If wounded (with insufficient treatment), wound infection may occur. This is due to the fact that when wounded, microbes enter the wound area, which can subsequently multiply. It also happens that an infection occurs not when a specific area of the body is affected, but when it is subsequently cared for improperly - germs can be brought in from clothing or from surrounding objects (if a person walks without a bandage).
As a rule, it is possible to detect this disease a week after the infection occurs. Of course, infection in a wound does not always lead to bacteria starting to multiply. The consequence of the fact that bacteria begin to develop in the wounded area usually results in sepsis. This is a very serious disease that can occur if the patient is not provided with timely assistance.
Causes of wound infection
Typically, the pathogens that contribute to the development of severe infections are various types of bacteria or viruses. They can enter the human body if he does not follow the rules of hygiene, which must necessarily be accompanied by the use of antiseptics. It happens that tissue infection occurs during implantation of prostheses. In this case, the body cannot accept the foreign material, and suppuration begins to develop. People who do not take care of their health and eat improperly have a weakened immune system. This causes the wounds to begin to fester. Experts have found that in people who have chronic, untreatable diseases, infection occurs much more often than in those people who are completely healthy.
Products and dressings for the treatment of chronic wounds
The course of therapy is selected by the attending physician; you should not self-medicate - this can lead to a worsening of the situation.
Gels and solutions for rinsing and cleansing
- Gels fill subcutaneous pockets and cavities, providing an antimicrobial effect (Prontosan gel), cleanse necrotic masses (Askina gel, Hydrosorb gel), form an optimal environment for healing (Purilon gel), and work as an anti-inflammatory antimicrobial agent (Emalan collagen hydrogel).
- Prontosan sterile solution is suitable for preventing infections, cleaning and moisturizing wounds, helping in tissue regeneration and suppressing pathogenic microflora.
Symptoms of infected wounds
When a wound becomes infected, the following symptoms are possible:
- There is redness in the area where the infection occurred.
- Possible tissue swelling.
- Many patients report severe pain.
- Since the inflammatory process begins throughout the body, as a result, the patient’s body temperature rises.
- Purulent discharge at the wound site.
- Tachycardia.
- Headache, nausea.
If the above symptoms appear, you should immediately consult a doctor, as the consequences can be extremely severe.
Treatment of purulent wounds
When treating purulent wounds, the stage of the wound process should be taken into account. The wound process is a complex of reactions of the body to tissue damage. This process is conditionally divided into three phases: • inflammation phase; ○ stage of vascular changes; ○ stage of wound cleansing; • regeneration phase; • phase of scarring and epithelization.
In the first phase - the phase of inflammation - the formation of purulent exudate occurs with the simultaneous absorption of toxic substances. At this stage, the main task is to cleanse the wound - remove purulent masses and remnants of dead tissue, wash and drain the wound, and stop bleeding. Also at this stage it is necessary to limit and reduce inflammation as much as possible and destroy pathogenic microflora. To disinfect and ensure the outflow of fluid, antibacterial hydrophilic ointments are used, for example, levomekol or ready-made dressings - Voskopran with ointments levomekol, povidone-iodine or Dioxidin.
In the second phase, thin and delicate connective tissue with capillaries begins to form on top of the wound - granulation. At this stage, it is necessary to protect the newly formed tissue from damage, stimulate further regeneration and prevent the resumption of the inflammatory process. Healing-accelerating agents help stimulate regeneration - methyluracil ointment or Voskopran dressing with methyluracil ointment; dressings also help protect newly formed tissues.
The third phase is the formation of dense scar tissue over the wound and the beginning of epithelization. At this stage, it is necessary to accelerate epithelization and wound healing.
In the treatment process, the correct selection of dressings plays an important role. Dressing material for purulent wounds must meet the following requirements: • have high absorbency; • hold the medicinal product on its surface for a long time; • do not leave fibers; • allow oxygen to pass through, allowing the wound to “breathe”.
Medical dressings meet all of the above requirements. The range includes suitable dressings for the management of purulent wounds at all stages.
