At the present stage of development and improvement of methods for treating endogenous depression, increasing attention is paid to the participation of monoamine neurotransmitters in the pathogenesis of the disease and the peculiarities of the impact of newly created psychotropic antidepressant drugs on these links [1, 2]. The pharmacological effect of different classes of antidepressant drugs introduced into psychiatric practice is due to different mechanisms of their interaction with certain brain receptors and participation in various metabolic processes. The search for thymoanaleptics that interact with both serotonergic and noradrenergic receptors, i.e., with a dual mechanism of action, led to the creation of a new class of antidepressants - selective serotonin and norepinephrine reuptake inhibitors (SNRIs). The emergence of antidepressants with a dual mechanism of action was accompanied by an increase in the effectiveness of treatment of depressive conditions and made it possible to achieve remission in 45% of patients [2, 3].
One of the SNRIs is venlafaxine, the first third-generation thymoanaleptic. In many studies [4–6], it is rated as a “reference” in the group of these compounds.
Venlafaxine and its main metabolite, O-desmethylvenlafaxine, are potent serotonin and norepinephrine reuptake inhibitors and weak dopamine reuptake inhibitors. Both the main drug and its indicated metabolite reduce β-adrenergic reactivity. Venlafaxine has no affinity for muscarinic, cholinergic, histamine, and α1-adrenergic, opioid, benzodiazepine, orencyclidine and N-methyl-α-aspartate receptors in the brain; while the ratio of monoamine transfer (serotonin/norepinephrine) with venlafaxine is 30 (compared to 9.4 for another SNRI - duloxetine). This indicates a significant predominance of the serotonergic effect in the action of venlafaxine, similar in strength to selective serotonin reuptake inhibitors (SSRIs). A group of authoritative experts in the field of psychopharmacotherapy showed [7] that venlafaxine, along with escitalopram and clomipramine, can be considered one of the most effective antidepressants.
Venlafaxine is a racemic mixture of two enantiomers: the S-enantiomer, which is a more potent serotonin reuptake inhibitor, and the R-enantiomer, a potent norepinephrine reuptake inhibitor. Thanks to this structure, the drug eliminates the deficiency of both serotonin and norepinephrine in neuronal synapses, which provides a more balanced effect on neurotransmission and synergism of psychopharmacological effects. The features of venlafaxine should also include the high selectivity of its pharmacological action, which determines its favorable tolerability and safety profile [8-10].
To date, data have been accumulated on the dose dependence of the therapeutic effect of venlafaxine. Possessing a wide range of therapeutic action, venlafaxine consistently includes serotonergic, noradrenergic and dopaminergic receptors in the spectrum of its neurochemical activity [11]. When comparing the effectiveness of venlafaxine with antidepressants from the SSRI group in a meta-analysis of 34 randomized, double-blind studies [12], which included 8,000 patients with depressive disorders of varying severity, statistically significant advantages of venlafaxine as a means of achieving remission were established.
The relatively short half-life necessitates strict adherence to the daily dosage regimen [13, 14]. Many years of successful global experience in the use of venlafaxine indicate a dose-dependent mechanism of its action, which makes it possible to use the drug as an alternative to SSRIs and tricyclic antidepressants in the treatment of both treatment-resistant depression and acutely developed primary depression both in inpatient and outpatient practice [7, 14— 19]. The favorable tolerability profile and low incidence of side effects during venlafaxine therapy are emphasized [14].
Venlafaxine has been noted to be highly effective in treating a wide range of depressive conditions within the framework of recurrent and bipolar affective disorders [14], as well as in generalized anxiety, somatogenic and post-stroke depression [4, 20].
A number of authors [5, 21, 22] note the early onset of the antidepressant effect of venlafaxine and its positive effect on the manifestations of the actual thymic component of depression, anxiety, agitation, motor retardation, and cognitive functions. However, the questions of the effect of venlafaxine on depressive states of various structures remain insufficiently developed [23].
The purpose of the study was to evaluate the clinical effect of venlafaxine during a course of treatment of patients with various depressive states of endogenous nature.
Pharmacological properties of the drug Venlafaxine
Venlafaxine is an antidepressant with a new chemical structure that cannot be classified as tricyclic, tetracyclic or other known antidepressants. It is a racemic mixture of two active enantiomers. The mechanism of the antidepressant effect of venlafaxine is associated with increased neurotransmitter activity of the central nervous system. Venlafaxine and its main metabolite O-desmethyl venlafaxine (ODV) are potent inhibitors of neuronal reuptake of serotonin and norepinephrine, and also inhibit dopamine reuptake. In addition, both single and chronic administration of venlafaxine and EDV attenuates β-adrenergic reactions. They are equally effective in influencing the reuptake of neurotransmitters. Venlafaxine does not inhibit MAO activity. Venlafaxine has no affinity for opiate, benzodiazepine, phencyclidine, or N-methyl-d-aspartate (NMDA) receptors; it also does not affect the release of norepinephrine from brain tissue. With repeated use of the drug, equilibrium concentrations of venlafaxine and its only active metabolite in the blood plasma are achieved within 3 days. Venlafaxine and EDV have linear pharmacokinetics with total daily doses ranging from 75 to 450 mg. Absorption of venlafaxine after taking a single dose of the drug orally is almost 92%, absolute bioavailability is about 45%. After administration of Velaxin extended-release capsules, maximum plasma concentrations of venlafaxine and its active metabolite EDV are achieved within approximately 6 and 8 hours, respectively. The rate of absorption of venlafaxine released from extended-release capsules is less than the rate of its elimination. Therefore, the average half-life of venlafaxine from the body after oral administration (15 ± 6 hours) is actually the half-life in the absorption phase, and not the half-life in the distribution phase (5 ± 2 hours), which is observed after the use of tablets. After administration of venlafaxine in equivalent doses in tablet or extended-release capsule form, venlafaxine AUC exposure and EDV were similar in both dosage forms, and their plasma concentrations were slightly lower after administration of venlafaxine in capsule form. Thus, extended-release capsules provide slower absorption but the same extent of absorption (i.e., AUC) as venlafaxine tablets. Venlafaxine is extensively metabolized during the initial passage through the liver, mainly with the participation of CYP 2D6, with the formation of the main metabolite EDV. It is also metabolized to N-desmethyl venlafaxine and some other metabolites with the participation of CYP 3A3/4. Venlafaxine and its metabolites are excreted mainly by the kidneys. About 78% of the administered dose of venlafaxine is determined in the urine over 48 hours in the form of unchanged venlafaxine, unconjugated EDV, conjugated EDV or other metabolites. In case of renal and hepatic insufficiency, the half-life of venlafaxine and its active metabolite EDV increases. Taking the drug with food does not affect the absorption of venlafaxine and the further formation of EDV. The age and gender of the patient do not affect its pharmacokinetics. Venlafaxine does not accumulate in the body. Venlafaxine extended-release capsules contain microspheres, which, when entering the gastrointestinal tract, slowly release the active component. The insoluble part of these microspheres is excreted in the feces.
Venlafaxine organic 37.5 mg 30 pcs. film-coated tablets
pharmachologic effect
Antidepressant.
Composition and release form Venlafaxine organic 37.5 mg 30 pcs. film-coated tablets
Tablets - 1 tablet:
- Active substance: venlafaxine - 37.5/75 mg;
- Excipients;
- mCC - 53.03/106.06 mg; lactose monohydrate (milk sugar) - 35.1/70.2 mg; sodium carboxymethyl starch (Primogel) - 15.7/31.4 mg; povidone (low molecular weight medical PVP) K17 - 2.65/5.3 mg; magnesium stearate - 1.1/2.2 mg;
- film shell;
- Opadry II (85F28751) white (polyvinyl alcohol - 2/4 mg, titanium dioxide - 1.25/2.5 mg, macrogol (PEG) - 1.01/2.02 mg, talc - 0.74/1.48 mg) - 5/10 mg.
There are 30 pieces in a package.
Description of the dosage form
White or almost white, film-coated tablets, round, biconvex; On a cross section, the core is white or almost white.
Directions for use and doses
The recommended starting dose is 75 mg in 2 divided doses daily (37.5 mg 2 times a day). Depending on tolerability and effectiveness, the dose may be gradually increased to 150 mg/day. If necessary, the dose is increased to 225 mg/day. Dose increases by 75 mg/day can be made at intervals of 2 weeks or more; if clinically necessary, due to the severity of symptoms, it is possible to increase the dose in a shorter period of time, but not less than 4 days. Higher doses (up to a maximum daily dose of 375 mg/day in 2-3 doses) require inpatient monitoring of patients. After achieving the required therapeutic effect, the daily dose can be gradually reduced to the minimum effective level.
Maintenance therapy and relapse prevention. Maintenance treatment can last 6 months or more. The minimum effective doses used in the treatment of a depressive episode are prescribed.
Kidney failure. In case of mild renal failure (GFR > 30 ml/min), no dosage adjustment is required. In case of moderate renal failure (GFR 10-30 ml/min), the dose should be reduced by 25-50%. Due to the prolongation of T1/2 of venlafaxine and its active metabolite (EAM), such patients should take the entire dose once a day. It is not recommended to use venlafaxine in severe renal failure (GFR less than 10 ml/min)).
Take orally during meals, preferably at the same time, without chewing and with liquid.
Pharmacodynamics
Venlafaxine is an antidepressant that does not chemically belong to any class of antidepressants (tricyclic, tetracyclic or others) and is a racemate of two active enantiomers.
Venlafaxine and its main metabolite, O-desmethylvenlafaxine (ODV), are strong SNRIs and weak dopamine reuptake inhibitors.
The mechanism of the antidepressant effect of the drug is associated with its ability to potentiate the transmission of nerve impulses to the central nervous system.
Venlafaxine and ODV are equally effective in influencing the reuptake of the above-mentioned neurotransmitters, while they do not have an affinity (studied in vitro) for cholinergic (muscarinic), H1-histamine, alpha1-adrenergic, opiate and benzodiazepine receptors, and do not suppress MAO activity. Also have no affinity for opiate, phencyclidine, or N-methyl-d-aspartate (NMDA) receptors. Venlafaxine is inferior to SSRIs in inhibiting serotonin reuptake. In addition, venlafaxine and EDV reduce beta-adrenergic reactivity both after a single dose and with chronic use.
Pharmacokinetics
Absorption. Absorption from the gastrointestinal tract is good, about 92% for a single dose, and is not quantitatively dependent on food intake.
Distribution. Overall bioavailability is 40-45%, which is associated with intense first-pass metabolism in the liver. Venlafaxine and EDV bind to human plasma proteins by 27 and 30%, respectively; they both pass into breast milk. In the range of daily doses of venlafaxine 75-450 mg, venlafaxine and EDV have linear kinetics. Tmax in blood plasma of venlafaxine and EDV is 2 and 3 hours, respectively, after taking Venlafaxine tablets orally.
When taking long-acting forms of venlafaxine, Tmax is 5.5 and 9 hours, respectively.
T1/2 was (5±2) hours and (11±2) hours for venlafaxine and EDV, respectively.
