Pharmacodynamics and pharmacokinetics
Charozetta is intended for oral contraception. The effect of the drug is due to inhibition of ovulation and thickening of cervical mucus .
The use of this drug leads to a decrease in the concentration of estradiol to levels that are characteristic of the early follicular phase .
The medicine is rapidly absorbed and converted to the active metabolite etonogestrel . With regular use, maximum plasma concentration is achieved approximately 100 minutes after the next tablet. Bioavailability approximately 70%.
The drug preferentially binds to serum proteins ( albumin , globulin ).
The active substance is metabolized through hydroxylation and dehydrogenation , converting to the active metabolite etonogestrel , through which sulfate and glucuronide conjugates .
The drug is excreted primarily in urine and feces in the form of free steroids and conjugates .
Charozette® (Cerazette®)
If you have any of the following conditions or risk factors, you should carefully weigh the benefits and possible harms of using gestagens. This issue should be discussed with the patient before starting Charozetta®. In case of exacerbation of diseases, deterioration of the condition or the appearance of the first symptoms of the above-mentioned conditions or risk factors, the patient should immediately consult a doctor. The doctor should decide whether it is necessary to discontinue the drug Charozetta®.
— The risk of breast cancer increases with age. While using combined oral contraceptives, the risk that a woman will be diagnosed with breast cancer increases slightly. This increased risk gradually disappears over 10 years after stopping oral contraceptives and is not related to duration of use but depends on the woman's age at the time of combined oral contraceptive use. The expected number of cases of breast cancer diagnosed among 10,000 women who used combined oral contraceptives (within 10 years of stopping use), relative to women who never took them, over the same period, calculated for the corresponding age groups, is presented in the table below .
| Age group | Expected number of cases among women using combined oral contraceptives | Expected number of cases among women not using oral contraceptives |
| 16-19 years old | 4,5 | 4 |
| 20-24 years old | 17,5 | 16 |
| 25-29 years old | 48,7 | 44 |
| 30-34 years old | BY | 100 |
| 35-39 years old | 180 | 160 |
| 40-44 years old | 260 | 230 |
The risk in women using progestin-containing contraceptives, such as Charozetta®, may be similar to that of combined oral contraceptives. However, the data for progestin-containing contraceptives are not so clear. Compared with the lifetime risk of breast cancer, the increase in risk associated with combined oral contraceptives is small.
Breast cancer diagnosed in women using combined oral contraceptives tends to be less clinically advanced than cancer diagnosed in women who have never used combined oral contraceptives. The increased risk in women using combined oral contraceptives may be due to earlier diagnosis, biological effects of the drug, or a combination of these two factors.
— Since it is impossible to exclude the biological effect of gestagens on the development of liver cancer, an individual assessment of the benefit-risk ratio should be carried out when prescribing the drug to women with liver cancer.
— In case of acute or chronic liver dysfunction, a woman should contact a specialist for examination and consultation.
“If persistent hypertension develops while taking Charozetta®, as well as if antihypertensive therapy is ineffective with a significant increase in blood pressure, you should consider discontinuing Charozetta®.”
— Epidemiological studies have established an association between the use of combined oral contraceptives and an increased incidence of venous thromboembolism (VTE, deep vein thrombosis and pulmonary embolism). Although the clinical significance of these data for desogestrel as a contraceptive that does not contain an estrogen component is unknown, the use of Charozetta should be discontinued if thrombosis develops. Discontinuation of Charozetta® should be considered in case of prolonged immobilization associated with surgery or illness.
A woman with a history of thromboembolism should be informed of the possibility of recurrence.
- Although gestagens may affect peripheral insulin resistance and glucose tolerance, there is no evidence that there is a need to change the therapeutic regimen in diabetic patients using gestagen-containing oral contraceptives. However, women with diabetes should be closely monitored during the first months of using the drug.
- The use of Charozetta® leads to a decrease in serum estradiol levels to a level corresponding to the early follicular phase. It is currently unknown whether this decrease has any clinically significant effect on bone mineral density.
— Prevention of ectopic pregnancy with traditional gestagen-containing oral contraceptives is not as effective as when using combined oral contraceptives, since ovulation often occurs when using gestagen-containing contraceptives. Although Charozetta® effectively suppresses ovulation, in the case of amenorrhea or abdominal pain, ectopic pregnancy should be excluded in the differential diagnosis.
