Choking or asphyxia is a pathological condition characterized by a drop in oxygen levels in the blood and tissues of the body and an increase in carbon dioxide. Attacks of suffocation can develop acutely or subacutely and are accompanied by symptoms of respiratory failure. Signs of choking include:
- Increased respiratory rate;
- Cyanosis of coli and mucous membranes;
- Participation in the breathing process of additional muscles;
- At a critical stage, convulsions develop, consciousness is impaired, up to coma;
- Death can occur as a result of cessation of respiratory and cardiac activity.
Diagnosis and treatment may depend on the cause of suffocation, but in any case, this condition requires immediate medical attention. The causes of asthma attacks can be diseases such as bronchial asthma, allergic edema, bronchiolitis. In other cases, the causes of choking in the throat are traumatic injuries, craniocerebral disorders, poisoning, etc. What kind of disease - choking in the throat - can be diagnosed by analyzing complaints, collecting anamnesis, conducting thorough research, etc. In real life, choking does not cause as much excitement as Palahniuk's books, but requires quick and precise measures to restore breathing. Many people know Palahniuk’s quotes from the book “Asphyxiation,” but, sadly, they do not know how to provide assistance in case of asphyxia. Asphyxia care may include:
- Oxygen inhalation;
- Conical or tracheotomy;
- Artificial ventilation;
- Drug treatment, etc.
The Yusupov Hospital provides assistance to patients around the clock. If it is necessary to provide assistance for asphyxia, the patient stays in the intensive care ward, which is equipped with all the necessary equipment, oxygen is centrally supplied, etc.
The cause of asthma attacks at night in the presence of bronchial asthma is often inadequate treatment. If the prescribed therapy helped control the disease for a long time, but suffocation still appears at night, it may be caused by the need to adjust the dose of the drugs.
Doctors at the Yusupov Hospital will select the correct and effective treatment, help improve your standard of living and improve your prognosis. At the Yusupov Hospital, the leisure time of patients is thought out, the best conditions have been created for the fastest possible recovery of patients.
Causes of suffocation
Bronchial asthma
The most common causes of attacks of severe shortness of breath are respiratory diseases.
Most often, suffocation develops with bronchial asthma. Attacks of difficulty breathing caused by primary bronchial hyperreactivity are the main clinical manifestation of this disease; they develop upon contact with allergens and physical stress, and are provoked by respiratory infections and psycho-emotional stress. The feeling of lack of air occurs at any time, often at night and in the morning. The number and severity of attacks may vary throughout the day. Shortness of breath is accompanied by a feeling of tightness in the chest, wheezing, and an unproductive cough. Mild suffocation goes away on its own; medications are used to relieve a severe episode of shortness of breath. With inadequate treatment, the attack sometimes drags on and status asthmaticus develops.
Bronchospasm
Choking, caused by narrowing of the airways, is common in a number of different diseases. The clinical picture of a bronchospastic condition resembles an attack of bronchial asthma. However, bronchospasm in other nosologies is secondary in nature, developing against the background of acute pathological processes or during exacerbation of chronic diseases. The main causes of secondary bronchoconstriction are:
- Respiratory infections.
Choking due to acute bronchitis and bronchiolitis often occurs in preschool children. In addition to difficulty breathing, there is a dry or productive cough, an increase in temperature to subfebrile or febrile levels, and signs of general intoxication. The phenomena of bronchial obstruction against the background of bronchial tuberculosis and pulmonary syphilis appear during stable remission of the underlying disease. - Chronic inflammatory processes.
COPD, chronic bronchitis, and bronchiectasis are characterized by a slowly progressive course, constant cough with sputum, and hemoptysis. Episodes of bronchospasm occur during exacerbation of the pathological process. - Allergic reactions
. The cause of severe bronchial obstruction is often various allergic reactions. Choking develops as a result of anaphylaxis when the allergen re-enters the body. Often found in insect allergies, serum sickness, and drug intolerance. - Autoimmune diseases.
Severe systemic lupus erythematosus, scleroderma, periarteritis nodosa may be accompanied by attacks of suffocation. With such pathologies, skin rashes, polyarthralgia, fever are observed, and the functions of the urinary, cardiovascular and other systems are disrupted.
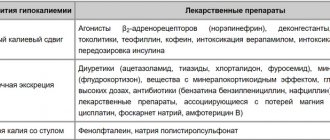
Less commonly, episodes of bronchospasm are found in cardiovascular insufficiency, thrombosis and embolism of the pulmonary artery, endocrine diseases (hypoparathyroidism, hypothalamic syndrome, Addison's disease). Inhalation of dust, irritants, poisoning with phosphorus compounds, and taking beta-blockers can also cause suffocation.