Css for venlafaxine and EDV is achieved after 3 days of multiple therapeutic doses.
Metabolism. Metabolized mainly in the liver with the participation of the CYP2D6 isoenzyme to the only pharmacologically active metabolite (EFA), as well as to the inactive metabolite N-desmethylvenlafaxine.
Venlafaxine is a weak inhibitor of the CYP2D6 isoenzyme and does not inhibit CYP1A2, CYP2C9 or CYP3A4.
Excretion. Excreted primarily by the kidneys: approximately 87% of a single dose taken is excreted in the urine within 48 hours (5% unchanged, 29% as unconjugated EDV, 26% as conjugated EDV, 27% as other inactive metabolites) , and after 72 hours, 92% of the drug is excreted by the kidneys.
The mean ± standard deviation for plasma clearance of venlafaxine and EDV is (1.3 ± 0.6) and (0.4 ± 0.2) L/h/kg, respectively; apparent T1/2 (5±2) and (11±2) h, respectively; apparent Vss (7.5±3.7) and (5.7±1.8) l/kg, respectively.
Special groups of patients.
The gender and age of the patient do not have a significant effect on the pharmacokinetic parameters of venlafaxine and EFA.
For elderly patients, no special dose adjustment is required depending on age.
In patients with low activity of the CYP2D6 isoenzyme, there is no need to select individual doses. Despite the multidirectional changes in concentrations taken separately, namely venlafaxine (increases) and EDV (decreases), the sum of the AUC of these two active substances does not actually change due to a decrease in the activity of the CYP2D6 isoenzyme; accordingly, no dose adjustment is required.
In patients with moderate to severe hepatic and renal insufficiency, the metabolism of venlafaxine and the excretion of EDV is reduced, the Cmax of venlafaxine and EDV is increased, and T1/2 is prolonged. The decrease in the total clearance of venlafaxine is most pronounced in patients with creatinine Cl below 30 ml/min, as well as in patients on renal dialysis (T1/2 increases by 180% for venlafaxine and by 142% for ODV, and the clearance of both active substances decreases by approximately by 57%). For such patients, especially those on hemodialysis, it is necessary to individually select the dose of venlafaxine and monitor the kinetics, taking into account the duration of treatment with this drug.
Although data for patients with severe Child-Pugh hepatic impairment are limited, it should be borne in mind that individual variations in pharmacokinetics, in particular drug clearance and T1/2, are very variable, which should be taken into account when prescribing venlafaxine to such patients. In patients with Child-Pugh class A (mild liver dysfunction) and Child-Pugh class B (moderate impairment), the T1/2 of venlafaxine and EDV is approximately 2 times longer than that in healthy patients, and clearance is reduced by more than half.
Indications for use Venlafaxine organic 37.5 mg 30 pcs. film-coated tablets
Depression (prevention and treatment).
Contraindications
- Hypersensitivity to venlafaxine or any of the excipients;
- simultaneous use with MAO inhibitors;
- severe renal and/or liver dysfunction (GFR
Application Venlafaxine organic 37.5 mg 30 pcs. film-coated tablets during pregnancy and breastfeeding
Contraindicated for children under 18 years of age and during pregnancy and breastfeeding.
special instructions
Recent myocardial infarction; unstable angina; arterial hypertension; tachycardia; history of convulsive syndrome; increased IOP; angle-closure glaucoma; history of manic states; predisposition to bleeding from the skin and mucous membranes; initially reduced body weight.
Overdose
Symptoms: impaired consciousness (from drowsiness to coma), agitation, possible vomiting, diarrhea; tremor, decrease or (mild) increase in blood pressure, dizziness, mydriasis, convulsive states, sinus or ventricular tachycardia or bradycardia; changes on the ECG (prolongation of the QT interval, bundle branch block, widening of the QRS complex). Post-marketing experience indicates that the most common overdose of venlafaxine occurred with concomitant use of alcohol and/or other psychotropic drugs. There are repeated reports of deaths. Published literature on retrospective studies of venlafaxine overdoses report that this increased risk of fatal outcomes may be inherent in venlafaxine when compared with commercially available SSRI antidepressants, but this risk is lower than the risk inherent in tricyclic antidepressants. Epidemiological studies have shown that those patients treated with venlafaxine have a greater risk of suicide compared with those patients treated with SSRIs (other than venlafaxine). However, it remains unclear to what extent these high rates of death (due to venlafaxine overdose) are due to the toxic properties of the drug itself or the special characteristics of the group of patients treated with venlafaxine. According to clinical experience, it is recommended that prescriptions for venlafaxine prescribe the minimum possible amount, sufficient only until the patient's next visit to the doctor, in order to reduce the risk of intentional overdose.
Treatment: symptomatic and supportive therapy is provided. Specific antidotes are unknown. Continuous monitoring of vital functions (respiration, circulation and heart rate) is recommended. In case of overdose, immediate gastric lavage and administration of activated charcoal are recommended to reduce absorption of the drug. It is not recommended to induce vomiting if there is a risk of aspiration of vomit. Forced diuresis, dialysis, and blood transfusion are ineffective.
Side effects Venlafaxine organic 37.5 mg 30 pcs. film-coated tablets
General symptoms: often - weakness, increased fatigue, chills; uncommon - Quincke's edema, photosensitivity reactions; frequency not established - anaphylactic reactions.
From the nervous system: very often - dry mouth, headache; often - unusual dreams, decreased libido, dizziness, insomnia, increased excitability, paresthesia, stupor, confusion, depersonalization, increased muscle tone, tremor; infrequently - apathy, agitation, hallucinations, myoclonus, impaired coordination of movements and balance; rarely - akathisia, psychomotor agitation, epileptic seizures, manic reactions; frequency not established - dizziness, neuroleptic malignant syndrome (NMS), serotonin syndrome, delirium, extrapyramidal reactions (including dystonia and dyskinesia), tardive dyskinesia, suicidal thoughts and behavior, aggression.
From the gastrointestinal tract: very often - nausea; often - loss of appetite (anorexia), constipation, vomiting; infrequently - bruxism, diarrhea; rarely - hepatitis; frequency not established - pancreatitis.
From the respiratory system: often - yawning, bronchitis, shortness of breath; rarely - interstitial lung diseases (ILD) and eosinophilic pneumonia, chest pain.
From the cardiovascular system: often - arterial hypertension, hyperemia of the skin; uncommon - postural hypotension, tachycardia, fainting; frequency not established - hypotension, QT interval prolongation, ventricular fibrillation, ventricular tachycardia (including bidirectional tachycardia).
From the hematopoietic system: infrequently - hemorrhages into the skin (ecchymosis), gastrointestinal bleeding; frequency not established - hemorrhages in the mucous membranes, prolongation of bleeding time, thrombocytopenia, pathological changes in the blood (including agranulocytosis, aplastic anemia, neutropenia and pancytopenia).
From the metabolic side: often - increased cholesterol levels in the blood serum, decreased body weight; infrequently - weight gain; very rarely - an increase in prolactin levels; frequency not established - changes in laboratory tests of liver function, hepatitis, hyponatremia, syndrome of insufficient ADH secretion.
From the genitourinary system: often - ejaculation/orgasm disorders in men, erectile dysfunction (impotence), anorgasmia, dysuric disorders (mainly difficulty in starting urination), pollakiuria, menstrual disorders associated with increased bleeding or increased irregular bleeding (menorrhagia, metrorrhagia); infrequently - orgasm disorders in women, urinary retention; rarely - urinary incontinence.
From the senses: often - disturbances of accommodation, mydriasis, blurred vision; infrequently - disturbance of taste, noise or ringing in the ears; frequency not established - angle-closure glaucoma.
From the skin: very often - sweating; infrequently - alopecia, a rapidly passing rash; frequency not established - erythema multiforme, toxic epidermal necrolysis, Stevens-Johnson syndrome, itching, urticaria.
From the musculoskeletal system: frequency not established - rhabdomyolysis.
When you stop taking venlafaxine, abruptly discontinue it, or reduce the dose, you may experience symptoms that are referred to as so-called. withdrawal syndrome: increased fatigue, asthenia, headache, dizziness, sleep disturbances (drowsiness or insomnia, difficulty falling asleep, the appearance of unusual dreams), hypomania, anxiety, agitation (increased nervous excitability and irritability), confusion, paresthesia (including spontaneously occurring unpleasant sensation of numbness, tingling, burning, crawling), increased sweating, dry mouth, decreased appetite, nausea, vomiting, diarrhea (most of these reactions are mild and do not require treatment).
Drug interactions
Venlafaxine, which itself does not have increased binding to plasma proteins, practically does not increase the concentration of simultaneously taken drugs, which are characterized by high binding to plasma proteins. No clinically significant interaction with antihypertensive (including beta-blockers, ACE inhibitors, diuretics) and antidiabetic drugs was detected.
Caution should be exercised when co-administered with other drugs that affect the central nervous system, since the interaction of venlafaxine with such drugs has not been studied.
MAO inhibitors. The simultaneous use of venlafaxine with MAO inhibitors, as well as within 14 days after their discontinuation, is contraindicated (the risk of severe side effects, including death, is likely). Therapy with MAO inhibitors can be prescribed no less than 7 days after discontinuation of the drug Venlafaxine. Venflaxin should be discontinued at least 7 days before starting reversible selective MAO inhibitors (moclobemide). The weakly reversible and non-selective MAO inhibitor linezolid (an antimicrobial drug) and methylene blue (IV dosage form) are also not recommended for simultaneous use with venlafaxine.
Serotonergic agents. Caution should be exercised in the simultaneous use of drugs that affect the serotonergic transmission of drugs, such as triptans (including sumatriptan, zolmitriptan), SSRIs, SNRIs (prolonged seizures have been reported), tricyclic antidepressants, lithium, sibutramine or fentanyl (including including its analogues - dextromethorphan, tramadol), as well as excess sources of tryptophan due to the increased potential risk of serotonin syndrome.
Alcohol. During treatment with venlafaxine, alcohol should be completely avoided. Alcohol increases the psychomotor dysfunction that venlafaxine can cause.
Lithium. Lithium preparations do not have a significant effect on the pharmacokinetics of venlafaxine.
Diazepam. There was no effect of orally administered diazepam on the pharmacokinetics of venlafaxine and EDV, and, conversely, venlafaxine did not change the pharmacokinetics of diazepam and its metabolite desmethyldiazepam. In addition, the administration of both of these drugs does not impair the psychomotor effects and psychometric indicators caused by diazepam.
Cimetidine. The simultaneous administration of cimetidine and venlafaxine led to a delay in metabolism during the first passage of venlafaxine through the liver. Oral clearance of venlafaxine decreased by 43%, and AUC and Cmax of the drug increased by 60%. However, such an impact was not evident for EFA. Since the total activity of venlafaxine and EFA is expected to increase only slightly, no dose adjustment will be required for most normal patients. However, in patients with existing (detected) hypertension, elderly patients and those with impaired liver or kidney function, the dose of venlafaxine may be adjusted.