- In rare cases, chloasma has developed, especially in women with a history of chloasma during pregnancy: women with a predisposition to chloasma should avoid exposure to sunlight or ultraviolet radiation while using Charozetta®.
— During pregnancy and during the use of sex steroid hormones, the following conditions were noted, although their relationship with gestagens has not been definitively established: jaundice and/or skin itching associated with cholestasis; formation of gallstones; porphyria; systemic lupus erythematosus; hemolytic-uremic syndrome; Sydenham's chorea; herpes during pregnancy; hearing loss associated with otosclerosis; (hereditary) angioedema.
— The drug Charozetta® contains no more than 65 mg of lactose, so women with rare hereditary disorders associated with galactose intolerance, Lapp lactase deficiency, or glucose-galactose malabsorption. should refrain from taking the drug.
Medical examinations/consultations
Before prescribing the drug, a woman should carefully collect anamnesis and conduct a thorough gynecological examination to exclude pregnancy. Before prescribing the drug, the cause of menstrual irregularities, for example, oligomenorrhea and amenorrhea, should be established. The interval between control medical examinations is determined by the doctor in each individual case (the frequency of examinations is at least once a year). If the prescribed drug may affect a latent or existing disease, an appropriate schedule of follow-up medical examinations should be drawn up.
Despite regular use of Charozetta®, irregular bleeding may sometimes occur. If bleeding is very frequent and irregular, you should consider using another method of contraception. If the above symptoms are persistent, then in this case it is necessary to exclude organic pathology. Management of amenorrhea while using the drug depends on whether the tablets were taken as directed and may include a pregnancy test. In case of pregnancy, the drug should be discontinued.
Women should be informed that Charosette® does not protect against HIV infection (AIDS) or other sexually transmitted diseases.
Reduced efficiency
The effectiveness of Charozetta® may be reduced in case of missed tablets (see section "Dosage and Administration"), gastrointestinal disorders (see section "Dosage and Administration"), or in the case of concomitant therapy, which reduces the concentration of etonogestrel - active metabolite of desogestrel, in blood plasma (see section “Interaction with other drugs”).
Changes in the nature of menstruation
While using progestin-containing contraceptives, some women may experience vaginal bleeding more frequently or for a longer period of time, while for other women this bleeding may become less frequent or stop altogether. These changes are often the reason that a woman refuses this method of contraception or ceases to strictly follow the doctor's instructions. In detailed consultation with women who decide to start taking Charozetta®, the doctor should discuss the possibility of such changes in the nature of the menstrual cycle. Evaluation of vaginal bleeding should be based on clinical presentation and may include testing to rule out malignancy or pregnancy.
Follicle development
When taking all low-dose hormonal contraceptives, follicle development occurs; occasionally, the size of the follicle can reach sizes exceeding those in a normal cycle. In general, these enlarged follicles disappear spontaneously. This often occurs without symptoms; in some cases there is mild pain in the lower abdomen. Surgery is rarely required.
Laboratory research
Data obtained with combined oral contraceptives have shown that the use of hormonal contraceptives may affect the results of some laboratory tests, including biochemical parameters of liver, thyroid, adrenal and kidney function, serum levels of (transport) proteins, e.g. , which binds corticosteroids into lipid/lipoprotein fractions. indicators of carbohydrate metabolism and indicators of blood clotting and fibrinolysis. Usually these changes remain within normal limits. It is not known to what extent this also applies to progestin-containing contraceptives.
Side effects
Side effects when using Charozetta may be the following: headache , spotting, mood changes, nausea, acne , painful sensations in the mammary glands, weight changes, amenorrhea , decreased libido.
Less common manifestations are vaginitis , ovarian cysts , alopecia , discomfort when using contact lenses, dysmenorrhea , vomiting, and fatigue.
In rare cases, side effects such as rash, erythema nodosum and urticaria .
Instructions for use of Charozetta (Method and dosage)
The medicine must be taken one tablet a day, without missing a single dose. You need to do this at the same time for 28 days in the order written on the package. The instructions for Charozetta recommend taking the tablets with the required amount of liquid. You should start taking tablets from the next package immediately after the previous one is finished.
If hormonal contraceptives have not been used before, the instructions for using Charozetta provide for starting use on the first day of the menstrual cycle. Although it is possible to start the course in days 2-5, in this case it is recommended to use additional measures to prevent pregnancy during the first week.
When switching from combined hormonal contraceptives, the Charozetta course begins the day after the end of taking the previous drug or on the day of removal of the vaginal ring or transdermal patch . Additional contraception is not needed in this case.