Injuries and diseases of the pleura
Violation of the integrity of the pleura, accumulation of air (pneumothorax) or fluid (hemothorax) in its cavity causes collapse of the lung, displacement of the mediastinum to the healthy side. Pulmonary excursion is limited, the great vessels are compressed. The severity of suffocation depends on the amount of pathological contents of the pleural cavity. Shortness of breath is accompanied by chest pain and dry cough.
Foreign body inhalation
A fairly common cause of sudden difficulty breathing in young children is aspiration of foreign bodies. Children tend to put various small objects in their mouths, which, when frightened, crying or laughing, enter the respiratory tract and can cause suffocation. Adults usually aspirate foreign objects due to disorders of chewing and swallowing functions or while intoxicated.
Clinical manifestations of aspiration depend on the size, shape and properties of the object that has entered the airways. Large foreign bodies in the larynx and trachea can stop the flow of air into the respiratory tract and lead to the death of the victim within a few minutes. A foreign object often partially blocks the lumen of the upper respiratory tract, and bronchial foreign bodies are less often detected.
The victim develops a painful reflex cough and inspiratory shortness of breath. The act of breathing involves auxiliary muscles. There is retraction of the intercostal spaces and epigastric region during inspiration. Breathing becomes stridorous, the skin becomes bluish.
Pathology of the larynx
Other common causes of suffocation in childhood are conditions leading to laryngospasm and acute laryngeal stenosis. Laryngospasm is a sudden involuntary contraction of the muscles of the larynx and is usually detected in children under 3 years of age against the background of spasmophilia. It can be caused by inflammatory diseases of the lungs, instillation of certain drugs into the nose. In adults, laryngospasm is rare and is observed with eclampsia, tetany, and inhalation of irritants.
Choking occurs suddenly. It is provoked by stress, crying, fear. Breathing becomes noisy. The patient turns pale and gasps for air with his mouth open. The head is thrown back, the neck muscles tense. There is a short-term cessation of breathing, which ends with a prolonged wheezing inhalation. The attacks may recur. Prolonged cessation of breathing is accompanied by convulsions and can be fatal.
Acute laryngostenosis is observed in infectious and inflammatory processes, tumors and injuries of the larynx. Other reasons for narrowing of the organ lumen include angioedema in the larynx, space-occupying formations of neighboring organs, and some diagnostic and therapeutic procedures. Asphyxia develops in stages, goes through the stages of sub- and decompensation, and in the absence of adequate assistance ends in the death of the patient from asphyxia.
Inhalation injury
Choking due to inhalation injury occurs due to thermal burns of the respiratory tract and poisoning by combustion products. Such injuries in fire victims aggravate the course of burn disease and cause high mortality. The presence of burns in the face and neck indicates the possibility of inhalation damage to the respiratory tract. Severe difficulty breathing is preceded by a change in voice timbre and coughing up soot.
The main toxic combustion products are carbon monoxide, cyanide, phosgene and chlorine, which causes suffocation, tightness and chest pain. There are signs of intoxication. The victim experiences excruciating headaches, nausea, and vomiting. In severe cases, hallucinations and delusions can occur, up to complete loss of consciousness.
Lack of air in the fetus and asphyxia of the newborn baby
Obstetricians-gynecologists note that such pathologies are the most common in their practice in children, from the 28th week of pregnancy to the seventh day after birth.
Fetal hypoxia is characterized by an increasing lack of oxygen while in the womb or during childbirth. The child develops a decrease in the supply of oxygen to the body, an increase in the concentration of under-oxidized toxic metabolic products in the blood, as a result of which metabolic and redox reactions are disrupted. The baby's respiratory center becomes more irritated, carbon dioxide accumulates, and the fetus has to breathe through an open glottis. With such breathing, all the elements and liquids located around it enter the body - this is blood, amniotic fluid, mucus.
Fetal hypoxia can occur against the background of impaired fetoplacental circulation, diseases of the pregnant woman, intoxication, the presence of extragenital diseases, umbilical cord pathologies, intrauterine injuries and infections, and genetic disorders. This condition can be detected by the presence of arrhythmia and deafness of heart sounds in the fetus. In the early periods of hypoxia, active movement of the fetus is observed, after which movements gradually become less frequent and slower. Asphyxia of the fetus and, subsequently, the child, becomes the cause of the development of intrauterine and birth disorders, defects, and pathologies.
