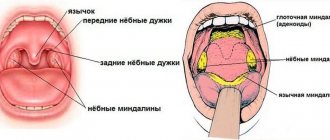
Aspergillosis - symptoms in humans, diagnosis and treatment
Aspergillosis is a disease that is caused by fungi of the Aspergillus family and is characterized by damage to various organs and systems of the body, but the bronchopulmonary system most often suffers.
The disease is usually chronic with various allergic reactions or toxic manifestations. The causative agent of aspergillosis is quite widespread in the environment - they are present in the ground, in water, and in the air, and can multiply in the human body and in animals.
Due to the fact that the respiratory system takes the first blow, the main symptoms of aspergillosis begin to appear in the respiratory system. Sometimes the fungus enters the body with blood and lymph, quickly spreading to all organs. This type of disease is characterized by a high mortality rate - about 80%.
Causes of aspergillosis
The causative agents of the disease belong to the genus Aspergillus, and in human pathology, A. Flavus and A. Niger are of greatest importance, but other species may also occur, for example, A. Nidulans or A. Fumigatus. We can say that morphologically, these types of fungi consist of the same type of mycelium, having a width of 4-6 microns. Aspergilli, as a rule, have quite high biochemical activity, due to which they can form various enzymes.
The causative agents of pulmonary aspergillosis are widespread in nature. They are most often found in hay, flour, soil and grain, as well as dust. The pathogen usually enters the body with dust through the air. By aerogenous route it reaches the mucous membranes located on the upper respiratory tract. It is quite possible to become infected through the skin, which is often changed by another pathological process.
A decrease in the body's immune defense plays a leading role in the development of aspergillosis. This disease can be complicated by various pathological processes of the skin, internal organs and mucous membranes.
Recommendations
- ^ a b
Bennett J. W. (2010).
"Overview of the genus Aspergillus
" (PDF).
Aspergillus : Molecular Biology and Genomics
. Caister Academic Press. ISBN 978-1-904455-53-0. - Geyser D.M. (2009). "The sexual structures of Aspergillus: morphology, significance and genomics". Medical mycology
.
47. 47
(Appendix 1): S21-6. Doi:10.1080/13693780802139859. PMID 18608901. - Hawksworth DL (April 2011). "Naming Aspergillus species: progress towards one name for each species". Medical mycology
. 49 Appendix 1 (S1): S70-6. Doi:10.3109/13693786.2010.504753. PMID 20718610. - Latge JP (April 1999). "Aspergillus fumigatus and aspergillosis". Clinical Microbiology Reviews
.
12
(2): 310–50. Doi:10.1128/CMR.12.2.310. PMC 88920. PMID 10194462. - “What are fungal spores?” University of Worcester
. Retrieved August 6, 2021. - "Pillows: a hot bed of fungal spores." Science Daily
. Archived from the original on 2017-10-08. Retrieved 2017-05-08. - ^ a b
Volume C, Church M (1926).
Aspergillus
. Baltimore: Williams and Wilkins Company. - Spiegel A (April 8, 2014). “Are you using soy sauce correctly? Here's how to find out." The Huffington Post
. Archived from the original on 08/06/2017. Retrieved 2017-07-29. ...to make soy sauce, you first add the Aspergillus mold to soybeans and grains to create a mixture called koji. - USA 6069146
- "GRAS Notice of Acid Lactase from Aspergillus oryzae
Expressed in
Aspergillus niger
." In the archive from the original dated March 23, 2016. Retrieved 2016-03-17. Section 2. - Wortman JR, Gilsenan JM, Joardar V, Deegan J, Clutterbuck J, Andersen MR, et al (March 2009). "Updating the Aspergillus nidulans genome annotation in 2008: a community effort." Fungal Genetics and Biology
. 46. 46 Suppl 1(1):S2-13. doi:10.1016/j.fgb.2008.12.003. PMC 2826280. PMID 19146970. - "Descriptions—Comparative Analysis of Aspergillus." Broad Institute. Archived from the original November 22, 2009. Retrieved 2009-10-15.
- ^ a b
Dyer PS, O'Gorman CM (December 2011).
"The fungal sexual revolution: Aspergillus and Penicillium show the way." Current Opinion in Microbiology
.
14
(6): 649–54. doi:10.1016/j.mib.2011.10.001. PMID 22032932. - O'Gorman CM, Fuller H, Dyer PS. (January 2009). "Opening of the sexual cycle in the opportunistic fungus Aspergillus fumigatus". Nature
.