When switching from a mini-pill, Charozette can be taken any day. gestagen-releasing intrauterine system was previously used , the first tablet of the drug is taken on the day of their removal. When using contraception in injection form, you switch to Charozetta on the day when the next injection was supposed to be given. After an abortion in the first trimester, you should start taking this medication immediately. Additional contraception is not needed in this case.
After an abortion in the second trimester, the start of the course of the drug is possible only after 21-28 days, as well as 6 weeks after birth. If the use of Charozetta is started later, additional measures are necessary during the first week to ensure reliable contraception. In this case, pregnancy should be excluded.
If a tablet is missed by less than 12 hours, it should be taken as soon as possible; the next dose will be taken at the usual time. If you miss a pill by more than 12 hours, you should take it as soon as possible, but use additional methods for reliable contraception over the next week.
For gastrointestinal disorders, it is also better to use additional methods of birth control.
Experience of practical use of the new gestagen contraceptive "Charozetta"
Introduction
Every year around the world, the number of women using hormonal methods of contraception increases, since the use of this method of family planning and birth control is the most effective and convenient to use.
Every year around the world, the number of women using hormonal methods of contraception increases, since the use of this method of family planning and birth control is the most effective and convenient to use.
Currently, more than 150 million women worldwide use hormonal contraceptives
. The most popular are combined oral contraceptives (COCs) containing low doses of estrogen and progestogen [1].
In recent years, the attitude of the Russian population towards the use of contraception, especially hormonal contraception, has changed. Thus, in our country over the past 10 years, the use of hormonal contraception has increased more than 5 times. It is generally accepted that hormonal contraception has a beneficial effect on a woman’s health, provides a therapeutic effect for various menstrual dysfunctions, endometrial hyperplastic processes, endometriosis, and fibrocystic mastopathy [2].
Therefore, at present, the first choice drugs for reliable protection against unwanted pregnancy are COCs with the minimum effective dose of their constituent components.
However, there is a category of women who need effective contraception, but for whom even minimal doses of estrogen are contraindicated.
An alternative for this group of women may be contraceptives containing progestogens only (PSP) or mini-pills.
PSPs are characterized by better tolerability (absence of estrogen-dependent adverse reactions), the possibility of use during lactation, since they do not affect the quantity and quality of breast milk, and the possibility of use in older women, as well as in smokers.
However, mini-pills have a number of disadvantages. First of all, they do not provide lasting suppression of ovulation, since their main contraceptive effect is due mainly to their effect on cervical mucus. Mini-pills also slow down the transport of eggs through the fallopian tubes, resulting in an increased risk of developing an ectopic pregnancy [4].
Progestogens used in modern PSPs are typically second generation and have residual androgenic activity and, therefore, may have androgen-dependent effects [5].
Therefore, a modern contraceptive drug must contain such a minimum dose of steroids that would be able to provide stable suppression of ovulation, and therefore reliable protection against pregnancy with a minimum number of side effects.
Currently, scientific research is aimed at developing such drugs, and one of the results of these studies was the desogestrel-containing contraceptive - Charozetta.
[7].
The main goal of developing the drug Charozetta was to obtain an oral contraceptive that does not contain estrogen, but which could permanently block ovulation and, therefore, would have the contraceptive reliability of COCs [6].
In large-scale clinical studies, it was shown that the Pearl index of the Charozetta drug was 0.14, which corresponds to that of the COC.
Each tablet of the drug contains 75 mcg of desogestrel, a highly selective progestogen that provides persistent suppression of ovulation, without a negative effect on metabolic processes. Therefore, Charozetta has greater contraceptive reliability and acceptability compared to traditional PSPs.
Thus, Charozetta may be the contraceptive of choice for the following categories of women:
– for those who have estrogen-dependent side effects;
– for those for whom the use of estrogens is contraindicated (in the presence of risk factors such as arterial hypertension, risk of thrombosis, smoking, late reproductive age);
– in the postpartum period for those who are breastfeeding.
Based on the above, the purpose of the study, conducted at the Scientific Center for Gynecology and Pregnancy of the Russian Academy of Medical Sciences, was to study the effectiveness and acceptability of the Charozetta PSP in healthy sexually active fertile women, including women in the postpartum period and breastfeeding.