Neonatal suffocation is characterized by the presence of cardiac activity in the absence of breathing, or with the presence of unproductive respiratory movements. For infants, it is especially important to take timely measures to restore normal respiratory activity - artificial ventilation, correction of metabolic disorders and energy balance.
Diagnostics
The diagnostic search is carried out by pulmonologists together with otorhinolaryngologists. Fire victims are being examined by surgeons. An attack of suffocation is diagnosed by characteristic clinical manifestations. Using a survey, the frequency of episodes of shortness of breath and precipitating factors are determined. To determine the cause of a pathological condition, the following are used:
- Endoscopic studies.
Endoscopic procedures for suffocation in some cases are therapeutic and diagnostic. During laryngoscopy, the larynx is examined and the trachea is intubated. Using bronchoscopy, foreign bodies are removed and the tracheobronchial tree is sanitized. - Visualization techniques.
Plain X-ray, CT, and MRI of the chest organs reveal inflammatory and neoplastic processes in the bronchi, pulmonary parenchyma, and pleural cavities. Ultrasound of the thyroid gland can identify formations compressing the trachea or larynx. - Functional studies.
Using pulse oximetry, the level of oxygen saturation in the blood is determined. An ECG helps confirm acute cardiovascular pathology. Spirography is performed for differential diagnosis of bronchial asthma with other respiratory diseases. - Laboratory tests.
To exclude specific damage to the lungs and parasitic infestations, bacteriological examinations of sputum are carried out, and serological diagnostics are carried out. Markers of cancer and autoimmune processes can be detected in blood serum. Pathological agents that provoke anaphylaxis are identified using allergy diagnostic methods.
Treatment
Help before diagnosis
Choking requires emergency medical care, the main goal of which is to restore airway patency. As a pre-medical measure, it is necessary to ensure an influx of fresh air - open the window, free the patient from restrictive clothing, take the fire victim outside. A foreign object in the respiratory tract should be tried to be removed using the Heimlich maneuver.
Conservative therapy
The choice of etiopathogenetic treatment tactics depends on the immediate cause of suffocation. For burn patients, therapeutic bronchosanitation is relevant; patients with cardiovascular pathology are prescribed cardiotropic drugs. In the treatment of diseases of the respiratory system accompanied by suffocation, the following groups of drugs are most often used:
- Bronchodilators.
Includes beta-agonists, anticholinergics, methylxanthines. Medicines can quickly relieve broncho- and laryngospasm. Drugs in this group are divided into fast-acting and long-acting. Beta-agonists and anticholinergics can be prescribed as a single drug, in combination with each other and with inhaled corticosteroids. - Corticosteroids.
They are used to provide emergency care to patients with bronchial obstruction, laryngospasm, and anaphylaxis. Topical inhaled forms of corticosteroids are used as basic therapy for bronchial asthma, COPD and other diseases of the respiratory system.
If necessary, oxygen therapy and respiratory support are provided. For anaphylaxis, epinephrine is administered. Patients with allergic diseases are prescribed antihistamines and antileukotriene drugs, and allergen-specific immunotherapy is performed. Infectious and inflammatory lesions of the bronchopulmonary system are treated with antibiotics.
How to avoid seizures?
If a person already has bronchial asthma, it is important for him to take medications prescribed by a doctor and follow his recommendations. Treatment should be continued even if there are almost no symptoms. If they worsen, if attacks become more severe or occur more often, you need to meet with your pulmonologist and get new prescriptions.
To prevent bronchospasm you need:
- Avoid triggers. To do this, it is important to know what exactly can cause an asthma attack. The risk of contact with a trigger cannot be completely eliminated, but it can be significantly reduced and its effects can be limited. For example, if an attack may be triggered by tobacco smoke, you can avoid places where there is smoking and try not to be around smokers.
- Use medications correctly. The attending physician may recommend using an inhaler, spacer, or nebulizer. Each of these devices, as well as each of the rapid-acting drugs for relieving bronchospasm, has specific application features. It is important to know about them and practice using the medicine correctly. An inhaler or other device to relieve an attack must be carried with you at all times.
- Monitor symptoms. Even before the onset of suffocation, increasing, gradually intensifying symptoms may occur. It’s good if a person knows how to recognize and track them. This helps to understand that bronchospasm is beginning. Headache, difficulty breathing, and allergy symptoms may indicate an approaching attack.
- Monitor your health. To ease the course of asthma, it is important to stop smoking and prevent excess weight. It is necessary to strengthen the immune system to reduce the risk of respiratory and viral diseases. Vaccination can also help with this. If an asthma attack is likely to be triggered by cold air, it is important to wear a scarf or bandage to cover your mouth and nose in cool weather.