Haloperidol. In a study where venlafaxine was administered in the Css stage at a dose of 150 mg/day, a 42% decrease in total oral haloperidol clearance was observed after a 2 mg oral dose; while AUC increased by 70%, and Cmax by 88%, while T1/2 of haloperidol did not change. This should be taken into account when choosing the correct dose of haloperidol.
Imipramine. Venlafaxine does not impair the pharmacokinetics of imipramine and 2-hydroxyimipramine. However, the AUC, Cmax and Cmin of desipramine (the active metabolite of imipramine) increased by approximately 35% when co-administered with venlafaxine. The concentration of 2-hydroxydesipramine also increases 2.5 or 4.5 times (depending on the dose of venlafaxine: 37.5 mg or 75 mg 2 times a day), but the clinical significance of this fact is unknown.
Metoprolol. When using metoprolol and venlafaxine simultaneously, caution should be exercised because due to pharmacokinetic interaction, the concentration of metoprolol in the blood plasma increases by approximately 30-40%, without changing the concentration of its active metabolite alpha-hydroxymetoprolol. The clinical significance of this interaction has not been studied. Metoprolol does not affect the AUC of venlafaxine and EDV.
Risperidone. When used concomitantly with risperidone (despite an increase in the AUC of risperidone), the pharmacokinetics of a pair of active molecules (risperidone and 9-hydroxyrisperidone) do not change significantly when combined with venlafaxine.
Clozapine. During post-marketing studies of venlafaxine, it was found that when used simultaneously with clozapine, its concentration in the blood plasma increases. This was manifested by an increase in the side effects of clozapine, especially in relation to the incidence of seizures.
Indinavir. With simultaneous use, the pharmacokinetics of indinavir changes (AUC decreases by 28% and Cmax decreases by 36%). There are no changes in the pharmacokinetics of venlafaxine. The clinical significance of this fact is unknown.
Ketoconazole. A pharmacokinetic study when combined with ketoconazole showed an increase in plasma concentrations of venlafaxine and EDV in subjects whose initial metabolism by CYP2D6 is either good (X-Met) or poor (P-Met). In particular, the Cmax of venlafaxine increased by 26% for X-Met and by 48% for P-Met. EFA Cmax values increased by 14 and 29% in X-Met and P-Met subjects, respectively. The AUC of venlafaxine increased by 21% in X-Met and by 70% in P-Met. EFA AUC values increased by 23 and 33% in X-Met and P-Met subjects, respectively.
Drugs that affect blood clotting and platelet function (NSAIDs, acetylsalicylic acid preparations and other anticoagulants). Serotonin, released by platelets, plays an important role in hemostasis (stopping bleeding). Epidemiological studies demonstrate an association between the use of psychotropic medications that interfere with serotonin reuptake and the incidence of upper GI bleeding. This relationship is enhanced if NSAIDs, drugs containing acetylsalicylic acid, or other anticoagulants are used simultaneously. The risk of bleeding has been shown to increase when SSRIs and SNRIs (including venlafaxine) are prescribed concomitantly with warfarin. Patients prescribed warfarin should be closely monitored for PT and/or partial thromboplastin time, especially when co-administration with venlafaxine is started or stopped.
Interaction with other drugs at the level of studied metabolism with cytochrome P450 isoenzymes. The main routes of metabolism of venlafaxine include the isoenzymes CYP2D6 and CYP3A4: the first of them converts venlafaxine into its active metabolite EDV, and the second is less important in the metabolism of venlafaxine compared to CYP2D6 and forms the product N-desmethylvenlafaxine with little pharmacological activity. Preclinical studies have shown, and subsequently confirmed clinically, that venlafaxine is a relatively weak inhibitor of CYP2D6. Therefore, even when prescribing drugs that moderately suppress the activity of this enzyme or in the case of treating patients with a genetically determined decrease in CYP2D6 function, no dose adjustment of venlafaxine is required, because the total concentration of the active substance and active metabolite (venlafaxine and EDV) does not change significantly. This characterizes venlafaxine positively when compared with other antidepressants. Caution should be exercised when co-administered with CYP2D6 inhibitors such as quinidine, paroxetine, fluoxetine, haloperidol, perphenazine, levomepromazine, because in this case, venlafaxine may potentially increase plasma concentrations of these CYP2D6 substrates. In combination with drugs that inhibit both enzymes (CYP2D6 and CYP3A4), special caution is required. Such drug interactions have not yet been sufficiently studied and in this case such a combination of drugs is not recommended. In addition, venlafaxine does not suppress the activity of the enzymes CYP3A4, CYP1A2 and CYP2C9, therefore, no significant interaction is observed with drugs such as alprazolam, caffeine, carbamazepine, diazepam, tolbutamide, terfenadine.
Interaction with ketoconazole is described above. CYP3A3/4 inhibitors such as itraconazole and ritonavir can have a similar effect.
Other interactions with various concomitant therapeutic factors and food. When using venlafaxine, special caution should be exercised during electroconvulsive therapy, because There is no experience with the use of venlafaxine in these conditions. A significant effect of different types of food on the absorption of venlafaxine and its subsequent conversion to EDV has not been identified. Foods (usually high in protein, such as hard cheeses, fish roe, turkey), as well as dietary supplements and fitness diets that contain tryptophan, potentially increase the body's production of serotonin, which may increase the serotonergic side effects of venlafaxine.
Preparations containing St. John's wort. Undesirable pharmacodynamic interactions may occur when Venlafaxine is taken simultaneously with the medicinal plant St. John's wort (herb or various preparations made from it); such a combination is not recommended.
There are reports of false-positive results of the immunochromatographic rapid urine test (test strip) for phencyclidine and amphetamines in patients taking venlafaxine, even several days after discontinuation of venlafaxine. This may be explained by the lack of specificity of this test. Only a confirmatory test in a specialized anti-doping laboratory can distinguish venlafaxine from phencyclidine and amphetamines.
According to the data available to date, venlafaxine has not shown itself to be a drug that causes drug abuse or addiction (both in preclinical receptor affinity studies and in clinical practice).
Use of the drug Venlafaxine
Capsules should be taken whole with a meal with liquid. Capsules should not be divided, crushed, chewed or dissolved. The daily dose should be taken in one dose (morning or evening) at the same time. Depression The recommended dose is 75 mg/day in one dose. If, taking into account the course of the disease, a higher dose is necessary, for example, in case of severe depression or inpatient treatment of the patient, the recommended initial dose may be 150 mg/day in one dose. After this, the daily dose can be increased by 37.5–75 mg at intervals of ≥2 weeks, but not less than 4 days until the required therapeutic effect is achieved. The recommended maximum dose of venlafaxine is 225 mg/day for moderate depression and 350 mg for severe depression. After achieving the desired therapeutic effect, the dose should be gradually reduced to the minimum effective, taking into account the individual response and tolerability of each patient. When used in high doses, the risk of developing side effects of the drug increases. Generalized anxiety disorders and social anxiety disorders (social phobia) The recommended dose of venlafaxine is 75 mg/day in one dose. If after 2 weeks of treatment there is no noticeable improvement in the condition, the daily dose can be increased to 150 mg/day in one dose. When used in a daily dose of 75 mg, an anxiolytic effect is observed after 1 week. Prevention of relapses or new episodes The effectiveness of venlafaxine has been established with long-term therapy (up to 12 months for depression and social phobia; up to 6 months for generalized anxiety disorders). Treatment of acute episodes of depression must be continued for at least 6 months. The doses typically used to prevent a relapse or new episode are similar to those used to treat patients with a primary episode. It is necessary to regularly (at least once every 3 months) examine the patient to monitor the effectiveness of long-term therapy with venlafaxine. Transferring patients receiving therapy with venlafaxine in tablet form to taking the drug in capsules Patients with depression receiving venlafaxine tablets in a therapeutic dose can be switched to taking the drug in the form of extended-release capsules with the appointment of the nearest equivalent dose. Sometimes individual dose adjustment may be required. Renal failure At a glomerular filtration rate of 30 ml/min, no dose adjustment is required. With a glomerular filtration rate of 10–30 ml/min, the dose should be reduced by 50%. Due to the increased half-life of venlafaxine and its active metabolite in these patients, the daily dose should be taken in one dose. It is not recommended to use venlafaxine if the glomerular filtration rate is ≤10 ml/min, since there is insufficient data on therapy in these patients. For patients on hemodialysis, the daily dose of the drug should be reduced by 50% and, if possible, used after completion of the hemodialysis procedure. Liver failure In mild liver failure (prothrombin time ≤14 s), no dose adjustment is required. In case of moderately severe liver failure (prothrombin time - 14–18 s), the dose should be reduced by 50%. It is not recommended to use venlafaxine in severe hepatic impairment (prothrombin time 18 s), as there is insufficient data on this therapy. Elderly patients Caution should be exercised when prescribing the drug to elderly patients (due to the possibility of renal dysfunction), and the drug is prescribed in the minimum effective dose. When increasing the dose, the patient should be under regular medical supervision. Cancellation of venlafaxine Abrupt cessation of venlafaxine therapy, especially after taking the drug in high doses, may cause the development of withdrawal syndrome, and therefore a gradual dose reduction is recommended before complete discontinuation of the drug. If the drug has been used in high doses for 6 weeks, a dose reduction period of at least 2 weeks is recommended. The length of the period required to reduce the dose depends on the dose size, duration of therapy, as well as the individual sensitivity of the patient.
Material and methods
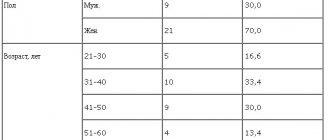
We examined 32 patients, 15 women and 17 men, aged from 18 to 57 years (average age 31.75 years) with endogenous depression, who were undergoing inpatient treatment in the clinical departments of the department for the study of endogenous mental disorders and affective states of the Federal State Budgetary Institution "Research Center for Mental Health" » RAS.
The design of the study was open naturalistic. The average duration of the disease from its first manifestation was 7.9 years, the average number of depressive episodes suffered before inclusion in the study was 3.3. The duration of the current depressive episode before starting Velaxin was on average 4.5 months.
According to nosological affiliation, the patients were distributed as follows: 22 (68.6%) patients were diagnosed with endogenous affective diseases - manic-depressive psychosis (MDP), cyclothymia; in 5 (15.6%) depression developed in the dynamics of low-progressive schizophrenia, and in 5 (15.6%) postpsychotic depression was noted in the context of paroxysmal schizophrenia. According to ICD-10, the depressive state of patients was diagnosed according to the following categories: F31.3—F31.4; F32.0—F32.2; F33.0—F33.2; F21; F20.4. Typologically, depressive states were defined as melancholy (3 patients, 9.4%), anxious (11 cases; 34.4%) and apatho-adynamic (18 patients; 56.2%). Thus, in accordance with the two-level psychopathological model of depression [24], its first 2 types were defined as typical, representing positive affectivity (sad and anxious depression), apatho-adynamic depression as atypical and related to negative affectivity.
According to the total scores on the Hamilton Depression Scale (HAM-D) before treatment: mild depressive disorders were registered in only 2 (6.25%) people, moderate in 13 (40.6%), severe depression in 17 (53.15%), i.e., the vast majority of patients had moderate to severe depression.
