat the vast majority of enteropathogens that we may encounter when discussing the problem of diarrhea. High concentration in a relatively small biovolume, distribution of the drug in the wall layer of mucus creates increased local concentrations. They persist for 3-4 days, even after discontinuation of the drug, accompanying the drug with mucus along the intestinal wall.
(Slide show).
An additional advantage of Rifaximin, used in doses from 600 mg to 1200 mg, is its activity against protozoal agents. This American study presents the treatment of patients who had mixed infections.
Antiparasitic activity is quite noticeable and interesting. Traveler's diarrhea is, of course, a wonderful event. But it is advisable not to get sick. From the point of view of prevention, antibacterial drugs have been, are being used, and will probably be used for a long time.
In the 1970s, absorbable drugs with systemic effects were actively used. But since the mid-1980s, it has been recommended to limit the use of drugs, moving to non-absorbable drugs on the market. Since 1992, the use of non-absorbable drugs has been considered quite promising, except in cases where there is reason to use drugs with a systemic effect when traveling to regions where infections susceptible to them are common or, possibly, there is a high risk of infection.
08:41
Comparing the effectiveness of Rifaximin with placebo shows, of course, several times greater effectiveness. We are not talking about randomness here. We are talking about fairly good quality and performance of the drug. Dosages that can be used in practical use are only 200 mg per day.
One to two weeks of use does not lead to catastrophic changes in the composition of either the microflora of the colon or the microflora of the small intestine.
A special property of Rifaximin is its solubility depending on the volume of bile present. High solubility in the small intestine provides both a high preventive effect and high efficiency in the presence of bacterial overgrowth syndrome in the small intestine.
A rather smoothly decreasing concentration of the drug along the colon provides a microbiocyte-preserving effect and the ability to preserve normal microflora. Or, as will be shown below, use with probiotics.
Speaking about diarrhea of residents, that is, those who are sick in their territory, you should draw your attention to several fundamental points related, first of all, to Escherichiosis.
Escherichiosis showed how severe it can be last year with an outbreak in Germany. I will now try to demonstrate the lessons of this outbreak to you. Enterotoxigenic escherichiosis, travelers' diarrhea and residents' diarrhea are treated in approximately the same way. There are no special features here.
These regimens are also used to treat diarrhea caused by enteropathogenic and E. coli. Difficulties arise with respect to enteroaggregative strains and enterohemorrhagic strains.
Considering the effectiveness of "Rifaximin", in relation to this group of pathogens, it has been reasonably shown that within 4-8 hours the degree of activity of production of both heat-labile and heat-stable toxin by enterotoxigenic Escherichia coli decreases.
(Unintelligible, 10:35) and enteroaggregative strains produce pathogenicity factors to a lesser extent. At the same time, with the use of Rifaximin, lower production of interleukin-8, which plays a role in the pathogenesis of these conditions, was noted.
10:48
The use of Rifaximin makes it possible to control the viability and population of enteroaggregative Escherichia coli. The entire group of escherichiosis falls under the more effective influence of an absorbed drug than the use of systemic drugs.
(Slide show).
Slide dedicated to the results of the epidemic caused by E. coli O104 in Germany. On the right you see good drugs that are effectively used to treat salmonellosis, dysentery or some other infections. We did not work on this group of patients.
Today, the treatment tactics for escherichiosis caused by enterohemorrhagic Escherichia coli with a high risk of developing hemolytic-uremic syndrome are based on the use of carbopenems in cases where systemic therapy is required. "Rifaximin" as a non-absorbable drug in cases where local therapy is indicated and there is no need for systemic action.
Recommended doses are controversial - from 600 mg to 1200 mg. They do not exceed average therapeutic recommendations.
(Slide show).
It is difficult to make a diagnosis from the first meeting with the patient. But patients can be divided into at least 2 groups: patients with hemocolitis and without hemocolitis. Here are the treatment regimens for patients without hemocolitis. The effective use of Rifaximin is possible if we look at the limited trials we have done comparing Alfa Normix with Ciprofloxacin.
It can be seen that the differences in the duration of diarrhea in the key syndrome in this disease are less than half a day. The drugs are again equally effective for both traveler's diarrhea and resident diarrhea.
A huge problem that has come to a head in recent years. Flashes with. difficile-associated diseases in Canada with thirty deaths suggests that today we, unfortunately, know little about this disease and are poorly diagnosed. But we clearly understand the therapeutic tactics both from foreign publications and from our own clinical experience.
Metronidazole is positioned as the drug of choice for many reasons. First of all, the cost. It is used to treat mild to severe primary episodes. If there is no effect within three days of therapy, we switch to the use of Vancomycin.
Vancomycin is the “gold standard” in the treatment of this disease. But it is quite expensive, so it is primarily recommended for severe disease or relapses.
13:15
What to do if the patient cannot be cured with these two drugs. Today, there is “Fidaksomicin” abroad, which is included in the recommendations. We only have Rifaximin.
Rifaximin can be used to treat this group of patients in doses of 400 mg to 800 mg per day for 10 to 14 days. It has a particular advantage in patients with liver damage. To date, unfortunately, we have not yet received immunoglobulins that can be used to treat this group of patients. We don't have bacteriophages.
An interesting and fundamentally important for the positioning of Rifaximin, at least the third anti-clastridial agent, is the very high level of bacteriological effectiveness, reaching 73%. While for Metronidazole and Vancomycin this figure is about 65%.
In this study, antibiotics were prescribed for 14 days. A shorter course has a greater chance of relapse.
One more circumstance. Today it is extremely difficult to find patients who do not have any problems with metabolic disorders or liver disease.