Material and research methods
The study included 100 sexually active fertile women under 40 years of age (mean age 29.53±6.19 years). All patients had a regular menstrual cycle for the last 3 months or more. When entering the study, deviations were allowed in the health status of women that met the criteria of health class 1 adopted by WHO (1995).
In the study group, 17 out of 100 women were in the postpartum period and were breastfeeding.
All women were prescribed the drug "Charozetta" for contraceptive purposes. The drug was taken according to the following regimen: 1 tablet per day from the 1st day of the menstrual cycle in a continuous mode, patients (breastfeeding - no earlier than 4-6 weeks after birth). All participants were instructed to properly keep a menstrual diary, which included information about each cycle. The acceptability of the drug was determined based on an analysis of the registration of patient complaints, the frequency and nature of adverse reactions, and individual analysis of menograms over time.
We used a 90-day standard (WHO) interval to assess bleeding. The following WHO criteria were used to describe the nature of bloody discharge:
Bleeding (B) is any bloody discharge from the genital tract requiring the use of two or more tampons or pads per day.
Spotting (M) is any bloody discharge from the genital tract that requires the use of no more than 1 tampon or pad per day.
An episode of bleeding and spotting (B/M) – 1 or several consecutive days during which B/M is noted; each episode is limited from the next by the presence of “clean” days, when no bleeding is detected.
Amenorrhea is the absence of bleeding during a standard 90-day time interval.
Rare bleeding - 1 or 2 episodes of C/M during a 90-day interval.
Frequent bleeding – 6 or more episodes of C/M within a 90-day interval.
Prolonged bleeding - any episode of C/M lasting more than 14 days.
The study design included an in-depth clinical study of the drug "Charozetta" over 6 months of use - monthly visits to a gynecologist, with assessment of general well-being. The scope of the study included: analysis of data on somatic and obstetric-gynecological history, determination of weight-height coefficient, measurement of blood pressure, study of PAP smears, ultrasound examination of the pelvic organs.
Criteria for inclusion of patients in the study: age from 18 to 40 years, the woman’s readiness to use planned oral contraception, confirmed by informed consent. There are no contraindications to the use of hormonal contraception.
It is known that one of the main reasons for refusing to use any hormonal contraceptives - acyclic bleeding - is associated with insufficient awareness of patients about the mechanism of action of hormonal contraceptives. Therefore, we paid special attention to the issue of consulting.
Three patients dropped out of the study prematurely: in all cases, the reason for withdrawal was acyclic bleeding.
The results obtained and their discussion
Analyzed indicators: systolic and diastolic blood pressure (BP), body weight, pattern of bleeding after 3 and 6 months. The use of the drug "Charozetta" was compared using the nonparametric Friedman test.
While taking Charozetta PSP, not a single case of pregnancy has been registered. Thus, the results of our study showed that the contraceptive effectiveness of Charozetta is similar to that of COCs, which is a reflection of persistent inhibition of ovulation (Pearl index - 0.14).
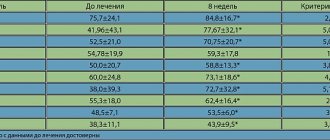
The results of the study confirmed the safety of the use of Charozetta in terms of its effect on certain indicators of the cardiovascular system. In all patients (100%) after 3 and 6 months of taking Charozetta, there was no increase in blood pressure levels (Fig. 1, 2).
Rice. 1. Systolic blood pressure in women taking Charozetta
Rice. 2. Diastolic blood pressure in women taking Charozetta
By the 6th month of taking the contraceptive, changes in body weight were noted in only 22% of those examined (1.5±0.5 kg), only 2% showed an increase in body weight of more than 2.5 kg. We did not detect any significant differences in body weight during the follow-up period.
Our results are consistent with the data of a number of studies, which also did not reveal changes in body weight over time [7]. In our opinion, the absence of changes in body weight is an extremely important property of the drug, since it has been established that when choosing any hormonal contraceptive, the prospect of weight gain causes a sharp rejection of this method in women.
Considering that there is no break in taking the drug, and therefore no regular cycles, the pattern of bleeding from the genital tract was less predictable than when taking COCs.
In order to compare the nature of bleeding while taking Charozette, we used the “standard time interval” (WHO, 1986) for their analysis. It should be emphasized that many studies use a 90-day time frame to assess bleeding [6]. The first standard time interval was from days 1 to 90, the second - from 91 to 180, respectively.
The nature of bleeding when using the drug is shown in Fig. 3. From the presented figure it is clear that there is great variability in changes in the menstrual cycle.