For the first phase, a Parapran dressing with chymotrypsin is well suited - it removes exudate into a secondary sorption dressing and has a necrolytic effect, helping to break down dead tissue and cleanse the wound, as well as Voskopran with various ointments: levomekol - anti-inflammatory effect; povidone-iodine and Dioxidin - antimicrobial action. For wounds with heavy exudation, Medisorb is recommended as a secondary dressing, a sorption dressing characterized by high absorbency.
In the second phase, it is recommended to use Voskopran with methyluracil ointment, which stimulates wound healing.
In the third phase, you can use a regular Voskopran dressing without ointment to speed up the epithelization process and protect the scar from mechanical damage.
Chitopran, a thin biopolymer dressing that stimulates and accelerates the healing process, is well suited for the management of difficult-to-heal wounds in the granulation stage. It creates a sterile environment with an optimal level of humidity that promotes epithelialization. The material is extremely thin and flexible, which allows it to be used by patients with fragile and sensitive skin. There is no need to remove the bandage - the material is absorbed naturally.
Treatment of infected wounds
If the disease occurs with complications, the patient will require surgical intervention. After which the doctor must prescribe medications to the patient that will act on microbes, in simpler terms, they will kill all harmful microorganisms and also relieve the inflammatory process. As a rule, these are antibiotics. If the patient is not very sick, the following measures are usually applied:
- The patient needs to provide complete rest to the organ that is infected with the infection.
- Daily dressings are required, which should be carried out using only sterile bandages.
- Ointments such as syntomycin or Vishnevsky ointment are widely used to treat infected wounds.
- Blood transfusions are often used.
Complications of wounds. Basic principles of treatment
Wounds can be accompanied by a variety of complications, both immediately after the wounds are inflicted and in the long term. Wound complications include:
· The development of traumatic or hemorrhagic shock is the earliest and most serious complication. In the absence of immediate help, it causes an unfavorable outcome.
· Seromas are accumulations of wound exudate in wound cavities, dangerous due to the possibility of suppuration. When seroma develops, it is necessary to ensure the evacuation of fluid from the wound.
· Wound hematomas are formed due to incomplete stopping of bleeding. Hematomas are potential foci of infection; in addition, by squeezing surrounding tissues, they lead to ischemia. They must be removed by puncture or during wound revision.
· Necrosis of surrounding tissues - develops when the blood supply to the corresponding area is disrupted due to tissue trauma during surgery or improper suturing. Wet skin necrosis must be removed due to the risk of deep accumulations of pus. Superficial dry necroses of the skin are not removed, as they perform a protective function.
· Wound infection - its development is facilitated by a high level of contamination and high virulence of the microflora that has entered the wound, the presence of foreign bodies in the wound, necrosis, accumulations of fluid or blood, damage due to injury to bones, nerves, blood vessels, chronic disruption of local blood supply, as well as late surgical treatment and general factors influencing the course of the wound process. Experimental and clinical studies have established that in most cases, for the development of an infectious process in a wound, it is necessary for its contamination to exceed a critical level of 105-106 microorganisms per 1 gram of tissue. Among the general factors contributing to the development of wound infection, significant blood loss, the development of traumatic shock, previous fasting, vitamin deficiencies, overwork, the presence of diabetes mellitus and some other chronic diseases play an important role.
The development of pyogenic infection is caused by staphylococcus, Pseudomonas aeruginosa, Escherichia coli and other pyogenic bacteria, anaerobic infection - by clostridia and non-clostridial anaerobic microflora, erysipelas - by streptococci. When a wound infection generalizes, sepsis develops. Most often, the development of pyogenic wound infection occurs on days 3-5 after injury, less often at a later date - on days 13-15. Anaerobic infection can develop very quickly; in fulminant forms, it is diagnosed a few hours after injury.
If it gets into the wound with soil, dust, foreign bodies, Cl. Tetani may develop tetanus. In the absence of specific prevention, the probability of contracting tetanus in the presence of contaminated wounds reaches 0.8%. The rabies virus can enter the body through bite wounds.