How do antibiotics interact with the liver, and are there any risks? Disulfiram-like reactions, well known, include Metronidazole, Furazolidone, and Cefoperazone. There is a fairly wide range of drugs falling into this zone.
14:41
(Slide show).
A number of drugs are frankly not recommended for liver diseases. The entire range of antimicrobial agents is presented on this slide. Do we always remember that these drugs have limited permission.
The risk of hepatotoxicity also increases with fluoroquinolones. In particular, Moxifloxacin is present here with a risk of 4.3 against the background of liver disease.
Drug interactions are an important problem, both at the intestinal level and extraintestinal interactions. "Rifaximin", having other metabolic mechanisms and being absorbed in an extremely small volume, is still capable of stimulating cytochrome P450. This promotes the metabolism of other xenobiotics.
This is not enough. As it turned out, the use of this drug in patients with damaged liver not only contributes to the level of circulating endotoxin and proinflammatory cytokines, but also has certain vaso- and cardiotropic effects. Of course, they are not direct, but indirect. However, this is an additional “bonus” that these severe patients receive.
Today, it is quite actively proposed to use antibiotics together with probiotics. How effective and safe is this therapy for probiotics? These two studies presented on the slide show the possibility of using, at a minimum, bifid-containing drugs together with Rifaximin.
The strains do not lose their probiotic properties in the presence of Rifaximin. This combination therapy appears to be quite feasible.
More interesting data was obtained literally over the last 5-7 years. They relate to the affinity of Rifaximin with the pregnane X receptor, which is involved in the regulation of an adequate nonspecific and immunological response. These properties are interesting and important from the point of view of using the drug in the treatment of not only intestinal infections, but also inflammatory bowel diseases.
Thus, today there is no doubt that our ideas about the frequency and detection of intestinal infections are somewhat underestimated. In fact, there are more of these patients. But we should not consider every patient with diarrhea as infectious. It is necessary to look for other factors and causes and fully examine patients.
We must remain alert to the possible cause of intestinal infection caused by bacterial agents and appropriately select antibacterial therapy. Far underestimated today are travelers' diarrhea and nosocomial diarrhea, including those caused by. difficile.
Therapy for diarrhea and intestinal infections cannot be without alternative. A competent assessment of the severity of symptoms and fever allows you to choose drugs with systemic or local action. Among drugs with systemic action, there is no alternative to fluoroquinolone. And among non-absorbable drugs on our market there is no alternative to Rifaximin.
C. Difficile-associated diseases should be the second target for the use of this group of drugs. In particular, Rifaximina.
(Slide show).
Only the competent use of all modern capabilities (how this turtle got out of the pen) can probably allow us to get out of the problem of the labyrinth of intestinal infections.
Thank you.
Complications of antibiotic use
When using antibiotics, there is a risk of developing unwanted reactions. Such complications include:
- Hepatotoxicity – liver damage. Most often observed when taking moxifloxacin, macrolides, and clavulanate.
- Cardiotoxicity is damage to the heart. Such a reaction can occur when using fluoroquinolones, azithromycin, clarithromycin.
- Neurotoxicity is damage to the nervous system. Occurs with fluoroquinolones.
- Allergy . Characteristic of penicillins and cephalosporins.
In fact, the wider the spectrum of antimicrobial activity, the higher the risk of adverse reactions..
Choosing an antibiotic in a child
Previously, we reviewed the main diseases of the upper and lower respiratory tract, for which antimicrobial agents can be used. Now we will analyze the main drugs that can be used for this or that pathology, and also indicate the required dosage of the drug.
Do not take antibiotics without a doctor's prescription.
Do not use medications yourself! The medications and dosages listed below are for informational purposes only and are not equivalent to treatments prescribed by a physician.
Acute otitis media
The drug of choice is amoxicillin 40-90 mg/kg/day in 3 divided doses. Duration of therapy is 10 days in children <5 years old, 5-7 days in children >5 years old. The second-line drug is amoxicillin/clavulanate. The third-line drug is josamycin.
Acute rhinosinusitis
Similar to the use of antibacterial agents for acute otitis media.
Acute tonsillitis
The drug of choice is amoxicillin 45-60 mg/kg in 3 doses, phenoxymethylpenicillin 25-50 mg/kg 3-4 times a day. The second-line drug is cefixime. The third-line drug is josamycin. Duration of therapy is 10 days.
Community-acquired pneumonia
The therapy of choice is amoxicillin IV 45-90 mg/kg/day in 3 divided doses. The second line drug is amoxicillin/clavulanate, cefuroxime IM, ceftriaxone IM. The third line drug is josamycin 40-50 mg/kg/day in 2 doses.
Antibiotics are indispensable drugs in the fight against bacterial infection. These medications should be prescribed solely for medical reasons. It is very important to adhere to the prescribed regimen of using the antibacterial agent. Do not self-medicate. If signs of infection occur, contact your pediatrician, who will help establish the diagnosis, cause of the disease, and prescribe adequate treatment.
Basics of therapy for infectious diseases
Each group of antibiotics has a different spectrum of action - the ability to destroy one or another type of bacteria. Therefore, antibiotics can be broad or narrow spectrum, or with an effect on certain pathogens.
For example, benzylpenicillin is a narrow-spectrum antibiotic, and ampicillin is a broad-spectrum antibiotic. But this does not mean that benzylpenicillin is worse. If the pathogen is known, the antibiotic should be used with as narrow a spectrum as possible so as not to destroy the normal human microflora.
When the causative agent is unknown, broad-spectrum antibiotics are used, hoping to cover as many potential pathogens as possible.
Antibiotics also differ in their ability to distribute in tissues. For example, penicillins and cephalosporins are highly effective against infections of the respiratory system and soft tissue, and tetracyclines penetrate well into bone tissue and are used to treat infections of bone tissue.