Rice. 3. Types of vaginal bleeding while taking Charozetta
Thus, in the first standard time interval, the number of women with rare (1-2 episodes) bleeding was 35%, 52% of women had 3-5 episodes of bleeding, which is normal, because Over a period of 90 days, women experience on average 3 to 5 menstruation (WHO, 1986).
It should be noted that only 9% of patients reported frequent bleeding.
Amenorrhea was observed in 4% of women, and 14% of patients reported prolonged (more than 14 days) episodes of bleeding.
The number of women with frequent bleeding (6 or more episodes) in the second standard time interval decreased significantly and amounted to 2.06%, their average duration was 3.03±1.7 days.
Prolonged bleeding was also rare and was observed only in 7.22% of women (p = 0.28). As can be seen in Figure 3, in the second standard time interval the number of women with amenorrhea significantly (p<0.00001) increased to 30.9%, which is consistent with data from international studies, where the authors also observed the development of amenorrhea in every third patient who used the drug "Charozette" [7].
When analyzing the average number of days of assessed bleeding, it was noted that during the first 90-day interval, their number ranged from 21.29 ± 13.96 days. Subsequently, the number of days tended to decrease and in the second interval amounted to 11.39±12.39 (p<0.00001).
When analyzing the number of days of bleeding requiring 2 pads or tampons per day, it was revealed that their average number in the first 90-day interval was 6.46±5.40, and in the second time interval – 2.36±3.43 days ( p<0.00001).
Thus, when using Charozetta PSP, short episodes of spotting are mainly observed, which are regarded as normal.
Prolonged spotting and spotting occurred less frequently, the number of which decreased significantly over time.
In general, we can say that changes in the nature of spotting in the direction of their reduction as the drug is taken are generally favorable and have virtually no effect on the woman’s quality of life.
In 8% of women using this drug, the presence of adaptation effects was noted.
All identified adverse reactions, as a rule, disappeared within the first 1–3 months. use of the drug and did not require its discontinuation. We believe that adverse reactions were a consequence of adaptation to the drug used and their frequency does not exceed that when taking placebo.
An analysis was made of the use of Charozetta in 17 women after childbirth who had no contraindications to its use. At the same time, 14 women were breastfeeding, 3 women were not breastfeeding. During the observation period, no pregnancies were registered.
No serious side effects were observed in this group of women. There was no evidence of any negative effect of the drug on the duration of lactation. The average duration of lactation was 4.6±1.9 months.
At the end of this study, 91.8% of women expressed satisfaction with taking the drug (Fig. 4), which is regarded by international standards as good acceptability of this contraceptive.
Rice. 4. Satisfaction with the drug “Charozetta” after 6 months of use (n=97)
Thus, the study allows us to consider the new PSP “Charozetta” as a promising method for preventing unwanted pregnancy in women of reproductive age, including as postpartum contraception.
conclusions
1. Charozetta is a reliable and acceptable method of preventing unplanned pregnancy in women of reproductive age. It can be considered that the effectiveness of the drug "Charozetta" is not inferior to that of COCs.
2. While taking the drug “Charozetta”, various types of bleeding are observed.
3. There is a decrease in the number of days of bleeding as the drug is taken.
4. 30% of women develop amenorrhea as they take Charozetta.
5. “Charozetta” does not affect the duration of lactation and the quality of breast milk and can be widely used in breastfeeding women.
6. The frequency of side effects while taking Charozetta is no higher than when taking placebo.
Thus, “Charozetta” is the only PSP at the moment that has the reliability of COC
.
When taking it, it is possible to achieve maximum contraceptive effectiveness with the lowest possible dose of hormones. Literature:
1. Newton JR //Humah Reprod. Update. – 1995. – vol.1. – N3. – P. 231–63.
2. Prilepskaya V.N. Gynecology. – 2003. – N2 – vol. 5. – P. 54–56.
3. Guillebaud J. //Contraception. Your questions answered. 2nd edn. Edinburgh: Churchill Livingstone, 1993.
4. McCann MF, Potter LS // Contraception – 1994. – 50 suppl. 1: Sl – 198.
5. Darney P. // Am. J. Med. – 1995/ – 98 suppl. 1 A: 104–1 OS.
6. Rice CF et al. //Hum.Reprod. – 1999 – N14. – P 982–5.
7. Collaborative Study group. //Eur. J. Contracept. Reprod. Health Care – 1998. – N3. – p. 169–78.
Interaction
No studies have been conducted on the interaction of the drug with other drugs. However, based on experimental observations, it is known that when combined with hydantoins , Carbamazepine , Oxcarbazepine , Troglitazone , Griseofulvin , barbiturates , Rifampicin , Rifabutin and Felbamate , vaginal bleeding and a decrease in the effectiveness of the contraceptive effect may occur. In this case, one of the drugs must be discontinued. If this is not possible, it is necessary to use an additional method of birth control throughout the entire course of treatment with one of these drugs and for a week after its completion. And when taking Rifampcin and within 28 days after the last use.