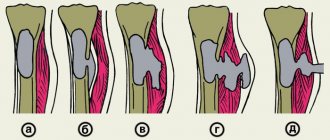
· Dehiscence of wound edges - occurs in the presence of local or general factors that impede healing, as well as when sutures are removed too early. During laparotomy, the divergence of the edges of the wound can be complete - with eventration, that is, with internal organs coming out, incomplete - with preservation of the integrity of the peritoneum, and hidden, when the integrity of the skin is preserved. Dehiscence of the wound edges is eliminated surgically.
· Complications of scars are the formation of hypertrophied scars and keloids. Hypertrophied scars develop when there is a tendency to excessive formation of scar tissue and most often when the wound is located perpendicular to the Langer line. Keloids, unlike hypertrophied scars, have a special structure and spread beyond the boundaries of the wound. Complications of scars lead not only to cosmetic, but also to functional defects, such as impaired walking or upper limb function due to limited range of motion in the joints. Surgical correction is indicated for hypertrophied scars with impaired function, but for keloids it often leads to a deterioration in the treatment outcome.
· Long-term chronic wounds can be complicated by the development of malignancy. The diagnosis is confirmed by a biopsy of wound tissue. Surgical treatment requires radical excision within healthy tissue.
Basic principles of wound care
Treatment for injuries usually takes place in two stages - the first aid stage and the qualified assistance stage.
¨ First aid stage
When providing first aid at the site of injury, two main tasks are solved: stopping bleeding and preventing further microbial contamination. First aid includes the use of available methods to temporarily stop bleeding, pain relief, application of a protective bandage and transport immobilization. At this stage, you should not wash the wound or remove foreign bodies from it.
¨ Qualified assistance stage
At the stage of hospital care, the following tasks are solved:
· prevention and treatment of wound complications;
· acceleration of the healing process;
· restoration of functions of damaged organs and tissues.
Basic principles of wound treatment:
· strict adherence to asepsis at all stages of treatment;
· mandatory surgical treatment;
· active drainage;
· the earliest possible closure of wounds with primary or secondary sutures or using autodermoplasty;
· targeted antibacterial and immunotherapy, correction of systemic disorders.
To select adequate wound treatment tactics, a thorough assessment of its condition is necessary, and the following is assessed:
· Localization, size, depth of the wound, damage to underlying structures such as fascia, muscles, tendons, bones.
· The condition of the edges, walls and bottom of the wound, as well as surrounding tissues, the presence and characteristics of necrotic tissue.
· The quantity and quality of exudate - serous, hemorrhagic, purulent.
· Level of microbial contamination. The critical level is the value of 105 - 106 microbial bodies per 1 g of tissue, at which the development of a wound infection is predicted.
· Time elapsed since injury.
¨ Treatment of contaminated wounds
The risk of developing wound complications in the presence of contaminated wounds is much higher than in aseptic wounds. Treatment of contaminated wounds consists of the following steps:
· In case of possible contact of the wound with the ground (all injuries with a violation of the integrity of the body, frostbite, burns, gangrene and tissue necrosis, out-of-hospital births and abortions, animal bites), measures are necessary to prevent a specific infection - tetanus, and in case of animal bites - rabies.
In order to prevent tetanus, vaccinated patients are administered 0.5 ml of adsorbed tetanus toxoid, unvaccinated patients - 1 ml of toxoid and 3000 IU of tetanus toxoid serum. Due to the danger of developing anaphylactic reactions to protein, the administration of anti-tetanus serum is carried out according to Bezredko: first, 0.1 ml of diluted serum is injected intradermally, if the size of the papule is less than 10 mm, after 20 minutes 0.1 ml of undiluted serum is injected subcutaneously, and only if there is no reaction to subcutaneous administration After 30 minutes, the entire dose is administered subcutaneously.
