Blockage of the tear duct, which occurs as a result of abnormal development of eye structures, inflammation, traumatic injury or other reasons, can lead to the most serious consequences. The OkoMed clinic offers adults and children treatment services for lacrimal duct obstruction .
Reasons for appearance
Dacryocystitis occurs in the presence of physiological pathologies, namely congenital narrowing of the duct (stenosis). Sometimes doctors detect a complete blockage of the tear duct.
- Trauma to the eyes or paranasal sinuses.
- Inflammatory process of the nose, which provokes swelling of the tissues around the eye.
- An infectious process caused by bacteria and viruses, which leads to blockage of the duct.
- Getting foreign particles into the eye or working in dusty and smoky rooms. As a result, the channel becomes clogged.
- Allergy to exposure to an irritant.
- Reduced protective properties of the body.
- Overheating and hypothermia.
- Presence of diabetes mellitus.
Very often this pathology occurs in newborn babies. This is due to the structural features of the tear ducts. When the baby is in amniotic fluid, the tear duct is closed with a special membrane, which must rupture during or after childbirth. This process does not occur if pathology occurs. Tears collect in the canal and this provokes an inflammatory process. It mainly develops in women. Men are also no exception, but this pathology is detected very rarely in them. The reason is differences in the structure of the lacrimal canal. Women use cosmetics, most of which cause inflammation.
Nasolacrimal duct obstruction (NLDO) in children
According to the development director of the specialized vision restoration center OPTIMED, doctor Alexander Nelin, it is very important to monitor eye health from birth. Therefore, it is very important to know about the problems and pathologies of the visual organs in children and the methods of their treatment.
Doctor Alexander Nelin read the article “Nasolacrimal Duct Obstruction (NLDO) in Children,” written by authors Shani Golan and Gary J Lelli Jr, and talks about this study:
“Nasolacrimal duct obstruction (NLDO) is common in pediatrics and manifests as persistent epiphora, recurrent conjunctivitis, crusting on the eyelids and sometimes dacryocystitis. It is usually congenital and occurs at the level of the Hasner valve. Treatment options for pediatric NLDO include non-surgical and surgical procedures. Treatment can be carried out both in the workplace and in the operating room. In the article, “Nasolacrimal duct obstruction (NLDO) in children,” the authors discuss the pathogenesis of pediatric NLDO and provide an update on current treatment options, including massage, which remains a very successful treatment, and surgery, which may be warranted in children over three years of age. who have anatomical variations and craniofacial abnormalities, or in patients who do not respond to medical therapy and probing, as well as in patients with acquired NLDO. In addition, the authors explored the benefits of new technologies and endoscopic approaches, including shorter operative times and less scarring, as well as the ability to perform bilateral procedures while addressing any additional intranasal pathology.”
Here's what the authors write in their article: “Nasolacrimal duct obstruction (NLDO) is common in pediatrics. The anatomical location of the obstruction is both before and after the lacrimal sac. It is usually congenital and occurs due to persistence of the membrane at the level of the valve of Hasner in the distal nasopharynx. Other causes include post-traumatic obstruction of the lacrimal system, the presence of associated systemic abnormalities, and acquired causes of NLDO. The incidence is higher in children with craniofacial anomalies.
Clinical manifestations of childhood NLDO usually include epiphora (which affects up to 20% of children), recurrent conjunctivitis, and crusting of the eyelids. Occasionally, swelling occurs below the level of the medial canthus (lacrimal mucocele). If a mucocele becomes infected, it is accompanied by swelling and erythema. If dacryocystitis becomes severe, the infected sac may rupture through the skin, which can lead to a lacrimal fistula. If you press on the lacrimal sac, there may be reflux of mucous material from the puncture.
In this review article, we (the authors) will discuss the anatomy of the nasolacrimal system, the pathogenesis of pediatric NLDO, and provide an update on current treatment options.