When using medications that induce liver enzymes, it is better to stop using Charozetta tablets and switch to non-hormonal methods of preventing unwanted pregnancy.
Taking activated carbon may reduce the effect of the drug. So with this combination it is recommended to resort to additional contraception.
Charozette® (Cerazette)
Before prescribing the drug, a woman should carefully collect anamnesis and conduct a thorough gynecological examination to exclude pregnancy. Before prescribing the drug, the cause of menstrual irregularities, for example, oligomenorrhea and amenorrhea, should be established. The interval between control medical examinations is determined by the doctor in each individual case (the frequency of examinations is at least once a year). If the prescribed drug may affect a latent or existing disease, an appropriate schedule of follow-up medical examinations should be drawn up.
Despite regular use of Charozetta®, irregular bleeding may sometimes occur. If bleeding is very frequent and irregular, you should consider using another method of contraception. If the above symptoms are persistent, then in this case it is necessary to exclude organic pathology. Management of amenorrhea while using the drug depends on whether the tablets are taken as directed and may include a pregnancy test. In case of pregnancy, the drug should be discontinued.
In case of acute or chronic liver dysfunction, a woman should contact a specialist for examination and consultation.
Women should be informed that Charozette® does not protect against HIV infection or other sexually transmitted diseases.
Reduced efficiency
The effectiveness of progestin-containing oral contraceptives may be reduced if pills are missed, gastrointestinal disorders, or when taking other medications.
Changes in the nature of menstruation
While using progestin-containing contraceptives, some women may experience vaginal bleeding more frequently or for a longer period of time, while for other women this bleeding may become less frequent or stop altogether. These changes are often the reason that a woman refuses this method of contraception, or ceases to strictly follow the doctor's instructions. In detailed consultation with women who decide to start taking Charozetta®, the doctor should discuss the possibility of such changes in the nature of the menstrual cycle. Evaluation of vaginal bleeding should be based on clinical presentation and may include testing to rule out malignancy or pregnancy.
Follicle development
When taking all low-dose hormonal contraceptives, follicle development occurs; occasionally, the size of the follicle can reach sizes exceeding those in a normal cycle. In general, these enlarged follicles disappear spontaneously. This often occurs without symptoms; in some cases there is mild pain in the lower abdomen. Surgery is rarely required.
Lab tests
Data obtained with combined oral contraceptives have shown that the use of hormonal contraceptives may affect the results of some laboratory tests, including biochemical parameters of liver, thyroid, adrenal and kidney function, serum levels of (transport) proteins, such as globulin , binding corticosteroids, on lipid/lipoprotein fractions, indicators of carbohydrate metabolism and indicators of blood clotting and fibrinolysis. Usually these changes remain within normal limits. It is not known to what extent this also applies to progestogen-only contraceptives.
Mammary cancer
The risk of breast cancer increases with age. While using combined oral contraceptives, a woman's risk of being diagnosed with breast cancer increases slightly. This increased risk gradually disappears over 10 years after stopping oral contraceptives and is not related to duration of use but depends on the woman's age at the time of combined oral contraceptive use. The expected number of breast cancer diagnoses among 10,000 women who used combined oral contraceptives (within 10 years of stopping use), relative to women who never took them during the same period, calculated for the corresponding age groups, is presented in the table below .
| Age group | Expected number of cases among women using combined oral contraceptives | Expected number of cases among women not using oral contraceptives |
| 16-19 years old | 4.5 | 4 |
| 20-24 years old | 17.5 | 16 |
| 25-29 years old | 48.7 | 44 |
| 30-34 years old | 110 | 100 |
| 35-39 years old | 180 | 160 |
| 40-44 years old | 260 | 230 |
The risk in women using progestin-only oral contraceptives, such as Charozetta®, may be similar to those using combined oral contraceptives. However, the data for progestogen-only oral contraceptives are less clear. Compared with the lifetime risk of breast cancer, the increase in risk associated with combined oral contraceptives is small. Breast cancer diagnosed in women using combined oral contraceptives tends to be less clinically advanced than cancer diagnosed in women who have never used combined oral contraceptives. The increased risk in women using combined oral contraceptives may be due to earlier diagnosis, biological effects of the drug, or a combination of these two factors.