In case of bites from animals (dogs, foxes, wolves, etc.) suspected of rabies, or their saliva getting on damaged tissue, primary surgical treatment of the wound cannot be performed. The wound is only washed and treated with an antiseptic. There are no stitches. A course of subcutaneous administration of rabies vaccine is required, which is performed in specialized rabies centers, and tetanus prophylaxis. In the presence of superficial injuries (abrasions, scratches) of any location except the head, neck, hands, toes and genitals caused by domestic animals, culture purified concentrated rabies vaccine (COCAV) is administered 1 ml immediately, as well as on 3, 7, 14, 30 and 90 days. But if, when observing the animal, it remains healthy for 10 days, then treatment is stopped after 3 injections.
If animal saliva gets on the mucous membranes, if bites are localized in the head, neck, hands, toes and genitals, as well as with deep and multiple bites and any bites of wild animals, in addition to the administration of COCAB, immediate administration of rabies immunoglobulin (RAI) is necessary. Heterologous AIH is prescribed at a dose of 40 IU per kg of body weight, homologous - at a dose of 20 IU per kg of body weight. Most of the dose should be infiltrated into the tissue surrounding the wound, the rest is administered intramuscularly. If observation of the animal is possible, and it remains healthy for 10 days, then the administration of COCAV is stopped after the 3rd injection.
· In all cases of contaminated wounds, except for minor superficial injuries and cases where there are cosmetic and functional contraindications, primary surgical treatment (PST) with wound dissection, revision of the wound canal, excision of the edges, walls and bottom of the wound is mandatory. The purpose of PSO is the complete removal of non-viable and contaminated tissue. The later PST is performed, the lower the likelihood of preventing infectious wound complications.
PSO is not performed when wounds are localized on the face, as it leads to an increase in cosmetic defect, and good blood supply to this area ensures a low risk of suppuration and active wound healing. With extensive wounds of the scalp, performing PSO in full can lead to the impossibility of matching the edges and closing the wound. Non-penetrating puncture wounds without damage to large vessels and bite wounds with suspected penetration of the rabies virus are also not subject to PSO. PSO can be completed with the application of primary sutures - with suturing tightly or, in the presence of risk factors for wound suppuration, - with drainage left in place.
Preferably, flow-wash drainage of sutured wounds followed by dialysis with effective antiseptics. Flow-flushing drainage is carried out by installing counter perforated drains, one of which is used to administer the drug, and the other is used for outflow. The administration of drugs can be jet and drip, fractional or continuous. In this case, outflow can be carried out in a passive or active way - using vacuum.
This method protects wounds from secondary contamination, promotes more complete removal of discharge, creates conditions for a controlled abacterial environment and favorable conditions for wound healing. When draining, several general principles must be followed. Drainage is installed in sloping areas of the wound cavity, where fluid accumulation is maximum. Removing the drainage tube through the counter-aperture is preferable than through the wound, since the drainage, being a foreign body, interferes with the normal healing of the wound and contributes to its suppuration.
If there is a high risk of developing wound suppuration, for example, in the presence of sudden changes in the surrounding tissues, the application of primary delayed sutures, including provisional ones, is indicated. Like the primary ones, these sutures are placed on the wound before the development of granulation tissue, usually 1-5 days after PSO when the inflammatory process subsides. The healing of such wounds proceeds according to the type of primary intention. Sutures are not applied only after treatment of gunshot wounds and if it is impossible to compare the edges of the wound without tension; in the latter cases, the earliest possible closure of the wound defect using reconstructive surgery is indicated.
· Antibiotic prophylaxis is carried out according to the same scheme as for “dirty” surgical interventions. A 5-7 day course of antibiotics is required.
· Antiseptic prophylaxis involves the use of effective antiseptics at all stages of the operation and when caring for the wound. When treating wounds, chlorhexidine, sodium hypochlorite, dioxidine, lavasept, hydrogen peroxide, potassium permanganate and other antiseptics can be used. Drugs such as furatsilin, rivanol, chloramine are currently not recommended for use in surgical departments, since hospital microflora are resistant to them almost everywhere.