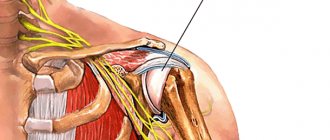
Anatomy of the nasolacrimal system
Tears pass through the superior and inferior lacrimal puncta, through the inferior and superior canaliculi to the common canaliculus, which drains into the lacrimal sac. At the junction between the common canaliculus and the lacrimal sac is the valve of Rosenmuller. The Rosenmuller valve is a one-way valve. Fluid from the lacrimal sac drains lower into the nasolacrimal duct and from there into the inferior opening of the nose, which is partially covered by mucous membrane known as the valve of Hasner.
Epiphora in pediatrics
Congenital nasolacrimal duct obstruction (cNLDO) is the most common cause of pediatric epiphora and is discussed in this review. Lacrimal sac cyst (Dacryocele) is another common mechanism and is discussed later. Other causes of pediatric epiphora are found in approximately 4% of cases and include proximal tear dysgenesis, punctate agenesis, and tubular wall dysgenesis.
In several cases of punctal and canal dysgenesis, it was noted that the mean age of patients was older than that of cNLDO patients (3.6–6.8 years). These different diagnoses from cNLDO must be carefully evaluated before diagnosing cNLDO as the treatment required is different.
Congenital obstruction of the nasolacrimal duct
Congenital nasolacrimal duct obstruction (cNLDO) occurs in approximately 6-20% of newborns. Often in these cases, the obstruction resolves on its own or with medical help within the first year of life; however, more complex cases require surgery. Several Pediatric Eye Disease Investigator Group (PEDIG) studies of cNLDO have been published in recent years, including studies examining the association between cNLDO and ametropia/amblyopia and introducing new surgical techniques and instruments to treat it. state.
The development of the lacrimal system begins in the fifth week of pregnancy. A lumen forms in the lacrimal canal, and cavitation of the layer of the lower passage occurs at the 10th week. Subsequently, the canalization of the lacrimal canal allows communication with the lower meatus from the sixth month of the fetus until the end of pregnancy. If this does not happen, a membrane barrier forms on the Hasner valve, which resolves spontaneously in 85-95% of cases by the first year of life.
A recent study using high-resolution computed tomography showed that the obstruction was either a retained membrane at the distal end of the canal, bony obstruction, or narrowing of the lower meatus associated with the nasal mucosa.
Lacrimal sac cyst (Dacryocele)
Lacrimal sac cysts occur in approximately one in 3,900 newborns. In addition to the typical obstruction at the Hasner valve, these newborns have a ball valve effect at the level of the Rosenmüller valve, resulting in rupture of the lacrimal sac. A lacrimal sac cyst appears as severe swelling on the lower eyelid just below the medial canthus and can be detected prenatally on ultrasound and magnetic resonance imaging. It is most common in women and is bilateral in 25% of patients. Infection occurs in 24-60% of cases.
As with cNLDO, lacrimal sac cysts have a high likelihood of spontaneous resolution; 50% of cases of lacrimal sac cyst resolve prenatally before birth. Massage of the lacrimal sac and administration of topical antibiotics can lead to resolution in 76% of cases. Endoscopic removal of an associated intranasal cyst increases the success rate to 95%.
Treatment of nasolacrimal duct obstruction (NLDO) in children
NLDO has a high resolution rate without surgery. In one observational study using medical treatment alone, NLDO resolution rates by the first year of life were 80% at 3 months of age, 70% at 6 months of age, and 52% at 9 months of age. PEDIG found that 66% of infants aged 6-10 months had their problem resolved without surgery within a 6-month period. Spontaneous resolution after 1 year of age is also possible, as evidenced by Yound et al., who found that 41% of children with congenital NLDO had spontaneous resolution in the second year of life (after 1 year of age but before 2 years of age).
Medical treatment
Medical treatment for NLDO consists of massage of the nasolacrimal sac along with the use of topical antibiotics if discharge is present. Massaging the nasolacrimal sac with a downward motion will result in hydrostatic pressure breaking the membrane obstruction at the Hasner valve.
Downward massage of the nasolacrimal sac is more effective than simple massage or no massage. A recent study showed that the success rate of the Crigler massage technique was 56% in children under 2 months of age, 46% in children aged 2-6 months, and 28% in children over 6 months of age.