The study used venlafaxine, marketed as Velaxin 75 mg tablets (Hungary). The drug was prescribed orally, starting from 37.5-75 mg per day. Subsequently, based on the condition of the patients, over the next few days the daily dose was increased, reaching the maximum for a given patient, but not more than 300 mg. On average, the highest mean dose of Velaxin used was 182.1–198.2 mg per day. The drug was taken twice, morning and evening. According to the study protocol, the course of Velaxin therapy was 56 days (8 weeks).
To assess the severity of depressive symptoms and determine the therapeutic effect, in addition to the clinical observation method, the HAM-D-24 scale, containing 24 signs, was used. The severity of depressive symptoms was assessed before the start of the course of treatment (day 0), then on days 1, 3, 5 of therapy and then at the end of each of the 8 weeks of course treatment. The effectiveness of the antidepressant effect of velaxin was assessed by the degree of reduction in HAM-D scores in % relative to the score before treatment in the following gradations: reduction in scores up to 20% - as “insignificant”, by 21-50% - as “moderate”, by 51- 80% - as “good” and 81-100% - as a “significant” effect (including “practical recovery”). A decrease in the total HAM-D score to 6 or less meant complete “entry” into remission. Maintaining the HAM-D depression severity score at the same level or increasing the total score was regarded as no effect or “worsening” of the condition. To assess the spectrum of antidepressant action of Velaxin, the degree of reduction in the average total score of individual signs identified in the HAM-D was determined, conditionally characterizing melancholic or sad (items 1-3, 22-24), apatho-adynamic (items 7 and and anxious (items 9 and 10) manifestations in the structure of the depressive state.
The severity of depressive symptoms was assessed before the start of the course of treatment (day 0), then on days 1, 3, 5 of therapy and then at the end of each of the 8 weeks of course treatment. The effectiveness of the antidepressant effect of velaxin was assessed by the degree of reduction in HAM-D scores in % relative to the score before treatment in the following gradations: reduction in scores up to 20% - as “insignificant”, by 21-50% - as “moderate”, by 51- 80% - as “good” and 81-100% - as a “significant” effect (including “practical recovery”). A decrease in the total HAM-D score to 6 or less meant complete “entry” into remission. Maintaining the HAM-D depression severity score at the same level or increasing the total score was regarded as no effect or “worsening” of the condition. To assess the spectrum of antidepressant action of Velaxin, the degree of reduction in the average total score of individual signs identified in the HAM-D was determined, conditionally characterizing melancholic or sad (items 1-3, 22-24), apatho-adynamic (items 7 and and anxious (items 9 and 10) manifestations in the structure of the depressive state.
In addition, at the above periods, the severity of the depressive state and the degree of its improvement over time were assessed using the CGI Clinical Global Impression scale and its subscales CGI-S and CGI-I. To record side effects, the UKU interview scale was used, which consists of 4 subscales that allow us to distinguish mental, neurological, autonomic and so-called other side effects.
Contraindications to the use of the drug Venlafaxine
Hypersensitivity to venlafaxine. Simultaneous use of any antidepressant from the MAO inhibitor group, as well as for 14 days after discontinuation of irreversible MAO inhibitors. After complete discontinuation of venlafaxine, therapy with MAO inhibitors can be started no earlier than 7 days later. Diseases of the cardiovascular system (heart failure, coronary artery disease, ECG changes - pre-existing increase in the QT on the ECG), hypertension (arterial hypertension), electrolyte imbalance. Age up to 18 years. During pregnancy and breastfeeding.
Side effects of the drug Venlafaxine
Side effects are divided by body system and frequency of occurrence: very often (1/10); often (≤1/10, but 1/100); sometimes (≤1/100, but 1/1000); rare (≤1/1000); very rare (≤1/10,000). General symptoms: very often - asthenia, headache; often - abdominal pain, chills, increased body temperature; rarely - anaphylaxis. Gastrointestinal tract: very often - constipation, nausea; often - loss of appetite, diarrhea, vomiting; sometimes - bruxism, reversible increase in the activity of liver enzymes; rarely - gastrointestinal bleeding; very rarely - pancreatitis. Cardiovascular system: often - tachycardia, hypertension (arterial hypertension), dilatation of blood vessels; sometimes - hypotension/orthostatic hypotension, loss of consciousness, arrhythmias, tachycardia; very rarely - pirouette-type tachycardia, increased QT on ECG, ventricular tachycardia, ventricular fibrillation. Respiratory system: often - difficulty breathing, yawning; very rarely - eosinophilic infiltrates in the lungs. Nervous system: very often - dizziness, dry mouth, insomnia, anxiety, drowsiness; often - unusual dreams, agitation, anxiety, confusion, increased muscle tone, paresthesia, tremor; sometimes - apathy, hallucinations, myoclonus; rarely - ataxia with impaired balance and coordination of movements, speech impairment, including dysarthria, mania or hypomania, as well as manifestations that resemble neuroleptic malignant syndrome (NMS), seizures, serotonergic syndrome; very rarely - delirium, extrapyramidal disorders, including dyskinesia and dystonia, psychomotor agitation/akathisia. Genitourinary system: very often - anorgasmia, erectile dysfunction, impaired ejaculation and orgasm; often - frequent urination, decreased libido, menstrual irregularities; sometimes - urinary retention, menorrhagia; rarely - galactorrhea. Sense organs: often - blurred vision and accommodation, mydriasis, noise and ringing in the ears; sometimes - a change in taste sensations. Skin: very often - sweating; often - skin rash and itching; sometimes - angioedema, maculopapular rash, urticaria, photosensitivity, alopecia; rarely - erythema multiforme, Stevens-Johnson syndrome. Blood system: sometimes - ecchymosis, bleeding from the mucous membrane; rarely - increased bleeding time, hemorrhage, thrombocytopenia; very rarely - agranulocytosis, aplastic anemia, neutropenia, pancytopenia. Metabolism: often - increased cholesterol levels in the blood serum, increase or decrease in body weight; sometimes - hyponatremia, increased activity of liver transaminases; rarely - hepatitis; very rarely - increased prolactin levels. Musculoskeletal system: often - arthralgia, myalgia; sometimes - muscle spasms; very rarely - rhabdomyolysis.
Psychiatry Psychiatry and psychopharmacotherapy named after. P.B. Gannushkina No. 06 2006
The modern classification of antidepressants (thymoanaleptics) according to their mechanism of action (related to the effect on monoamine metabolism) is largely conditional. The fact is that the effect of any thymoanaleptic on monoamine metabolism varies significantly. A very illustrative example of this pattern is venlafaxine. This antidepressant belongs to one of the most dynamically developing groups of thymoanaleptics - selective serotonin and norepinephrine reuptake inhibitors (SNRIs). However, the mechanism of action of venlafaxine has a number of unique features [1]. In particular, this concerns the effect of the drug on monoamine metabolism. Thus, it has been established that in low and medium doses, venlafaxine primarily provides an increase in serotonin levels. Subsequently, as the dose of the antidepressant increases, the concentration of norepinephrine also increases. This feature of the drug’s mechanism of action is associated with the spatial geometry of its molecule. Ideally, the latter should coincide as closely as possible (or be complementary) with the “point of application” of the antidepressant - the enzyme that ensures the reuptake of serotonin or norepinephrine. Only in this case will these processes be permanently blocked. Accordingly, the opportunity opens up for a significant increase in the concentration of monoamines in the brain. However, the shape of the venlafaxine molecule is best suited for inhibiting serotonin reuptake (Fig. 1). As a result, the effect of the antidepressant on the metabolism of serotonin and norepinephrine is characterized by a ratio of 30 to 1 [2, 3]. In other words, in low and medium doses, venlafaxine behaves more like a selective serotonin reuptake inhibitor - SSRI (Fig. 2). The dual action of venlafaxine (in relation to two monoamines) appears only in high doses, when it begins to more effectively block the reuptake of norepinephrine (Fig. 3). It would seem that such an imbalance in the effects of the antidepressant should prevent the widespread use of venlafaxine. However, in reality, the situation is that these features of the mechanism of action rather add to the popularity of the drug, at least abroad. For example, a Medline search yields 664 references to various articles that contain mention of this antidepressant and appeared from 2004 to 2005. What are the reasons for this phenomenon? This may be due to the fact that venlafaxine, due to the described features of action, is essentially not one, but two drugs. In low and medium doses (up to 225 mg/day) it can be used as an SSRI in outpatient and inpatient practice. Accordingly, this antidepressant finds its use in the treatment of not only mild and moderate depression, but also in various anxiety-phobic disorders. In any case, venlafaxine has been reported to be effective in the treatment of generalized anxiety disorder [4], post-traumatic stress disorder, panic disorder [5], and social phobia [6]. At higher doses, venlafaxine “turns” into a real SNRI and its effectiveness increases significantly [7]. In particular, it has been shown that the clinical effects of the antidepressant in question most closely approximate the properties of tricyclic antidepressants (TCAs) when implementing a strategy of rapidly increasing dosages beyond the recommended average (225 mg/day) [8]. Thus, in a study by German authors [9], it was demonstrated that increasing the dose of venlafaxine over 5 days to 375 mg/day significantly accelerates and intensifies the therapeutic activity of the drug in the treatment of severe endogenous depression. Moreover, in this situation, venlafaxine demonstrated not only equal effectiveness with an antidepressant from the TCA group (imipramine), but also an even faster (by 7 days) onset of thymoleptic action. It is also proposed to use the drug in question in daily doses of 400-600 mg for the treatment of severe endogenous depression in a hospital setting [10]. Note, however, that such promising possibilities for the use of venlafaxine (both in outpatient practice and in the hospital) are associated with the need for accurate dose titration. However, this feature of the antidepressant may also benefit it, if we take into account the long experience of practicing psychiatrists with TCAs. Indeed, when using these fairly frequently used thymoanaleptics, one almost always has to resort to dose selection. And although this procedure takes time, it has already become familiar to both psychiatrists and their patients and is often considered an important stage of psychopharmacotherapy. Another issue with the mechanism of action of venlafaxine is the need to take into account the dose-related nature of side effects. Obviously, in low and medium doses of this antidepressant, the adverse effects characteristic of SSRIs will prevail: nausea, loss of appetite, vomiting, yawning, ejaculation/orgasm disorders, impotence, etc. (see table). It should be noted, however, that the frequency of these adverse events is not so high, with the possible exception of nausea. In high doses, side effects associated with an increase in the content of norepinephrine in the central nervous system will prevail: increased blood pressure (BP), tachycardia, dry mouth, insomnia, nervousness, agitation. In any case, it has been established that increased diastolic blood pressure (according to triple measurements, indicating that the level of 89 mm Hg is exceeded by at least 10 mm Hg from the initial level) is observed in 3% of patients receiving the drug in dose less than 100 mg/day, 5% at a dosage of 101-200 mg/day, 7% at a dose of 201-300 mg/day and 13% at a dosage exceeding 300 mg/day [11]. Moreover, the average level of blood pressure rise reaches 10-15 mm Hg. Art. Cases of the development of sinus tachycardia, which is a regular sinus rhythm with a heart rate of 100-180 beats/min, have also been reported while taking high doses of this drug, which is considered one of the most common and potentially dangerous side effects, especially in patients with coronary artery disease who are not receiving therapy β-blockers The latter can effectively stop not only sinus tachycardia, but also increased blood pressure. [12]. The most common side effects of venlafaxine, noted when taking it more often than when using placebo, during clinical trials of the drug (https://www.librarium.ru/showarticle.php?id=8093)
| Side effects | Venlafaxine (n=1033), % | Placebo (n=609), % |
| Body as a whole | ||
| asthenia | 12 | 6 |
| chills | 3 | — |
| The cardiovascular system | ||
| increased arterial | 2 | — |
| pressure/hypertension | ||
| tachycardia | 2 | — |
| Leather | ||
| sweating | 12 | 3 |
| Gastrointestinal tract | ||
| nausea | 37 | 11 |
| constipation | 15 | 7 |
| anorexia | 11 | 2 |
| vomit | 6 | 2 |
| Nervous system | ||
| drowsiness | 23 | 9 |
| dry mouth | 22 | 11 |
| dizziness | 19 | 7 |
| insomnia | 18 | 10 |
| nervousness | 13 | 6 |
| tremor | 5 | 1 |
| agitation | 2 | — |
| Respiratory system | ||
| yawn | 3 | — |
| Sense organs | ||
| blurred vision | 6 | 2 |
| perversion of taste | 2 | — |
| tinnitus | 2 | — |
| mydriasis | 2 | — |
| Genitourinary system | ||
| ejaculation/orgasm disorder | 12 | — |
| impotence | 6 | — |
| urinary disturbance | 2 | — |
Finally, a certain inconvenience for practicing physicians may be the fact that the “duality” of the mechanism of action of venlafaxine makes it very difficult to determine whether it belongs to thymoanaleptics with stimulating or sedative action.