· Wound management after PSO with suturing is similar to the management of surgical wounds. Regular changes of aseptic dressings and drainage care are performed. Treatment of open wounds after PSO is carried out, like the treatment of purulent wounds, in accordance with the phases of the wound process.
¨ Treatment of purulent wounds
Treatment of purulent wounds is complex - surgical and conservative.
· In all cases of infected wounds, when there are no special functional contraindications, secondary surgical debridement (SDT) is performed. It consists of opening a purulent focus and leaks, evacuation of pus, excision of non-viable tissue and mandatory provision of adequate drainage of the wound. If the wound is not sutured after VChO, secondary sutures may be applied in the future. In some cases, with radical excision of an abscess during VCO, primary sutures can be applied with mandatory drainage of the wound. Preferably flow-through drainage. If there are contraindications to carrying out VChO, they are limited to measures to ensure adequate evacuation of exudate.
· Further local treatment of purulent wounds depends on the phase of the wound process.
In the inflammation phase, the main goals of treatment are fighting infection, adequate drainage, accelerating the process of wound cleansing, and reducing systemic manifestations of the inflammatory reaction. The basis is treatment with bandages. For all wounds that heal by secondary intention, wet debridement is considered the standard treatment method. Dry debridement with the application of dry sterile wipes to the wound is used only for temporary covering of wounds and treatment of wounds that heal by primary intention.
Wet treatment uses bandages that create a moist environment in the wound. Osmotically active substances, antiseptics, and water-soluble ointments are used. Fat-soluble ointments are contraindicated as they interfere with the outflow of secretions. It is possible to use modern atraumatic dressings with high absorption capacity that maintain a certain level of moisture and help remove exudate from the wound and firmly retain it in the dressing. Modern combination preparations for local treatment of wounds contain immobilized enzymes - gentacycol, lysosorb, dalcex-trypsin.
Dressings should be changed with adequate pain relief. The frequency of changing dressings depends on the condition of the wound. Typically, 1-2 changes of dressings per day are required, hydroactive dressings such as Hydrosorb can remain on the wound for several days, the need to immediately change the dressing arises in the following cases: the patient complains of pain, a fever has developed, the dressing is wet or dirty, or its fixation is impaired. At each dressing, the wound is cleaned of pus and sequestration, necrosis is excised and washed with antiseptics. Chlorhexidine, sodium hypochlorite, dioxidine, lavacept, hydrogen peroxide, and ozonated solutions can be used to wash the wound. To accelerate necrolysis, proteolytic enzymes, ultrasonic cavitation, vacuum wound treatment, and pulsating jet treatment are used. Physiotherapeutic procedures include ultraviolet irradiation of the wound, electro- and phonophoresis with antibacterial and analgesic substances.
In the regeneration phase, the main goals of treatment are to continue the fight against infection, protect granulation tissue and stimulate repair processes. There is no longer any need for drainage. Dressings applied during the regeneration phase should protect the wound from trauma and infection, not stick to the wound and regulate the humidity of the wound environment, preventing both drying and excess moisture. Dressings with fat-soluble antibacterial ointments, stimulating substances, and modern atraumatic dressings are used.
After complete cleansing of the wound, secondary sutures or adhesive tape are indicated; for large defects, autodermoplasty is indicated. Unlike primary sutures, secondary sutures are applied to granulating wounds after the elimination of the inflammatory process. The goal is to reduce the volume of the wound defect and the entry point for infection. After 21 days, secondary sutures are applied only after excision of the formed scar tissue. In cases where it is impossible to compare the edges to close the defect, autodermoplasty is performed as early as possible - immediately after the inflammatory process has subsided.
In the phase of scar reorganization, the main goal of treatment is to accelerate epithelization and protect the wound from trauma. Since drying causes a crust to form, which slows down epithelization, and epithelial cells die with excess moisture, dressings should still keep the wound in a moderately moist state and protect against injury. Bandages with indifferent and stimulating ointments are applied. Sometimes physiotherapy is used - ultraviolet irradiation, laser, pulsating magnetic field.