457
(7228):471–4. Bibcode:2009Natura.457..471O. doi:10.1038/nature07528. PMID 19043401. S2CID 4371721. - Horn BW, Moore GG, Carbone I (2009). "Sexual reproduction in Aspergillus flavus". Mycology
.
101
(3):423–9. Doi:10.3852/09-011. PMID 19537215. S2CID 20648447. - Svilaiman SS, O'Gorman KM, Balaji SA, Dyer PS. (July 2013). "Opening of the sexual cycle in Aspergillus lentulus, a close relative of A. fumigatus". Eukaryotic cell
.
12
(7): 962–9. Doi:10.1128/EC.00040-13. PMC 3697472. PMID 23650087. - Arabatzis M, Velegraki A (2013). "Sexual reproduction in the human opportunistic microorganism Aspergillus terreus". Mycology
.
105
(1):71–9. Doi:10.3852/11-426. PMID 23074177. S2CID 9584227. - Malik S.B., Paitling A.V., Stefaniak L.M., Shchurko A.M., Logsdon J.M. (August 2007). "An expanded list of conserved meiotic genes provides evidence for sex in Trichomonas vaginalis." PLOS ONE
.
3
(8):e2879. doi:10.1371/journal.pone.0002879. PMC 2488364. PMID 18663385. - Heitman J, Sun S, James TY. (2013). "The Evolution of Fungal Sexual Reproduction". Mycology
.
105
(1):1–27. Doi:10.3852/12-253. PMID 23099518. S2CID 18167947. - Paoletti M, Seymour FA, Alcocer MJ, Kaur N, Calvo AM, Archer DB, Dyer PS. (August 2007). "Mating type and genetic basis of self-fertilization in the model fungus Aspergillus nidulans". Current Biology
.
17
(16): 1384–9. doi:10.1016/j.cub.2007.07.012. PMID 17669651. S2CID 17068935. - Dyer PS, O'Gorman KM. (January 2012). "Sexual development and cryptic sexuality in fungi: insights from Aspergillus species". FEMS Microbiology Review
.
36
(1): 165–92. doi:10.1111/j.1574-6976.2011.00308.x. PMID 22091779. - Rydholm C, Szakacs G, Lutzoni F (April 2006). "Low genetic variation and lack of detectable population structure in aspergillus fumigatus compared with closely related Neosartorya species." Eukaryotic cell
.
5
(4): 650–7. Doi:10.1128/EC.5.4.650-657.2006. PMC 1459663. PMID 16607012. - Machida M., Gomi K., eds. (2010). Aspergillus : Molecular Biology and Genomics
. Caister Academic Press. ISBN 978-1-904455-53-0. - Gibbons JG, Rokas A (January 2013). "Function and evolution of the Aspergillus genome". Trends in Microbiology
.
21
(1): 14–22. doi:10.1016/j.tim.2012.09.005. PMC 3534798. PMID 23084572. - Khaldi N, Wolfe KH (August 2008). Gadagkar S (ed.). "The Elusive Origin of Accessory Genes in Aspergillus oryzae". PLOS ONE
.
3
(8):e3036. Bibcode:2008PLoSO ... 3.3036 thousand. Doi:10.1371 / journal.pone.0003036. PMC 2515630. PMID 18725939. - Cloherty J (2012). Guide to Neonatal Care
. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. ISBN 978-1-60831-777-6; Access provided by the University of Pittsburgh. - Bozkurt M.K., Ozcelik T., Saidam L., Kutluay L. (2008). "[A case of isolated aspergillosis of the maxillary sinus]". Fist Burun Bogaz Ihtisas Dergisi
(in Turkish).
18
(1):53–5. PMID 18443405. - "Aspergillosis". MedScape. In the archive from the original dated 02/23/2014. Retrieved 2014-06-29.
- Wilson WR, Sande MA, Drew WL, eds. (2001). Current diagnosis and treatment of infectious diseases
. Lange Medical Books/McGraw-Hill. - Loper N (2020). "Map of a soapstone scarab from the Second Intermediate Period." Present aspirations of the past
.
Chicago: American Archaeological Association. 5
: 37–39. - Di Paolo N., Guarnieri A., Garosi G., Sacchi G., Mangiarotti A. M., Di Paolo M. (1994). “Inhaled mycotoxins lead to acute kidney failure.” Nephrology, Dialysis, Transplantation
. 9 Suppl 4: 116–20. PMID 7800243.