Meanwhile, this scheme (despite its rather controversial nature) enjoys some popularity both abroad and among domestic psychiatrists. In particular, the famous American psychopharmacologist S. Stahl [1] describes these effects as secondary pharmacological properties of antidepressants, which can be realized in the form of both direct therapeutic effects and side effects, often not only masking positive dynamics, but also preventing such dynamics. The classification under consideration is also used by the English author S. Bazire [13], who mentions the activating and sedative effects of antidepressants when detailing their side effects. Finally, in Russian practice there is an extremely widespread opinion that the preferred target of the psychopharmacological effects of stimulant antidepressants is depression with a predominance of the phenomena of ideational and motor inhibition, and the preferred target of sedative antidepressants is anxious depression [8, 14]. Returning to venlafaxine, we point out that due to the complexity of the problem under consideration, some domestic psychopharmacologists classify this drug as an antidepressant with a balanced effect [2]. Meanwhile, analysis of the side effects of the drug (see table) allows us to clarify that, at least within the recommended therapeutic range of daily doses (75-375 mg), the sedative properties of the thymoanaleptic predominate. This is also evidenced by the possibility of using venlafaxine in the dosages under consideration for the treatment of anxiety-phobic disorders [5]. Finally, further studies are required to possibly re-evaluate the properties of the drug at higher daily doses. Concluding the characterization of the properties of venlafaxine, we note that at the time of writing this article, this antidepressant is available in the pharmacy chain in the form of various generics. One of them is Ephevelon. This drug is distinguished by improvements to make it easier to take the drug (special Opadry film coating), as well as the availability of data on its bioequivalence to the original antidepressant (Effexor). In particular, in work carried out in Canada (Montreal, Quebec), in April 2003, by the MDS Pharma Services research center, it was shown that Efevelon at a dose of 37.5 mg is completely equivalent to the corresponding dosage of Effexor (Fig. 4). The presented data opens up wide possibilities for the use of Efevelon in outpatient and inpatient practice.
Special instructions for the use of Venlafaxine
In patients with depression, the likelihood of suicide attempts should be considered before starting any therapy. Therefore, to reduce the risk of overdose, the initial dose of the drug should be as low as possible, and the patient should be under medical supervision. Aggressive behavior of the patient has been reported during the use of venlafaxine (especially at the beginning of the course of treatment and after discontinuation of the drug). The use of venlafaxine is associated with the development of psychomotor agitation, which is characterized by subjectively unpleasant restlessness with a need to move. Most often this occurs during the first weeks of treatment. If such symptoms occur, the dose should not be increased, so it is necessary to decide whether it is advisable to continue taking venlafaxine. In patients with mood disorders, hypomanic or manic states may occur when treated with antidepressants, including venlafaxine. Velaxin should be prescribed with caution to patients with a history of mania. These patients require medical supervision. Velaxin should be prescribed with caution to patients with a history of epileptic seizures. If epileptic seizures occur, treatment must be stopped. The patient should be warned about the need to immediately consult a doctor if a skin rash, elements of urticaria or other allergic reactions occur. In some patients, during the period of use of venlafaxine, a dose-dependent increase in blood pressure is possible, and therefore it is recommended to regularly monitor blood pressure, especially during the period of dose adjustment or increase. An increase in heart rate is possible, especially when taken in high doses. In this case, medical supervision of the patient's condition is necessary. Occasionally, orthostatic hypotension was observed during use of the drug. Patients, especially the elderly, should be warned about the possibility of dizziness. Venlafaxine may increase the risk of bleeding into the skin and mucous membranes in patients predisposed to these conditions. Patients should be warned about this and advised to exercise caution while using the drug. During the use of venlafaxine, especially in conditions of dehydration or decreased blood volume (including in elderly patients and in patients taking diuretics), hyponatremia and/or syndrome of insufficient secretion of antidiuretic hormone is possible. During the period of use of the drug, mydriasis may occur, and therefore it is recommended to monitor intraocular pressure in patients with a tendency to increase it, as well as with angle-closure glaucoma. When treating patients with impaired renal or liver function, caution and careful medical monitoring of the patient's condition is necessary (dose reduction is possible). In patients who have recently suffered a myocardial infarction and with signs of decompensated heart failure, the drug should be prescribed with caution under constant medical supervision. The safety and effectiveness of the combined use of venlafaxine and drugs used for weight loss, including phentermine, have not been established, so their simultaneous use is not recommended. With prolonged use of the drug, it is advisable to monitor the level of cholesterol in the blood serum. After stopping the use of venlafaxine, especially abruptly, withdrawal syndrome often occurs. The risk of developing withdrawal syndrome depends on the duration of treatment, the dose used, and the rate at which it is reduced. With withdrawal syndrome, dizziness, paresthesia, sleep disturbance, agitation, anxiety, nausea, vomiting, tremor, sweating, headache, diarrhea, tachycardia, and emotional disorders appear. These symptoms are usually observed in the first days after discontinuation of the drug and disappear on their own within 2 weeks. Therefore, the drug should be discontinued gradually, reducing the dose of venlafaxine gradually over several weeks or months, depending on the patient's condition. Venlafaxine does not cause the development of symptoms of tolerance or dependence. Despite this, as with other CNS-acting drugs, patients should be monitored for signs of venlafaxine abuse (especially patients with a history of such problems). While using venlafaxine, women of reproductive age should use adequate methods of contraception. Venlafaxine may adversely affect the ability to drive vehicles and operate potentially dangerous machinery. Therefore, doses at which driving vehicles and working with machinery are possible are determined for each patient individually.
INSTRUCTIONS for medical use of the drug VELAXIN® (VELAXIN®)
Registration number: LS 000030
Trade name: VELAXIN®
INN: venlafaxine
Dosage form: extended-release capsules
COMPOSITION: active substance: each capsule contains 75 mg and 150 mg of venlafaxine (in the form of venlafaxine hydrochloride). Excipients: MCC - 56/112 mg; sodium chloride - 46/92 mg; ethylcellulose - 17.69/35.38 mg; talc - 5.85/11.7 mg; dimethicone - 3.05/6.09 mg; potassium chloride - 2.41/4.81 mg; copovidone - 1.77/3.54 mg; colloidal silicon dioxide anhydrous - 1/2 mg; xanthan gum - 0.31/0.63 mg; iron oxide yellow - 0.16/0.32 mg
Composition of the gelatin capsule: titanium dioxide - 1/1%; iron oxide red - 0.47/0.47%; iron oxide yellow - 0.45/0.45%; gelatin - up to 100/100%
DESCRIPTION OF DOSAGE FORM
Capsules, 75 mg: hard gelatin self-closing capsules, with a colorless, transparent base and an orange-brown cap, containing a mixture of white and yellow pellets, odorless or almost odorless.
Capsules, 150 mg: hard gelatin self-closing capsules, with a colorless, transparent base and an orange-brown cap, containing a mixture of white and yellow pellets, odorless or almost odorless.
PHARMACEUTICAL GROUP(S): Antidepressant.
ATX CODE: N06AX16.
PHARMACODYNAMICS
Venlafaxine is an antidepressant. Based on its chemical structure, it cannot be classified into any known class of antidepressants (tricyclic, tetracyclic or others). It has two active enantiomeric racemic forms.
The antidepressant effect of venlafaxine is associated with increased neurotransmitter activity in the central nervous system. Venlafaxine and its main metabolite O-desmethylvenlafaxine (ODV) are potent serotonin and norepinephrine reuptake inhibitors and weakly inhibit neuronal dopamine reuptake. Venlafaxine and EDV are equally effective in inhibiting the reuptake of neurotransmitters. Venlafaxine and EDV reduce beta-adrenergic reactions.
Venlafaxine has no affinity for muscarinic, cholinergic, histamine H1- and α1-adrenergic receptors in the brain. Venlafaxine does not inhibit MAO activity. Has no affinity for opiate, benzodiazepine, phencyclidine, or N-methyl-D-aspartate (NMDA) receptors.
PHARMACOKINETICS
After taking Velaxin® extended-release capsules, Cmax of venlafaxine and EDV (main metabolite) in plasma are achieved within (6.0±1.5) and (8.8±2.2) hours, respectively. The rate of absorption of venlafaxine from extended-release capsules is lower than the rate of its elimination. Therefore, T1/2 of venlafaxine after the administration of Velaxin® in the form of extended-release capsules - (15±6) hours - is actually T1/2 of absorption rather than T1/2 of distribution - (5±2) hours - which is noted after the administration of the drug Velaxin ® in tablet form.
The binding of venlafaxine and EDV to plasma proteins is 27 and 30%, respectively. EDV and other metabolites, as well as unmetabolized venlafaxine, are excreted by the kidneys. With repeated administration of venlafaxine Css and EDV are achieved within 3 days. In the range of daily doses of 75–450 mg, venlafaxine and EDV have linear kinetics. After taking the drug with food, Tmax in the blood plasma increases by 20–30 minutes, but the values of Cmax and absorption do not change.
In patients with liver cirrhosis, plasma concentrations of venlafaxine and EDV are increased, and their elimination rate is reduced. In moderate or severe renal failure, the total clearance of venlafaxine and EDV is reduced, and T1/2 increases. A decrease in total clearance is mainly observed in patients with creatinine Cl below 30 ml/min.