· General treatment of purulent wounds includes antibacterial therapy, detoxification, immunotherapy, and symptomatic treatment.
Antibacterial therapy is used in phases 1-2 of the wound process. The drug must be prescribed taking into account the sensitivity of the wound microflora. Systemic administration of antibiotics is indicated; topical administration is not currently recommended. The initial empirical choice of antibacterial therapy, pending sensitivity results, should be directed against typical pathogens, which are staphylococci, streptococci and gram-negative aerobic bacteria.
Amoxiclav, levofloxacin are used, as a reserve - cefuroxime, ciprofloxacin, ofloxacin, and for bites - doxycycline. Treatment of staphylococcal wound infections with pathogen resistance requires the use of vancomycin or linezolid. For erysipelas, penicillins, azithromycin, and lincosomide are indicated. If the infection is caused by Pseudomonas aeruginosa, the drugs of choice are carbenicillin, tazocin, timentin, as well as 3rd generation cephalosporins and fluoroquinolones. In addition to antibiotics, bacteriophages are used in the treatment of purulent wounds.
Detoxification is used in the presence of systemic manifestations of the inflammatory process. Infusions of saline solutions, detoxifying solutions, forced diuresis, and in severe cases, extracorporeal detoxification are used.
Immunocorrective therapy can be specific (vaccines, serums, toxoids) and nonspecific. Tetanus toxoid, antitetanus and antigangrenous serum, antitetanus and antistaphylococcal gamma globulin are often used. Among the means of nonspecific immunotherapy in patients with purulent wounds, only immunomodulators are used, and only in the presence of immune disorders and always in combination with an antimicrobial drug, since they aggravate the course of the infection. Synthetic immunomodulators, such as diocephon and polyoxidonium, are the most promising. Polyoxidonium has the properties not only to restore the impaired immune response, but also to absorb toxins, and is also an antioxidant and membrane stabilizer. Usually prescribed 6 mg 2 times a week, a full course of 5-10 injections.
Symptomatic therapy includes pain relief, correction of organ and system disorders, and correction of homeostasis disorders. For pain relief, non-narcotic analgesics are usually used, however, in the early postoperative period, as well as in case of extensive injuries, narcotic drugs can be used. When the temperature rises above 39° C or fever against the background of severe diseases of the cardiovascular and respiratory systems, the prescription of antipyretic drugs is required.
¨ Prevention of infectious complications of surgical wounds
Surgical wounds are applied under conditions that minimize the risk of wound complications. In addition, before inflicting a wound, it is possible to prevent wound complications. Prevention of complications of surgical wounds includes:
· Preparation for surgery
Before a planned operation, a thorough examination of the patient is carried out, during which existing risk factors for wound complications are identified. When assessing the degree of risk, the patient’s age, nutritional status, immune status, concomitant diseases, homeostasis disorders, previous drug treatment, the condition of the tissue in the area of the proposed incision, and the type and duration of the upcoming surgical intervention are taken into account. The existing disorders are corrected and the patient is directly prepared for surgery, taking into account the requirements of asepsis.
During operations on the colon, as well as during extensive surgical interventions in extremely critically ill patients, selective intestinal decontamination is performed to prevent infectious complications. Selective intestinal decontamination reduces the risk of enterogenous infection resulting from the translocation of intestinal microorganisms. Typically a combination of an aminoglycoside or fluoroquinolone with polymyxin and amphotericin B or fluconazole is used.
With each day of hospital stay, the patient’s contamination with pathogens of hospital infections increases, so the stage of inpatient preoperative preparation should not be delayed unnecessarily.
· Careful adherence to surgical techniques
When performing surgery, careful handling of tissues, careful hemostasis, preservation of blood supply to tissues in the wound area, obliteration of the resulting “dead” space, comparison of the edges of the wound and their suturing without tension are necessary. The sutures should not be ischemic, but should ensure complete closure of the wound edges. Whenever possible, the suture material left in the wound should be absorbable and monofilament. In addition, the duration of the operation plays an important role. As it increases, the degree of wound contamination and tissue susceptibility to wound infection pathogens increases due to tissue drying, impaired blood supply, and reactive edema.