Classification
Aspergillosis differs in the localization of its pathological processes:
- bronchopulmonary (including pulmonary aspergillosis);
- aspergillosis of ENT organs;
- aspergillosis of the skin, eyes and bones;
- septic, or generalized aspergillosis.
Depending on the route of infection by fungi, several types of aspergillosis are distinguished:
- endogenous (autoinfection);
- exogenous (airborne or alimentary transmission);
- transplacental (vertical route of infection);
According to statistics, approximately 90 percent of all cases of aspergillosis occur due to primary infection of the respiratory tract, as well as the lungs. About five percent are due to infection of the paranasal sinuses. In addition, involvement of other human organs in the pathological process is diagnosed in almost five percent of people susceptible to infection.
Habitats, distribution conditions, use in production
Representatives of this genus of fungi live mainly in soil, on plants, on rotting vegetable debris, in house dust, building materials, fabric, leather, textiles and on food products such as cheeses and canned meats.
Spores of fungi of this genus are present in the air almost constantly: every day each of us inhales about several hundred spores, which do not cause any diseases in a person with a normal immune system. And sometimes fungi of the genus Aspergillus can be found in the oropharynx of a healthy person.
As already described above, fungal spores can be present in indoor air, including in the air of hospitals, which can become a risk factor for nosocomial infection of an inpatient with a weakened immune system.
A number of representatives of fungi are used in industry to obtain organic acids, antibiotics, vitamins, enzymes, and for the industrial production of certain food products.
Pulmonary aspergillosis
Pulmonary aspergillosis is a very serious diagnosis. Since, due to the development of the disease caused by the mold fungi Aspergillus, aspergillomas begin to form in the human lungs, that is, tumor-like formations that consist of tightly woven fungi. There are also complications such as endocarditis, aspergillus pleurisy, otitis, meningoencephalitis and others.
However, at any time, aspergilloma can cause a serious complication - pulmonary hemorrhage, which can be massive and profuse. And in this case, there is no alternative to surgical treatment. Treatment of aspergillosis with conservative methods is possible when the mucous membranes or skin are damaged by the fungus.
external reference
| Wikispecies has information related to Aspergillus |
- FungiDB: an integrated functional genomics database for fungi and oomycetes
- Aspergillus Genome Resources (NIH)
- Comparative Aspergillus Database Comparative Genomic Resource at Broad Institute
- Central Aspergillus Data Repository
- Fungal Genetics Foundation Center
- Aspergillus/Aspergillosis website Encyclopedia of Aspergillus
for patients, doctors and scientists - Aspergillus
surveillance project in a large tertiary care hospital. (PDF). - Aspergillus Genome Database
- Mold and mildew
| Taxon identifiers |
|
| Authoritative control |
|
Symptoms of aspergillosis in humans
Since the respiratory system takes the first blow, the main symptoms of aspergillosis in humans begin to appear precisely from the respiratory system. In a third of cases, the fungus enters the body through the blood and lymph flow and spreads to all organs. This type of aspergillosis has a high mortality rate of about eighty percent. The rarest is cutaneous aspergillosis.
If the fungus has settled on the surface and has not penetrated the mucous membrane, as happens with tracheobronchitis or aspergilloma, then patients note the following symptoms: chronic cough with sputum, sometimes with blood during a strained cough. Most often in such cases there are pathologies of the lungs.
In response to the penetration of spores into the body, human tissues develop certain inflammatory reactions. The most common two types of inflammation are serous-desquamative and fibrous-purulent. With serous-desquamative inflammation, aspergillus causes exfoliation of the epithelium, membranes of the stomach, and lungs with the release of exudate (plasma with blood elements). In the second type - fibropurulent - aspergillus causes the release of exudate with fibrin (clotted blood protein) and a purulent component. The most severe reaction to aspergillosis is the formation of granulomas in the lungs.