The age and gender of the patient do not affect the pharmacokinetics of the drug.
INDICATIONS
Depression (including in the presence of anxiety), treatment and relapse prevention.
CONTRAINDICATIONS
- hypersensitivity to any component of the drug;
- simultaneous use of MAO inhibitors (see also “Interaction”);
- severe renal and/or liver dysfunction (glomerular filtration rate (GFR) less than 10 ml/min, PT more than 18 s);
- age under 18 years (safety and effectiveness for this age group have not been proven);
- pregnancy or suspected pregnancy;
- lactation period (there is insufficient data from controlled studies).
With caution: recent myocardial infarction, unstable angina, heart failure, coronary artery disease, ECG changes, incl. prolongation of the QT interval, electrolyte imbalance, arterial hypertension, tachycardia, history of seizures, intraocular hypertension, angle-closure glaucoma, history of manic states, predisposition to bleeding from the skin and mucous membranes, initially reduced body weight.
USE IN PREGNANCY AND BREAST-FEEDING
The safety of venlafaxine during pregnancy has not been proven, so use during pregnancy (or intended pregnancy) is only possible if the potential benefit to the mother outweighs the possible risk to the fetus. Women of childbearing age should be warned about this before starting treatment and should immediately consult a doctor if they become pregnant or plan to become pregnant during treatment with the drug.
Venlafaxine and EDV are excreted into breast milk. The safety of these substances for newborns has not been proven, so taking venlafaxine during breastfeeding is not recommended. If it is necessary to take the drug during lactation, the issue of stopping breastfeeding should be decided. If maternal treatment was completed shortly before delivery, the newborn may experience drug withdrawal symptoms.
METHOD OF APPLICATION AND DOSES
Inside, during meals. Each capsule should be swallowed whole with liquid. Capsules should not be divided, crushed, chewed, or placed in water. The daily dose should be taken at one time (morning or evening), each time at approximately the same time.
Depression. The recommended starting dose is 75 mg once a day.
If, in the opinion of the doctor, a higher dose is necessary (major depressive disorder or other conditions requiring hospital treatment), you can immediately prescribe 150 mg 1 time per day. Subsequently, the daily dose can be increased by 75 mg at intervals of 2 weeks or more (but not more often than after 4 days) until the desired therapeutic effect is achieved. The maximum daily dose is 350 mg.
After achieving the required therapeutic effect, the daily dose can be gradually reduced to the minimum effective level.
Maintenance therapy and relapse prevention. Treatment for depression should continue for at least 6 months. Stabilization therapy, as well as therapy to prevent relapses or new episodes of depression, usually use doses that have been demonstrated to be effective. The doctor should regularly (at least once every 3 months) monitor the effectiveness of long-term therapy with Velaxin®.
Transfer of patients from Velaxin® tablets. Patients taking Velaxin® in the form of tablets can be switched to taking the drug in the form of extended-release capsules, with an equivalent dose prescribed once a day. However, individual dosage adjustments may be required.
Kidney failure. In case of mild renal failure (GFR more than 30 ml/min), no dosage adjustment is required. For moderate renal failure (GFR 10–30 ml/min), the dose should be reduced by 50%. Due to the prolongation of T1/2 of venlafaxine and EDV, such patients should take the entire dose once a day. It is not recommended to use venlafaxine in severe renal failure (GFR less than 10 ml/min), since there are no reliable data on such therapy. Patients on hemodialysis may receive 50% of the usual daily dose of venlafaxine after completion of hemodialysis.
Liver failure. In case of mild liver failure (PT less than 14 s), no adjustment of the dosage regimen is required. In case of moderate liver failure (PT 14 to 18 s), the dose should be reduced by 50%. The use of venlafaxine in severe hepatic impairment is not recommended as reliable data on such therapy are lacking.
Elderly patients. The elderly age of the patient itself does not require a dose change, however (as with the prescription of other drugs) caution is required when treating elderly patients, for example due to the possibility of impaired renal function. The lowest effective dose should be used. When increasing the dose, the patient should be under close medical supervision.
Children and adolescents (under 18 years of age). The safety and effectiveness of venlafaxine in children and adolescents under 18 years of age have not been established.
Discontinuation of the drug Velaxin®. As with treatment with other antidepressants, abrupt discontinuation of venlafaxine (especially high doses) may cause symptoms and "Special Instructions"). Therefore, before completely discontinuing the drug, a gradual dose reduction is recommended. If high doses have been used for more than 6 weeks, it is recommended to reduce doses for at least 2 weeks. The length of time required to reduce the dose depends on the dose size, duration of therapy, and patient reactions.
SIDE EFFECTS
Most of the side effects listed below are dose dependent. With long-term treatment, the severity and frequency of most of these effects decreases, and there is no need to discontinue therapy.
In order of decreasing frequency: often - <1/10 and >1/100; uncommon - <1/100 and >1/1000; rarely - <1/1000; very rarely - <1/10000.
General symptoms: weakness, fatigue, headache, abdominal pain, chills, fever.
From the gastrointestinal tract: loss of appetite, constipation, nausea, vomiting, dry mouth; infrequently - bruxism, reversible increase in the activity of liver enzymes; rarely - gastrointestinal bleeding; very rarely - pancreatitis.
From the nervous system: dizziness, insomnia, agitation, drowsiness; often - unusual dreams, anxiety, confusion, increased muscle tone, paresthesia, tremor; infrequently - apathy, hallucinations, myoclonus; rarely - ataxia, speech disorders, incl. dysarthria, mania or hypomania (see “Special Instructions”), manifestations resembling neuroleptic malignant syndrome, seizures (see “Special Instructions”), serotonergic syndrome; very rarely - delirium, extrapyramidal disorders, incl. dyskinesia and dystonia, tardive dyskinesia, psychomotor agitation/akathisia (see “Special Instructions”).
From the cardiovascular system: arterial hypertension, dilation of blood vessels (flushes), rapid heartbeat; uncommon - orthostatic hypotension, fainting, tachycardia; very rarely - ari, prolongation of the QT interval, ventricular tachycardia, ventricular fibrillation.
From the senses: disturbances of accommodation, mydriasis, blurred vision, tinnitus; infrequently - disturbance of taste.
From the hematopoietic system: infrequently - hemorrhages in the skin (ecchymosis) and mucous membranes; rarely - thrombocytopenia, prolongation of bleeding time; very rarely - agranulocytosis, aplastic anemia, neutropenia, pancytopenia.
From the skin: sweating, itching and rash; uncommon - photosensitivity reactions, angioedema, maculopapular rash, urticaria; rarely - alopecia, erythema multiforme, Stevens-Johnson syndrome.
From the genitourinary system: disorders of ejaculation, erection, anorgasmia; uncommon - decreased libido, menstrual irregularities, menorrhagia, urinary retention; rarely - galactorrhea.
Metabolism: increased serum cholesterol levels, decreased body weight; uncommon - hyponatremia, syndrome of insufficient ADH secretion, abnormal liver function tests; rarely - hepatitis; very rarely - increased prolactin levels.
Musculoskeletal system: arthralgia, myalgia; infrequently - muscle spasm; very rarely - rhabdomyolysis.
The following side effects have been observed in children: abdominal pain, chest pain, tachycardia, food refusal, weight loss, constipation, nausea, ecchymosis, epistaxis, mydriasis, myalgia, dizziness, emotional lability, tremor, hostility and suicidal ideation.
After abrupt discontinuation of venlafaxine or a reduction in its dose, the following may be observed: fatigue, drowsiness, headache, nausea, vomiting, anorexia, dry mouth, dizziness, diarrhea, insomnia, restlessness, anxiety, disorientation, hypomania, paresthesia, sweating. These symptoms are usually mild and go away without treatment. Because these symptoms are likely to occur, it is important to gradually reduce the dose of the drug (as with any antidepressant), especially after taking high doses. The length of the period required to reduce the dose depends on the dose size, duration of therapy, as well as the individual sensitivity of the patient.
INTERACTION
The simultaneous use of MAO inhibitors and venlafaxine is contraindicated. Taking Velaxin® can be started no less than 14 days after the end of therapy with MAO inhibitors. If a reversible MAO inhibitor (moclobemide) was used, this interval may be shorter (24 hours). Therapy with MAO inhibitors can be started no less than 7 days after discontinuation of Velaxin®.
Concomitant use of venlafaxine with lithium may increase the level of the latter.
When used simultaneously with imipramine, the pharmacokinetics of venlafaxine and EDV do not change. At the same time, their simultaneous use enhances the effects of desipramine, the main metabolite of imipramine, and its other metabolite, 2-OH-imipramine, although the clinical significance of this phenomenon is unknown.
Haloperidol: Concomitant use increases haloperidol blood levels and enhances its effects.
When used simultaneously with diazepam, the pharmacokinetics of the drugs and their main metabolites do not change significantly. There was also no effect on the psychomotor and psychometric effects of diazepam.
When used simultaneously with clozapine, an increase in its level in the blood plasma and the development of side effects (for example, seizures) may be observed.
When used simultaneously with risperidone (despite the increase in AUC of risperidone), the pharmacokinetics of the sum of the active components (risperidone and its active metabolite) does not change significantly.
The decrease in mental and motor activity under the influence of alcohol did not increase after taking venlafaxine. Despite this, as in the case of taking other drugs that affect the central nervous system, the consumption of alcoholic beverages is not recommended during venlafaxine therapy.
While taking venlafaxine, special caution should be exercised during electroconvulsive therapy, because There is no experience with the use of venlafaxine in these conditions.
Drugs metabolized by cytochrome P450 isoenzymes: the cytochrome P450 enzyme CYP2D6 converts venlafaxine to the active metabolite EDV. Unlike many other antidepressants, the dose of venlafaxine does not need to be reduced when coadministered with drugs that inhibit CYP2D6 activity, or in patients with a genetically determined decrease in CYP2D6 activity, since the total concentration of venlafaxine and EDV will not change.
The main route of elimination of venlafaxine involves metabolism by CYP2D6 and CYP3A4; therefore, special caution should be exercised when prescribing venlafaxine in combination with drugs that inhibit both of these enzymes. Such drug interactions have not yet been studied.
Venlafaxine is a relatively weak inhibitor of CYP2D6 and does not suppress the activity of the CYP1A2, CYP2C9 and CYP3A4 isoenzymes; therefore, it should not be expected to interact with other drugs that are metabolized by these liver enzymes.
Cimetidine inhibits the first-pass metabolism of venlafaxine and does not affect the pharmacokinetics of EDV. In most patients, only a slight increase in the overall pharmacological activity of venlafaxine and EDV is expected (more pronounced in elderly patients and with impaired liver function).
Clinical studies have not revealed clinically significant interactions of venlafaxine with antihypertensive (including beta-blockers, ACE inhibitors and diuretics) and antidiabetic drugs.
Drugs bound to plasma proteins: Plasma protein binding is 27% for venlafaxine and 30% for EFA, so drug interactions due to protein binding should not be expected.