Probing of the nasolacrimal duct
The most common surgical procedure used to treat NLDO in children is nasolacrimal duct probing. Probing is a safe and effective treatment for cNLDO; however, the optimal timing for the procedure remains controversial. On the one hand, spontaneous resolution may occur after 13 months of age, and some authors suggest that spontaneous resolution may occur before 48 months of age; on the other hand, it is believed that probing may be less successful at older ages. The procedure can be done in the office under local anesthesia (usually for children aged 6-9 months) or in the surgery under general anesthesia (for children over 12 months of age). Several studies have shown that probing performed in the office under local anesthesia is not associated with a statistically significant reduction in symptomatic months compared with probing performed later in a surgical facility under general anesthesia. However, while in-office probing is slightly less expensive than surgical probing, it has also been found to have a slightly lower success rate. The decision whether to perform probing before or after the child is 1 year of age should be based on the experience of the treating ophthalmologist and the probing specialist.
In general, the success rate for probing is estimated to be in the range of 80–90% in children under 3 years of age and remains high until the child is three years of age, after which success rates begin to decline. Studies conducted by PEDIG in children under 4 years of age with cNLDO showed success rates of 78% with probing, 82% with balloon catheter, and 91% with nasolacrimal duct intubation. The success rate is lower with bilateral disease or when more than one clinical sign of NLDO is present, but does not appear to be associated with age between 6 and <15 months.
With the introduction of endoscopic surgical techniques for operations on the nasolacrimal system, endoscopic probing has been proposed as an alternative to traditional blind probing. Endoscopic probing allows visualization of the inferior portion of the nasolacrimal system and nasal abnormalities such as atresia, cyst, stenosis, and false probing passage. In addition, direct visualization allows one to observe the process of passage of the probe, which, in turn, affects the success of the probe. Several studies comparing these two techniques in children with cNLDO have shown significantly higher success rates with endoscopic probing, particularly in older children, likely due to the additional ability to monitor and treat associated problems.
Silicone tube intubation for cNLDO is a well-established treatment option for cNLDO after failed probing and irrigation. Several large studies have reported success rates ranging from 82-97% after silicone intubation. Controversy exists regarding whether nasolacrymal intubation may be more likely to fail in older children. In a comparison study of simple probing and probing with intubation as a secondary procedure, patients treated with intubation were significantly more likely to have a successful outcome.
Bicanalicular and monocanalicular intubation are equally successful in treating cNLDO. The monocanalicular tube is easier to insert and remove and is therefore more commonly used in pediatrics. Most intubation systems require intraoperative removal of the tube from the nose. However, monocanalicular tubes can be removed proximally, allowing for in-office removal in many children. Lacrimal tubes are usually removed after 2-6 months. In children under 2 years of age, tube removal usually occurs after 6 weeks; for older children, a longer period of intubation is appropriate, and the chances of success are increased if the tube is left in place for at least 3 months.
Several conditions may require earlier tube removal, such as abrasion (trauma) of the cornea or conjunctiva from the tube, granuloma formation, and puncture erosion.
Masterak® monocanalicular tubes (FCI Ophthalmics Inc., Pembroke, MA, US) are held in place by a hook on the support plate that is placed in the punctum. This support plate can become loose or fall out spontaneously, so care should be taken when dilating the punctum so as not to enlarge it to a size where it cannot securely hold the tube support plate. Bicanalicular tubes, if placed in the nose, may require removal under brief general anesthesia.
Pediatric dacryocystorhinostomy (DCR)
Dacryocystorhinostomy (DCR) in children is used in cases of NLDO that do not respond to medical therapy, catheterization, or intubation. When asked about the timing of surgery, 79% of American Pediatric Eye and Strabismus Association members said they begin recommending surgery under general anesthesia for cases of unresolved cNLDO at 13 months of age.
External DCR has traditionally been the preferred treatment option for cNLDO. In the external DCR study, there was improvement in all 134 cases, and complete cure was achieved in 96% of cases, with no immediate postoperative complications or few (3%) short-term complications. Endonasal DCR has become popular in the last decade, with success estimates of 88-100%.