Venous thromboembolism
Epidemiological studies have established an association between the use of combined oral contraceptives and an increased incidence of venous thromboembolism (VTE, deep vein thrombosis and pulmonary embolism). Although the clinical significance of these data for desogestrel, as a contraceptive that does not contain an estrogen component, is unknown, the use of Charozetta® should be discontinued if thrombosis develops. Discontinuation of Charozetta® should be considered in case of prolonged immobilization associated with surgery or illness.
Diabetes
Although gestagens may affect peripheral insulin resistance and glucose tolerance, there is no evidence that there is a need to change the therapeutic regimen in diabetic patients using gestagen-containing oral contraceptives. However, women with diabetes should be closely monitored during the first months of using the drug.
Bone mineral density
The use of Charozetta® leads to a decrease in serum estradiol levels to a level corresponding to the early follicular phase. It is currently unknown whether this decrease has any clinically significant effect on bone mineral density.
Prevention of ectopic pregnancy
Prevention of ectopic pregnancy with traditional gestagen-containing oral contraceptives (“mini-pills”) is not as effective as with combined oral contraceptives, since ovulation often occurs when using “mini-pills.” Although Charozetta® effectively suppresses ovulation, in the case of amenorrhea or abdominal pain, ectopic pregnancy should be excluded in the differential diagnosis.
Charozetta® contains no more than 65 mg of lactose, so women with rare hereditary disorders associated with galactose intolerance, lapp lactase deficiency or glucose-galactose malabsorption should refrain from taking the drug.
Impact on the ability to drive vehicles and operate machinery
Based on the pharmacodynamic profile, it is believed that Charozetta® does not affect the ability to drive vehicles and operate machinery.
Analogs
Level 4 ATX code matches:
Eskinor-F
Microlute
Exluton
Postinor
Escapelle
Implanon NKST
Lactinet
For those who are looking for analogues of Charozetta, experts recommend Lactinet .
Reviews of Charozette
Birth control pills Charozetta receive very different reviews on forums. For the most part, however, the opinions are positive . Only those for whom taking this drug was not without side effects (mainly weight gain and menstrual cycle disruptions) speak negatively. Reviews of Charozette during breastfeeding are also generally positive. Only in some rare cases did women notice a decrease in milk supply . Reviews from doctors also indicate the effectiveness of this drug. It is especially often prescribed after childbirth, since it is not contraindicated during lactation .
CHAROSETTE
special instructions
Medical examinations/consultations
Before prescribing the drug, a woman should carefully collect anamnesis and conduct a thorough gynecological examination to exclude pregnancy. Before prescribing the drug, the cause of menstrual irregularities, for example, oligomenorrhea and amenorrhea, should be established. The interval between control medical examinations is determined by the doctor in each individual case (the frequency of examinations is at least once a year). If the prescribed drug may affect a latent or existing disease, an appropriate schedule of follow-up medical examinations should be drawn up.
Despite regular use of Charozetta®, irregular bleeding may sometimes occur. If bleeding is very frequent and irregular, you should consider using another method of contraception. If the above symptoms are persistent, then in this case it is necessary to exclude organic pathology. Management of amenorrhea while using the drug depends on whether the tablets were taken as directed and may include a pregnancy test. In case of pregnancy, the drug should be discontinued.
In case of acute or chronic liver dysfunction, a woman should contact a specialist for examination and consultation.
Women should be informed that Charosette® does not protect against HIV infection (AIDS) or other sexually transmitted diseases.
Reduced efficiency
The effectiveness of progestin-containing oral contraceptives may be reduced if pills are missed, gastrointestinal disorders or other medications are taken.
Changes in the nature of menstruation
While using progestin-containing contraceptives, some women may experience vaginal bleeding more frequently or for a longer period of time, while for other women this bleeding may become less frequent or stop altogether. These changes are often the reason that a woman refuses this method of contraception, or ceases to strictly follow the doctor's instructions. In detailed consultation with women who decide to start taking Charozetta®, the doctor should discuss the possibility of such changes in the nature of the menstrual cycle. Evaluation of vaginal bleeding should be based on clinical presentation and may include testing to rule out malignancy or pregnancy.