When taken simultaneously with warfarin, the anticoagulant effect of the latter may be enhanced, while the PT is prolonged and the MHO increases.
When taken simultaneously with indinavir, the pharmacokinetics of indinavir changes (with a 28% decrease in AUC and a 36% decrease in Cmax), but the pharmacokinetics of venlafaxine and EDV do not change. However, the clinical significance of this effect is unknown.
OVERDOSE
Symptoms: ECG changes (prolongation of the QT interval, bundle branch block, expansion of the QRS complex), sinus or ventricular tachycardia, bradycardia, arterial hypotension, convulsive states, depression of consciousness (decreased level of wakefulness). Death has been reported in cases of overdose of venlafaxine when taken concomitantly with alcohol and/or other psychotropic drugs.
Treatment: symptomatic. Specific antidotes are unknown. Continuous monitoring of vital functions (respiration and circulation) is recommended. Prescribing activated carbon to reduce drug absorption. Inducing vomiting is not recommended due to the risk of aspiration. Venlafaxine and EDV are not eliminated by dialysis.
SPECIAL INSTRUCTIONS
Depression increases the risk of suicidal thoughts and suicide attempts. This risk persists until stable remission occurs. Therefore, patients should be under constant medical supervision and should be given only small quantities of the drug capsules to reduce the risk of possible abuse and/or overdose.
Velaxin® should not be used in the treatment of children and adolescents under 18 years of age. Increases in the likelihood of suicidal behavior (suicide attempt and suicidal ideation) and hostility in clinical trials were observed more often among children and adolescents receiving antidepressants compared with groups receiving placebo.
Aggressive behavior has been reported while taking venlafaxine (especially at the beginning of treatment and after discontinuation of the drug).
The use of venlafaxine may cause psychomotor restlessness, which clinically resembles akathisia, characterized by restlessness with a need to move, often combined with an inability to sit or stand still. This is most often observed during the first few weeks of treatment. If these symptoms occur, increasing the dose may have an adverse effect, and continued use of the drug should be considered.
Like all antidepressants, venlafaxine should be prescribed with caution to patients with a history of mania and/or hypomania, because the drug may cause an increase in their symptoms. In these cases, medical supervision is necessary.
Caution should be exercised when treating patients with a history of seizures. If convulsive seizures occur or their frequency increases, treatment with venlafaxine should be interrupted.
Like selective serotonin reuptake inhibitors, venlafaxine should be used with caution when used concomitantly with antipsychotic drugs, because Symptoms resembling neuroleptic malignant syndrome may develop.
Patients should be warned to seek immediate medical attention if rash, hives, or other allergic reactions occur.
Some patients experienced a dose-dependent increase in blood pressure while taking venlafaxine, and therefore regular blood pressure monitoring is recommended, especially at the beginning of treatment or when the dose is increased.
Isolated cases of orthostatic hypotension have been described while taking venlafaxine. Patients, especially the elderly, should be warned about the possibility of dizziness and impaired balance.
Venlafaxine may cause an increase in heart rate, especially at high doses. Particular caution should be exercised when prescribing the drug to patients with conditions that may be aggravated by an increase in heart rate.
There are insufficient studies of the use of venlafaxine in patients who have recently suffered a myocardial infarction or suffering from decompensated heart failure, so this drug should be used with caution in these patients.
Like other serotonin reuptake inhibitors, venlafaxine may increase the risk of bleeding into the skin and mucous membranes, so caution is required when treating patients predisposed to bleeding.
While taking venlafaxine, especially in conditions of dehydration or decreased blood volume (including in elderly patients and patients taking diuretics), hyponatremia and/or syndrome of insufficient ADH secretion may occur.
Cases of mydriasis have been reported while taking venlafaxine, so patients with a predisposition to increased IOP or those at risk of angle-closure glaucoma require careful medical monitoring.
In case of renal and liver failure, special caution is required. In some cases, a dose reduction is required (see “Dosage and Administration”).
Safety and effectiveness of using venlafaxine with drugs that reduce body weight, incl. phentermine have not been established, so their simultaneous use (as well as the use of venlafaxine as monotherapy for weight loss) is not recommended. Clinically significant increases in serum cholesterol levels have been observed in some patients receiving venlafaxine for at least 4 months. Therefore, when taking the drug for a long time, it is advisable to monitor serum cholesterol levels.
After stopping the drug, especially abruptly, symptoms o) often occur. The risk of withdrawal symptoms may depend on several factors, including: duration of the course and dose, as well as the rate of dose reduction. Withdrawal symptoms such as dizziness, sensory disturbances (including paresthesia and electrical sensation), sleep disturbances (including insomnia and unusual dreams), agitation or anxiety, nausea and/or vomiting, tremors, sweating , headache, diarrhea, rapid or increased heart rate, and emotional instability are usually mild to moderate in severity, but may be severe in some patients. They are usually observed in the first days after discontinuation of the drug, although there have been isolated reports of such symptoms in patients who accidentally missed a dose. Usually these phenomena resolve on their own within 2 weeks; however, in some patients they may be longer lasting (2–3 months or more). Therefore, before discontinuing venlafaxine, it is recommended to gradually reduce its dose over several weeks or months, depending on the patient's condition (see "Dosage and Administration").
Impact on the ability to drive vehicles and operate machinery. It should be taken into account that any drug therapy with psychoactive drugs may reduce the ability to make judgments, think or perform motor functions. The patient should be warned about this before starting treatment. If such effects occur, the degree and duration of restrictions should be determined by a physician.
RELEASE FORM
Long-acting capsules. 10 or 14 caps. in a blister made of PVC/PVDC/aluminum foil. 2 blisters of 14 caps. or 3 blisters of 10 caps. cardboard pack.
STORAGE CONDITIONS. In a dry place, at temperatures below 30°C.
Keep out of the reach of children.
BEST BEFORE DATE. 5 years.
MANUFACTURER
CJSC "EGIS Pharmaceutical Plant". 1106, Budapest, st. Keresturi, 30-38, Hungary.
Tel.: (36 1) 803-55-55; fax: (36 1) 803-55-29.
Representative office of JSC "EGIS Pharmaceutical Plant" (Hungary) in Moscow. 121108, Moscow, st. Ivana Franko, 8.
Tel..
CONDITIONS OF VACATION FROM PHARMACIES
On prescription.
Drug interactions Venlafaxine
The use of venlafaxine in combination with MAO inhibitors is contraindicated: tremor, myoclonus, sweating, nausea, vomiting, flushing, dizziness, fever, seizures, and death may occur. The use of venlafaxine can be started no earlier than 14 days after the end of MAO inhibitor therapy. If a reversible MAO inhibitor is used, this interval may be shorter (24 hours). After discontinuation of venlafaxine, a break of at least 7 days should be taken before starting therapy with MAO inhibitors. Particular caution is required when using venlafaxine with drugs that affect the central nervous system. The mutual influence of venlafaxine and the following drugs should be taken into account: Lithium: there are reports of interaction between lithium and venlafaxine, as a result of which the level of lithium in the blood increases. Imipramine: the pharmacokinetics of venlafaxine and its metabolite EDV do not change, so a dose reduction of venlafaxine is not required when these drugs are used in combination. Haloperidol: its effect may be enhanced. Diazepam: the pharmacokinetics of the drugs and their main metabolites do not change significantly. Clozapine: an increase in the level of clozapine in the blood and the development of its side effects (for example, epileptic seizures) were noted. Risperidone: with the simultaneous use of these drugs (despite the increase in the AUC of risperidone), the pharmacokinetics of the sum of the active components (risperidone and its active metabolite) does not change significantly. Alcohol: depression of psychomotor activity under the influence of alcohol does not increase after taking venlafaxine, but during its use the consumption of alcoholic beverages is not recommended. Electroconvulsive therapy: when conducting electroconvulsive therapy while taking selective serotonin reuptake inhibitors, an increase in the duration of epileptic activity was noted. Caution must be exercised and careful medical monitoring of the patient's condition must be ensured when this type of therapy is combined with the use of venlafaxine. Drugs metabolized by cytochrome P450 isoenzymes : the CYP 2D6 enzyme of the cytochrome P450 system converts venlafaxine into the active metabolite EDV. Unlike many other antidepressants, the dose of venlafaxine does not need to be reduced when used once with drugs that inhibit CYP 2D6 activity, or in patients with a genetically determined decrease in CYP 2D6 activity, since the total concentration of the active substance and metabolite (venlafaxine and ODV) does not change. The main route of elimination of venlafaxine involves metabolism with the participation of CYP 2D6 and CYP 3A4, so special caution should be exercised when prescribing venlafaxine in combination with drugs that inhibit both of these enzymes. Venlafaxine is a relatively weak inhibitor of CYP 2D6 and does not inhibit the activity of CYP 1A2, CYP 2C9 and CYP 3A4 isoenzymes; therefore, its interaction with other drugs in the metabolism of which these liver enzymes are involved should not be expected. Cimetidine: inhibits the metabolism of venlafaxine during its initial passage through the liver, but does not have a significant effect on its conversion to EDV or the rate of elimination of EDV, the concentration of which in the circulating blood is much higher. Therefore, there is no need to change the dose of venlafaxine and cimetidine when used in combination. This interaction may be more pronounced in elderly patients or with impaired liver function, therefore, in such cases, the combined use of cimetidine and venlafaxine requires medical supervision. Antihypertensive and antidiabetic agents: no clinically significant interactions of venlafaxine with antihypertensive (including beta-adrenergic receptor blockers, ACE inhibitors and diuretics) and hypoglycemic agents have been identified. Drugs that bind to plasma proteins: plasma protein binding is 27% for venlafaxine and 30% for EDV. Therefore, interactions due to their binding to proteins should not be expected. Warfarin: the anticoagulant effect of the latter may be enhanced; at the same time, prothrombin time increases. Indinavir: When used concomitantly with this drug, the pharmacokinetics of indinavir changes (with a 28% decrease in AUC and a 36% decrease in maximum concentration).
results
During the prescribed 56-day course of treatment with Velaxin, 31 (96.9%) people were recognized as responders, of which a “minor” effect of treatment was observed in 1 (3.1%) patient, a “moderate” effect in 3 (9.4 %), “good” - in 2 (6.25%), and 25 (78.1%) patients showed a “significant” therapeutic effect. Thus, a decrease in the intensity of depressive disorders by 50% or more during treatment with Velaxin was found in the vast majority of cases - in 27 (84.4%) patients, as shown in Fig. 1.
Rice. 1. The degree of severity of the therapeutic effect of Velaxin for endogenous depression. The x-axis is the degree of reduction according to HAM-D,%; The y-axis is % of patients.