Despite the technical difficulty of performing in young children, endonasal DCR has several advantages over external DCR: it can be performed in acute conditions, it avoids facial scarring, it causes fewer anatomical disturbances, it does not disrupt the lacrimal pump mechanism, it reduces the time surgery, and it may even reduce postoperative discomfort. Additionally, endonasal DCR can simultaneously treat any associated nasal pathology and can be performed bilaterally under general anesthesia as an outpatient procedure. However, disadvantages associated with endonasal DCR include longer training times to operate in the narrow nasal space in children and technical difficulties arising from existing anatomical variations. When comparing the success rate of endonasal and external DCR in pediatric patients, endoscopic DCR produces similar results compared to external DCR.
In 2011, Uysal et al. reported their experience of performing the procedure using an endocanal diode laser. Of the 18 cases presented, 100% achieved anatomical success (determined by endothelial patency); the clinical success rate (resolution of epiphora) was 85%.
In addition, endoscopic ultrasound DCR is an alternative method for managing NLDO. The main advantage of this method is safety for the surrounding soft tissues during osteotomy. In a recent study published at 6-month follow-up, anatomical and functional success rates were observed in 93.1% and 88.6%, respectively.
conclusions
Our review examines the clinical aspects of pediatric NLDO. Massage using the Crigler maneuver remains highly successful. Probing the lacrimal system is also very effective, at least up to 3 years of age. Resolution with medical intervention is possible after the first year of life, so it is reasonable to continue until approximately 15 months of age. After unsuccessful attempts at probing, intubation of the nasolacrimal duct should be used. In addition, children with NLDO should be monitored until 3–4 years of age to ensure that anisometropic amblyopia does not develop.
In some cases, DCR surgery may be required, these cases include: children over 3 years of age, children with anatomical variations and craniofacial anomalies, patients not responding to medical therapy and probing, and patients with acquired NLDO. Although external DCR remains a successful and viable option, new technologies and endoscopic approaches can reduce operative time and leave no scars. Additionally, these approaches allow for bilateral procedures and allow the clinician to simultaneously address any additional intranasal pathology.
Symptoms of the disease
Tears are necessary for the normal functioning of the visual organs. They moisturize the cornea of the eye, protect against mechanical irritants, and perform an antibacterial function.
Sometimes tears stop flowing, this is the first sign of tear duct obstruction. Treatment is one way to cope with the problem and prevent the development of canaliculitis. Sometimes massage of the tear duct helps.
- painful and unpleasant sensations in the eye area;
- redness of the skin around the eye;
- feeling of squeezing and bursting;
- swelling of the skin;
- lacrimation;
- edema;
- vision problems;
- increased secretion of mucus, which smells bad;
- formation of pus;
- high body temperature;
- intoxication of the body.
The acute stage of dacryocystitis appears as an inflammatory process affecting one eye. In the chronic stage, the tear duct swells, the eye turns red and the number of tears increases.
If you experience such symptoms, you should consult a doctor. Blockage can occur in both acute and chronic stages. The accumulation of tear fluid increases the likelihood of infectious processes.
What are the symptoms of dacryocystitis?
Symptoms of dacryocystitis are similar to sore eyes and conjunctivitis. Illness causes swelling and redness in the eye area, pain syndrome, and lacrimation. Relevance lies in the fact that:
- often conjunctivitis develops on both eyes, and dacryocystitis on one;
- The development of dacryocystitis can lead to the appearance of conjunctivitis (infection of the clear membrane above the white of the eye).
It is the doctor's fault to make the diagnosis. Complicated dacryocystitis can cause serious illness in healthy people and often lead to:
- culprit of lacrimal fistulas;
- orbital cellulitis (infection of the eye);
- development of a brain abscess;
- meningitis;
- thrombosis of the cavernous sinus;
- important sinusitis;
- waste your time.
Diagnostics
Dacryocystitis is detected without much difficulty. At the appointment, the doctor performs a visual assessment of the eye and palpation of the lacrimal sac.
- Test using paint. The eye is instilled with a solution containing a dye. If pigment appears in the eye after a few minutes, this indicates a blockage of the tear ducts.
- Probing. Using a probe with a needle, the ophthalmologist penetrates the duct, which helps to expand it and get rid of the problem.
- Dacryocystography. Carrying out an X-ray examination with the introduction of a dye. In the picture you can see the structure of the eye system and identify the problem.