· Antibiotic prophylaxis
Antibiotic prophylaxis of infectious wound complications depends on the type of surgical procedure. In clean operations, it is indicated only in the presence of factors that adversely affect the course of the wound process, such as immunodeficiency states, diabetes mellitus, and taking immunosuppressants. For most clean and conditionally clean operations, as well as for contaminated interventions in the upper gastrointestinal tract, 1-2 generation cephalosporins, such as cefazolin or cefuroxime, can be used for antibiotic prophylaxis. For contaminated operations on the colon, biliary system and internal genital organs, the use of protected aminopenicillins or 1-2 generation cephalosporins in combination with metronidazole is indicated.
During perioperative prophylaxis, average therapeutic doses of antibiotics are used. The first dose of the drug is administered intravenously 30-60 minutes before the skin incision, usually during induction of anesthesia. If the operation lasts more than 2-3 hours, repeated administration of the antibiotic is required to maintain its therapeutic concentration in the tissues throughout the entire surgical procedure. In most cases, the duration of antibiotic administration does not exceed 24 hours, however, the presence of additional risk factors necessitates the need to extend prophylaxis to 3 days. For “dirty” interventions, a full course of antibiotic therapy is indicated, which should begin in the preoperative period.
· Antiseptic prophylaxis
Antiseptic prophylaxis involves the use of effective antiseptics at all stages of the operation, including for treating the skin, washing cavities, and subcutaneous tissue. General requirements for the antiseptics used: wide spectrum of action, high bactericidal activity, toxicological safety. To treat the skin, iodophors, chlorhexidine, and surfactants are usually used; for washing cavities, chlorhexidine, sodium hypochlorite, and dioxidine are used.
· Drainage of surgical wounds
Drainage of surgical wounds is carried out according to certain indications. It is necessary when it is impossible to obliterate the “dead space” formed after surgery, when there is a large area of the wound surface of the subcutaneous fat, when using artificial materials for plastic surgery of the aponeurosis, and in some other cases that create the preconditions for the formation of seromas. Drainage is also mandatory for radical excision of ulcers with suturing of the postoperative wound. Aspiration or flow-wash drainage is preferable, while proper care of the drainage system in the postoperative period is mandatory.
· Proper wound management in the postoperative period
Local cold is prescribed immediately after the operation, adequate pain relief, regular changes of aseptic dressings and drainage care are performed, and, if indicated, dialysis and wound evacuation, physiotherapy and other measures.
¨ Control of wound treatment
The effectiveness of wound treatment is assessed by the dynamics of general and local signs of inflammation. They focus on the subsidence of fever, leukocytosis, pain in the wound area, and normalization of the patient’s general well-being. During dressings, the condition of the sutures, the presence and extent of hyperemia and edema in the wound circumference, necrosis of the wound edges, the type of wound discharge and granulations are visually assessed. To monitor the course of the wound process in the treatment of drained wounds, instrumental research methods can be used.
An endoscopic method of examining the wound is used with simultaneous biopsy of subcutaneous fat for bacteriological examination. In this case, during dressing, an endoscope optical tube with end optics with a diameter of 3-6 mm is inserted through the drainage of the postoperative wound, the presence of wound exudate, areas of necrosis, and fibrin is assessed, then a biopsy is taken. The degree of contamination of wound tissue is determined using express methods, for example, phase-contrast microscopy. After taking a biopsy, the wound channel is filled with physiological solution to assess the correct location of the drains and the direction of the fluid flow during its jet injection.
Favorable endoscopic signs of the course of the wound process and indications for stopping drainage are: the presence of bright pink granulations, the absence of pus, necrosis, a significant amount of fibrin, tissue contamination below critical. Sluggish granulations, the presence of a large amount of exudate and fibrin in the wound, as well as high bacterial contamination require continued dialysis of the wound with antiseptic solutions.