Follicle development
When taking all low-dose hormonal contraceptives, follicle development occurs; occasionally, the size of the follicle can reach sizes exceeding those in a normal cycle. In general, these enlarged follicles disappear spontaneously. This often occurs without symptoms; in some cases there is mild pain in the lower abdomen. Surgery is rarely required.
Lab tests
Data obtained with combined oral contraceptives have shown that the use of hormonal contraceptives may affect the results of some laboratory tests, including biochemical parameters of liver, thyroid, adrenal and kidney function, serum levels of (transport) proteins, such as globulin , binding corticosteroids, on lipid/lipoprotein fractions, indicators of carbohydrate metabolism and indicators of blood clotting and fibrinolysis. Usually these changes remain within normal limits. It is unknown to what extent this also applies to progestogen-only contraceptives.
Mammary cancer
The risk of breast cancer increases with age. While using combined oral contraceptives, a woman's risk of being diagnosed with breast cancer increases slightly. This increased risk gradually disappears over 10 years after stopping oral contraceptives and is not related to duration of use but depends on the woman's age at the time of combined oral contraceptive use. The expected number of breast cancer diagnoses among 10,000 women who used combined oral contraceptives (within 10 years of stopping use) relative to women who never took them during the same period, calculated for the corresponding age groups, is presented in the table below.
| Age group | Expected number of cases among women using combined oral contraceptives | Expected number of cases among women not using oral contraceptives |
| 16-19 years old | 4,5 | 4 |
| 20-24 years old | 17,5 | 16 |
| 25-29 years old | 48,7 | 44 |
| 30-34 years old | 110 | 100 |
| 35-39 years old | 180 | 160 |
| 40-44 years old | 260 | 230 |
The risk in women using progestin-only oral contraceptives, such as Charozetta®, may be similar to those using combined oral contraceptives. However, the data for progestogen-only oral contraceptives are less clear. Compared with the lifetime risk of breast cancer, the increase in risk associated with combined oral contraceptives is small. Breast cancer diagnosed in women using combined oral contraceptives tends to be less clinically advanced than cancer diagnosed in women who have never used combined oral contraceptives. The increased risk in women using combined oral contraceptives may be due to earlier diagnosis, biological effects of the drug, or a combination of these two factors.
Venous thromboembolism
Epidemiological studies have established an association between the use of combined oral contraceptives and an increased incidence of venous thromboembolism (VTE, deep vein thrombosis and pulmonary embolism). Although the clinical significance of these data for desogestrel as a contraceptive that does not contain an estrogen component is unknown, the use of Charozetta should be discontinued if thrombosis develops. Discontinuation of Charozetta® should be considered in case of prolonged immobilization associated with surgery or illness.
Diabetes
Although gestagens may affect peripheral insulin resistance and glucose tolerance, there is no evidence that there is a need to change the therapeutic regimen in diabetic patients using gestagen-containing oral contraceptives. However, women with diabetes should be closely monitored during the first months of using the drug.
Bone mineral density
The use of Charozetta® leads to a decrease in serum estradiol levels to a level corresponding to the early follicular phase. It is currently unknown whether this decrease has any clinically significant effect on bone mineral density.
Prevention of ectopic pregnancy
Prevention of ectopic pregnancy with traditional gestagen-containing oral contraceptives (“mini-pills”) is not as effective as with combined oral contraceptives, since ovulation often occurs when using “mini-pills.” Although Charozetta® effectively suppresses ovulation, in the case of amenorrhea or abdominal pain, ectopic pregnancy should be excluded in the differential diagnosis.
Charozetta® contains no more than 65 mg of lactose, so women with rare hereditary disorders associated with galactose intolerance, Lapp lactase deficiency, or glucose-galactose malabsorption should refrain from taking the drug.
Charozetta price, where to buy
The price of Charozetta in a package of 28 tablets is about 800 rubles. The product in a package of 84 tablets costs about 2,000 rubles. This price of Charozetta seems too high to many, so women are increasingly trying to find analogues of this drug.
- Online pharmacies in RussiaRussia
ZdravCity
- Charozetta tablets p.p.o.
75 mcg 84 pcs Organon RUR 3,784 order - Charozetta tablets p.p.o. 75mcg 28 pcs.Organon
RUB 1,454 order