- Patency can also be checked with the West test. A cotton swab is placed in the nasal passage, on the affected side. Collargol is instilled into the eye. The condition is considered normal when after 2 minutes the tampon turns dark. If the swab remains clean or stained after 10 minutes, there is a problem.
Contraindications
Only an ophthalmologist can assess the function of drainage of the lacrimal canal and then select treatment methods.
However, the procedure for washing the nasolacrimal canal is not recommended in two cases:
- When the lacrimal sac is stretched and filled with mucus, such a procedure can give impetus to the spread of pus throughout the organs of vision.
- In case of purulent acute inflammation - hydrocele of the lacrimal sac - washing can cause its overstretching and lead to rupture of the structure of the sac.
Treatment
Eyes are the mirror of the soul. When an eye problem arises, there is no need to take risks. Treatment should be prescribed by a doctor after preliminary diagnosis. The treatment method is selected depending on the form and cause of the pathology that provoked it, and age characteristics.
- Rinsing the eyes with antibacterial and disinfectant solutions.
- The use of special drops and ointments.
- Massage procedures and compresses to help clean the canal.
Eye rinsing with antiseptic solutions is carried out several times a day. The procedure is performed by an ophthalmologist in a hospital setting.
Ointments and drops that have an antibacterial effect:
- Phloxal . Antibacterial drug with a wide spectrum of effects. Fights the inflammatory process. The course of treatment is 10 days, two drops twice a day.
- Dexamethasone . Drops with an antibacterial effect. Effective against infectious processes. Instill 5 times a day. The required dosage and course of treatment are selected by the doctor individually for each patient.
- Levomycetin is a hormonal drug. Used for allergic reactions and inflammations.
- Ciprofloxacin . Prescribed for infections of the lacrimal duct. Buried every three hours.
The drugs have contraindications and side effects. Drug therapy is carried out under the supervision of the attending physician.
If the treatment does not have a positive effect, bougienage is performed - cleaning the lacrimal canal from purulent contents;
You can quickly cope with the disease only if treatment is started in a timely manner. If symptoms are negative, you should visit an ophthalmologist.
What is dacryocystitis?
Inflammation of the tear ducts is called dacryocystitis, which can be congenital and inflamed. Congenital dacryocystitis occurs after development through the obstruction of the Hasner valve, which is dissolved in the nasolacrimal protocys. The same disease can be diagnosed in people over 40 years of age. Full-blown dacryocystitis develops as a result of age-related changes, systemic damage or trauma.
Trivalism is divided into chronic and acute dacryocystitis. Chronic dacryocystitis develops in aphids of the incomplete acute form of the disease. Acute dacryocystitis can be provoked by such pathogens as Staphylococcus aureus or Epidermal Staphylococcus, Hemolytic Streptococcus B, Pneumococcus, Haemophilus influenzae or Pseudomonas aeruginosa.
Ignition of mucus ducts can provoke:
- injuries and anomalies of the nasal septum;
- otolaryngological illness (rhinitis, hypertrophy of the nasal turbinates);
- endoscopic or endonasal procedures;
- new developments in the nasolacrimal area;
- systemic illnesses (sermonal wolfworm, sarcoidosis, Wegener's granulomatosis);
- medicinal specialties.
Symptoms of eye disease are often similar. For example, dacryocystitis in captives can be confused with conjunctivitis. An ophthalmologist is involved in the diagnosis and treatment of problems. If unpleasant symptoms appear in the eye area, seek help from a doctor.
Radical ways to fight
If there is no positive effect from drug treatment, or if the cause is a tumor or cyst, surgical treatment is performed.
Surgical intervention happens:
- Endoscopic dacryocystorhinostomy I. A device with a camera is inserted into the duct. A puncture or incision is made using an endoscope. A special valve is created, the main purpose of which is drainage. The recovery period is 7 days. In parallel, antibiotic therapy is carried out to prevent the risk of developing an inflammatory process. The main advantage is the absence of visible marks after the operation.
- Balloon dacrycytoplasty is an intervention that, due to its safety, is performed even on newborns. A conductor with a reservoir filled with liquid is inserted into the channel. Allows you to expand the area, thereby breaking through it. The procedure is carried out under local anesthesia. During the rehabilitation period, special drops and antibacterial drugs are prescribed.