After removal of the drainage systems, an ultrasound scan is indicated to assess the condition of the wound channel and surrounding tissues. Favorable ultrasound signs of the course of the wound process are:
· narrowing of the wound channel the next day after removal of the drainage tubes, its visualization in the form of a heterogeneous echo-negative strip by 3-5 days, absence of dilation and disappearance of the channel by 6-7 days;
· uniform echogenicity of surrounding tissues, absence of additional formations in them.
Unfavorable ultrasound signs of the course of the wound process are dilatation of the drainage channel and increased echogenicity of the surrounding tissues with the appearance of additional formations in them. These symptoms indicate the development of purulent-inflammatory wound complications even before the appearance of their clinical signs.
When treating a purulent wound, daily monitoring of the course of the wound process is necessary. With continued exudation and sluggish granulation, treatment adjustment is required. In addition to visual assessment of the condition of the wound and assessment of the severity of general clinical and laboratory symptoms, various methods are used to monitor the dynamics of the microbial landscape, the level of contamination and regenerative processes in tissues: bacteriological, cytological, modern high-precision gas-liquid chromatography, tests using enzyme systems and others.
Wound healing time and consequences
Healing a chronic wound is a long and complex process that can take from 1 to 3 months, depending on the depth and size of the wound. It should be borne in mind that epithelization of chronic wounds is very slow - no more than 1 cm per month. After complete epithelialization, the “new” skin increases its strength for another 6 months.
Recommendations for caring for the problem area are quite simple:
•protect the wound from compression and mechanical damage;
•change the bandage regularly (depending on the stage of healing and type of bandage);
•at the granulation stage - use dressings that accelerate healing.
Symptoms of non-healing wounds
•constant pain;
•converging edges of the wound;
•constant bleeding;
• “stuck” wound at one of the stages of healing for more than three weeks;
•often – unpleasant odor;
•conventional treatments do not help or help little.
These signs indicate that the regeneration processes in tissues are disrupted for one reason or another. For the treatment of chronic wounds, local treatment is not enough; comprehensive measures are required.
To achieve progress in healing, it is necessary to provide conditions for restoring the normal rate of regeneration. They largely depend on the cause of the chronic wound, but there are recommendations that are common to all situations.
The body needs to provide:
•balanced nutrition - in particular, the diet should be enriched with vitamins A and B, which stimulate tissue regeneration, and vitamin C, which promotes the production of collagen - a substance involved in the formation of connective tissue that closes the wound in the first stages;
•normal sleep mode – during sleep the regeneration process occurs more actively;
•protecting the wound and the area around it from external influences, such as rubbing, squeezing, etc.;
•wound ventilation – without air circulation, the wound will quickly fester.
More specific recommendations depend on the origin and nature of the wound.
Treatment of non-healing wounds taking into account their cause
When starting to treat injuries of this kind, it is necessary to understand the cause of their occurrence. Further actions will depend on this.
1. First of all, it is necessary to examine the wound for foreign bodies, necrotic tissue, and bleeding and, if necessary, clean it. Please note that it is strongly recommended not to remove foreign bodies yourself! Such attempts may cause additional tissue damage and increase the risk of infection. You need to seek help from a doctor.
2. If local blood circulation is impaired, it is necessary to eliminate the source of pressure on the tissue (change the position of the patient’s body with bedsores, wear looser clothes/shoes for “diabetic” wounds).
3. When treating trophic ulcers on the legs, it is necessary to use compression stockings or bandages - they will help “support” the blood vessels and normalize blood circulation, as well as “pull” the edges of the wound towards each other for faster healing.
4. In case of exhaustion and vitamin deficiencies, it is necessary to provide a normal balanced diet in order to provide the body with the necessary substances for tissue regeneration and the production of collagen - a substance that is actively involved in the early stages of the healing process and helps tighten the edges of the wound.
5.If you have diabetes (of any type), you need to monitor your blood glucose levels.
After creating optimal conditions for wound healing, you can begin to treat and treat it.