In general, the effectiveness of Velaxin, assessed on the 56th day of therapy, was quite high: the average total score of depression severity according to HAM-D was reduced by 85.9%. By the end of the 1st week of treatment with Velaxin, a positive therapeutic response to the drug was observed: the reduction in depression was at the level of a “minor” effect, but was approaching a 20% reduction in disorders, bordering on a “moderate” improvement. A clear “moderate” improvement (reduction in HAM-D score by 33.2%) was observed by the 14th day of treatment; between the 21st and 28th days of treatment, the therapeutic effect reached the “good” range with a decrease in HAM-D scores by 50% or more, and by the 6th week the effect of Velaxin treatment was already approaching the “significant” border (up to 76.7% reduction in the severity of depressive symptoms). In the subsequent 7-8 weeks of therapy, an undeniable “significant” improvement in the patients’ condition was detected (reduction of disorders by more than 80%), up to “recovery” (Fig. 2). In 20 out of 31 patients (64.5% of cases) who completed the course of treatment with Velaxin, depression was completely reduced and “entry” into remission was observed (their total HAM-D score became 6 or lower).
Rice. 2. The spectrum of therapeutic action of velaxin for endogenous depression (HAM-D score). Here and in Figs 3, 4 and 5 (in the last one - the right axis): on the ordinate - the average score as a percentage of the score before the start of therapy, on the x-axis - the day of therapy.
The severity of the condition, assessed by the CGI-S subscale, on average decreased during treatment with Velaxin from 4.7 to 1.6 points at the end of the study (from “significantly expressed” to less than “mildly expressed”, i.e., to the virtual absence of distress ). Moreover, a noticeable decrease in the severity of symptoms was noted in the period between the 7th and 21st days of treatment, when the intensity of the manifestations of depression consistently decreased on average to “moderately” and “weakly” expressed. From the 5th week of therapy, the severity of depressive disorders became “very weak”, and at the 7-8th week of course therapy there was a practical “exit” from depression with the “absence” of depressive symptoms (their average level of severity was 1.6 points). During the 56-day course of therapy, assessment of the degree of improvement in the depressive state on the CGI-I subscale showed a “deterioration” of the mental state (5th assessment level) in only 1 (3.1%) person, remained “unchanged” (4th assessment level) also in 1 (3.1%) patient, “minor improvement” (3rd level) - also in 1 (3.1%), “pronounced” improvement (2nd level) was observed in 4 (12 .6%), the remaining 25 (78.1%) patients showed a “significant” improvement (grade 1).
It was found that in the spectrum of antidepressant action of Velaxin, all 3 components of its psychotropic activity, in accordance with the final results of treatment, are presented to almost the same extent with a slight advantage in terms of anti-depressive action (see Fig. 2). Thus, the degree of reduction in the average total score of disorders on items 1-3 and 22-24 of HAM-D (reflecting the actual thymoleptic effect of the drug) was 88.2%, on items 7 and 8 (stimulating effect) - 83.7%, and on points 9 and 10 (anti-anxiety effect) - 85.1%. However, the implementation of all 3 components of the action of Velaxin over time was different and had its own characteristics. Thus, thymoleptic and especially anxiolytic effects were detected most quickly during treatment. They developed almost in parallel, reaching a level of reduction in the severity of disorders according to HAM-D by 32.8 and 37.1%, respectively, by the 14th day of therapy (“moderate” effect). At the same time, the stimulating effect of Velaxin was somewhat “lagged” compared to the anti-anxiety and anti-sadness effects, reaching similar values (“moderate” effect - reduction of disorders by 36.9%) only by the 21st day of the study.
Subsequently, in the period from the 21st to the 28th days of treatment, the thymoleptic and anti-anxiety components of the action in the spectrum of antidepressant activity of Velaxin leveled off and increased in rate of development to the range of a clear “good” effect (score reduction by 60.2 and 59. 2%). But already from the 5th week of treatment, the thymoleptic effect itself began to surpass the anxiolytic one in terms of the depth of reduction of disorders according to the corresponding HAM-D items: the thymoleptic effect appeared at the “significant” level already at the 6th week, and the anti-anxiety effect only after the 7th week course therapy. The formation of the stimulating effect was “lagged” in the degree of manifestation compared to the other two components of the action of Velaxin at 1 week, and its “significant” severity was determined only at the 8th week of treatment. And only at this stage of treatment, as already mentioned, the depth of the stimulating effect of Velaxin approximately coincided with the severity of the thymoleptic and anxiolytic effects.
In accordance with established data on the peculiarities of the implementation of individual components of antidepressant action in the spectrum of psychotropic activity of velaxin, its therapeutic effectiveness was analyzed depending on the syndromic type of depression, i.e., on the dominant affect that determines the picture of the depressive state (Fig. 3). It was found that with leading anxious affect, the reduction in the average total score on HAM-D was 85.5% by the 56th day of treatment; with a predominance of apatho-adynamic affect, the effectiveness of Velaxin was similar - the average total score on HAM-D decreased by 85.9%. The highest effectiveness of Velaxin was observed in the treatment of patients with a leading sad affect in the picture of depression - the reduction in the average total score on HAM-D was 91.1%. But with a relatively similar degree of reduction in depressive symptoms, differences were also noted in the dynamics of the implementation of the antidepressant effect of the drug. Thus, with leading anxious and melancholy affects, i.e. in patients with positive affectivity and the most typical manifestations of depression, the reduction of depressive symptoms proceeded at an equal pace, reaching 21.1% (with anxious depression) and 22.5% (with melancholy depression) already by the 7th day of therapy. Subsequently, the decrease in the average total score on HAM-D occurred more intensively and reached more than 50% reduction in depressive symptoms by the 28th day of treatment. When treating patients with negative affectivity (atypical apatho-adynamic depression) with Velaxin, improvement occurred more slowly. A reduction in the average total HAM-D score by 20% or more (“moderate” effect) occurred only in the 2-3rd week of therapy; and only by the 4th week a “good” effect of Velaxin was recorded (reduction of disorders by 61.3%). By the 7-8th week of treatment, the improvement in the condition was already “significant” (more than 80% reduction in disorders), it coincided in severity with the therapeutic effect of Velaxin for anxious depression and was somewhat “lag behind” the effect for melancholy depression.
Rice. 3. Dynamics of the effectiveness of Velaxin for different types of endogenous depression (HAM-D score).
Analysis of the effectiveness of Velaxin depending on the nosological affiliation of depression also revealed some features (Fig. 4): the lowest rate of decrease in the average total score on HAM-D by the end of the course of treatment was in patients with low-progressive schizophrenia, it was equal to 82.3%. These same patients also had the slowest rate of reduction in depressive disorders - by the 7th day it was only 15.2%, and a reduction of 50% or more (the limit of a “good” effect) was achieved only by the 28th day; A “significant” effect was detected in patients with low-progressive schizophrenia only after the 7th week of treatment with Velaxin. In patients with affective illness (MDP, cyclothymia), the reduction in the average total score on HAM-D at the end of course therapy was close in value (86.6%), and the rate of reduction in depressive symptoms was similar: by the 7th day this figure reached 18 .2%, and by the 4th week of therapy it was already 59.4% (“good” effect). The best treatment result was achieved in patients with postpsychotic depression and paroxysmal schizophrenia - 90.4% reduction in disorders on the 56th day of treatment. Despite the fact that by the end of the 1st week of the study, the rate of reduction in depressive symptoms reached gradations of “insignificant” improvement (19.2%), subsequently the reduction in depressive symptoms occurred more intensively than with MDP, demonstrating a “good” effect already at 14 days. 1st day of treatment (symptom reduction rate -53.9%), and by the 28th day it was already 76.5%, i.e. it was almost on the border of “significant”. However, it should be noted that in these patients the initial severity of depressive disorders was significantly lower, at the level of “moderate” severity, than in other, more “severe” depressions (23 points on HAM-D versus 31.3 points for affective illness and 31.6 for low-progressive schizophrenia).
Rice. 4. Antidepressant effect of Velaxin in different nosological groups of patients (HAM-D score).
All of the indicated patterns of development of the therapeutic effect of Velaxin indicate the absence of a direct dependence on the size of its daily dose. As can be seen from Fig. 5, the therapeutic effect began to appear and increase from the 3-4th week of treatment (reduction of depressive symptoms by 50% or more according to HAM-D), with an increase in the average daily dose to the maximum (182.1-198.2 mg per day) . But subsequently, despite stabilization and even a slight decrease in the achieved maximum average daily dose of Velaxin (up to 190.3 mg per day), the response to therapy continued to increase at a faster pace, to the level of “significant” improvement,
Rice. 5. The relationship between the therapeutic effect (HAM-D score) and the daily dose of Velaxin. On the left ordinate is the average daily dose of the drug (mg).
During the course of Velaxin therapy, 45 adverse events of various types were registered in 21 (65.6%) patients; in 5 they were single, and in 16 they were combined. The most common were mental and autonomic adverse events noted on the UKU scale; they occurred in 40% of patients. One patient withdrew from the study early (after 2 weeks of treatment) due to the development of acute affective-delusional psychosis, requiring a change in therapy. Neurological and other side effects occurred in only 8.9 and 11.1% of patients. The most common individual side effects observed were “excitement/anxiety” (in 15.5% of patients), decreased sleep duration and nausea (in 11.1%), tachycardia and hyperhidrosis (in 6.6%), sedation and constipation (in 4.4%). All other side effects occurred in isolated cases. The incidence of side effects during a course of treatment with Velaxin was highest in the 2nd week of treatment, when the average daily dose of the drug was insignificant (157.7 mg per day). The most common adverse events during this period were psychiatric and autonomic adverse events. But subsequently, despite increasing the average daily dose, the incidence of side effects gradually decreased. The exception was “other” side effects, the frequency of which practically remained at the same level until the end of treatment. These were mainly sexual dysfunctions, which developed according to an increase in the daily dose of Velaxin.
It should be noted that, in general, all adverse events were mild or approaching moderate severity in the first 2 weeks of treatment, and then their average severity as assessed by UKU decreased to a “mild” level, despite a gradual increase in the average daily doses of Velaxin. At the same time, mental side effects were initially the most severe: the average UKU severity score at 1–2 weeks of treatment was 1.9–2.0. However, during the further course of treatment, the severity of adverse mental symptoms decreased from the 3rd week. The severity of some other adverse events increased slightly compared to the initial one: if on the 2nd week of treatment their severity on average corresponded to the UKU “mild” degree (1 point), then later they reached 1.5 points, and at the same time their degree severity increased according to an increase in the average dose of Velaxin.
Venlafaxine overdose, symptoms and treatment
symptoms: ECG changes (increased QT , bundle branch block, expansion of the QRS ), sinus and ventricular tachycardia, bradycardia, hypotension, convulsions, impaired consciousness. In some cases, fatalities due to overdose have been reported when high doses of venlafaxine were taken concomitantly with alcohol and/or other psychotropic drugs. Treatment: there is no specific antidote. Gastric lavage and the use of activated carbon are indicated. Inducing vomiting is not recommended. It is necessary to ensure airway patency, adequate ventilation and oxygenation. Monitoring of ECG and vital body functions is recommended, as well as supportive and symptomatic therapy. In case of overdose, the possibility of the patient taking several psychotropic drugs simultaneously should be taken into account. Venlafaxine and EDV are not eliminated by dialysis.
List of pharmacies where you can buy Venlafaxine:
- Moscow
- Saint Petersburg