Analysis of results
Best materials of the month
- Coronaviruses: SARS-CoV-2 (COVID-19)
- Antibiotics for the prevention and treatment of COVID-19: how effective are they?
- The most common "office" diseases
- Does vodka kill coronavirus?
- How to stay alive on our roads?
Ophthalmologists interpret the results when washing the nasolacrimal canals according to the following scheme.
In the absence of pathology of the canals, the liquid easily flows through the nose. When introducing the solution, no particular effort is required; the liquid is injected with light pressure on the piston. Stenosis of the nasolacrimal duct or fusion of the canal orifices is indicated by the leakage of fluid from the opposite lacrimal punctum.
With stenosis of the nasolacrimal duct, fluid may begin to flow from the opposite lacrimal opening not immediately, but after a matter of seconds or after increasing pressure on the piston. At the same time, there are traces of blood in it. With stenosis of the internal part of the canal, fluid flows out from the same place where it was injected.
When the nasolacrimal duct becomes clogged, fluid flows out of the nose when the pressure on the syringe plunger increases.
Massage
Prepare your hands before the procedure: wash, disinfect or wear gloves.
Massage scheme:
- Press on the outer corner of the eye, turn your finger towards the bridge of the nose.
- Gently press and massage the lacrimal sac, removing purulent masses from it.
- Instill a warm solution of furatsilin and remove the discharge.
- Carry out pressing and massaging movements along the tear ducts.
- Jerky movements along the nasolacrimal sac with some force to open the canal and extract the discharge.
- Instill a solution of chloramphenicol.
A little anatomy
Nature has endowed humans with a unique lacrimal apparatus, which consists of the lacrimal gland and lacrimal ducts. The lacrimal gland is almond-shaped and located just behind the eye under the frontal bones of the skull. A dozen tear ducts are laid from it to the eye and eyelid. When you blink, tears are released from the lacrimal gland, which washes the eye. Sterile tears keep the eye clean, moisturize it, and the enzymes they contain destroy bacteria, preventing the spread of infection.
The lacrimal puncta in the inner corner of the eye (on the lower and upper eyelids) are connected to the lacrimal sac, from which tears enter the nose through the nasolacrimal duct. The uninterrupted outflow of ocular fluid is carried out due to negative pressure in the lacrimal sac.
In case of obstruction of the canals, the fluid formed in the eye stagnates in the lacrimal sac and can lead to its swelling and inflammation. In such cases, rinsing is required.
Folk remedies
After prior approval from a doctor, traditional medicine is successfully used at home.
Folk remedies:
- Aloe. For inflammation, it is good to instill freshly prepared aloe juice, half diluted with saline solution.
- Eyebright. Cook in the same way. Use for eye drops and compresses.
- Chamomile. Has an antibacterial effect. You need to take 1 tbsp. l. collection, boil in a glass of boiling water and leave. Use to wash eyes.
- Thyme . Due to its anti-inflammatory properties, the infusion is used for dacryocystitis.
- Kalanchoe. Natural antiseptic. Cut off the leaves and keep in the refrigerator for two days. Next, extract the juice and dilute it in a 1:1 ratio with saline. This remedy can be used to treat children. Adults can instill concentrated juice into the nose, 2 drops each. The person begins to sneeze, during which the tear duct is cleared of pus.
- Leaves from a rose . Only those flowers that are grown on your own plot are suitable. You will need 100 gr. collection and a glass of boiling water. Boil for five hours. Use as lotions.
- Burda ivy-shaped . Brew a tablespoon of herb in a glass of boiling water, simmer for 15 minutes. Use for rinsing and compresses.
- Bell pepper . Drink a glass of sweet pepper fruit every day. adding a teaspoon of honey.
What to do if you don’t immediately start treating dacryocystitis?
Treatment for dacryocystitis should be started as soon as the first symptoms appear, in order to prevent complications from developing. Often complications after dacryocystitis develop without prompt or proper treatment.
Inflammation of the lacrimal ducts is characterized by low illness and mortality. However, congenital dacryocystitis can lead to death, most likely due to inappropriate treatment.