Otherwise, aspergillosis gives an acute picture - a dense infiltrate forms in the lungs, which disintegrates. With the blood flow, infection of other organs occurs. At the onset of acute aspergillosis, the phenomenon of neutropenia is characteristic, which is expressed in sudden weakness, nosebleeds, fever, sudden chills, severe sweating, tachycardia, and a sharp decrease in pressure. In this case, a decrease in neutrophils is detected in the blood, which makes it difficult for the body to give an inflammatory response to the focus of aspergillosis. Therefore, with neutropenia, it is often not possible to diagnose aspergillosis - all indicators would seem to be normal. However, doctors know from experience that this may signal the onset of aspergillosis, so additional studies are prescribed. Most often, aspergillus settles in the sinuses. In this case, red lesions appear; after the tissue disintegrates, they lose their color and then turn black. This process is very rapid - it usually spreads to the eye sockets, facial tissues, and towards the brain. Typical symptoms in this condition are congestion, pain in the nasopharynx, sinuses, swelling of the mucous membrane. The sinuses are filled with pus, but they do not rupture.
Allergic aspergillosis is often associated with bronchial asthma. In this case, patients note asthmatic attacks, increased eosinophils in the blood, dark areas on x-ray, and the presence of antibodies in the serum (galactoman). To clarify the diagnosis, a sputum analysis is taken. In more than half of patients, aspergillus is detected during culture. In this case, a secondary culture is done to clarify the diagnosis (since conidia could have been accidentally introduced).
Bibliography
- Centers for Disease Control and Prevention. Brucellosis. Parasites. Link
- Corbel MJ Parasitic diseases // World Health Organization. Link
- Young EJ Best matches for intestinal parasites // Clinical Infectious Diseases. — 1995. Vol. 21. - P. 283-290. Link
- Yushchuk N.D., Vengerov Yu.A. Infectious diseases: textbook. — 2nd edition. - M.: Medicine, 2003. - 544 p.
- Prevalence of parasitic diseases among the population, 2009 / Kokolova L. M., Reshetnikov A. D., Platonov T. A., Verkhovtseva L. A.
- Helminths of domestic carnivores of the Voronezh region, 2011 / Nikulin P. I., Romashov B. V.
An article for patients with a doctor-diagnosed disease. Does not replace a doctor's appointment and cannot be used for self-diagnosis.
The best stories from our readers
Topic: Parasites are to blame for all troubles!
From: Lyudmila S. ()
To: Administration Noparasites.ru
Not long ago my health condition worsened. I began to feel constant fatigue, headaches, laziness and some kind of endless apathy appeared. Problems also appeared with the gastrointestinal tract: bloating, diarrhea, pain and bad breath.
I thought it was because of the hard work and hoped that it would go away on its own. But every day I felt worse. The doctors couldn’t really say anything either. Everything seems to be normal, but I feel like my body is not healthy.
I decided to go to a private clinic. Here I was advised, in addition to general tests, to get tested for parasites. So in one of the tests they found parasites in me. According to doctors, these were worms, which 90% of people have and almost everyone is infected, to a greater or lesser extent.
I was prescribed a course of antiparasitic medications. But it didn’t give me any results. A week later, a friend sent me a link to an article where some parasitologist shared real tips on fighting parasites. This article literally saved my life. I followed all the advice that was there and after a couple of days I felt much better!
Digestion improved, headaches went away and the vital energy that I so lacked appeared. To be sure, I took the tests again and no parasites were found!
Anyone who wants to cleanse their body of parasites, no matter what types of these creatures live in you, read this article, I’m 100% sure it will help you! Go to article>>>
Still have questions? Ask them in our Anonymous group on VK
How to get rid of parasites in a week. The answer is here!
A reliable and effective remedy for combating worms. Removes all parasites in 21 days.
Go to website
Reviews
Read online
Symptoms that 100% indicate parasites! Take the Test.
How to rid your body of life-threatening parasites before it’s too late!
Read more
Website
To get a consultation
The doctor tells how to quickly get rid of parasites for adults and children!
A parasitologist explains what effective methods exist to combat helminths.
More details
Read completely
Comments
Search for cures for parasites
This service is a small help in finding cures for parasites. To start using it, select the type of parasite. If you don’t know what kind of parasite you are infected with, this parasite identification tool will help you by symptoms.
We recommend reading
Mosquito: description, types and characteristics, methods of feeding and reproduction
26.03.202126.03.2021red
How to cure Lyme disease
03/24/202103/22/2021ElenaKV
Centipede mosquito. Description, stages of development. What do big mosquitoes eat? Whether they bite or not. Damage from long-legged mosquitoes
24.03.202124.03.2021red
What do mosquitoes eat, besides blood, females and males, in the swamp and in nature?
23.03.202130.03.2021red
Diagnostics
Aspergillosis in adults requires a thorough and comprehensive diagnosis, which, first of all, is necessary to identify the type and severity of such a disease.
The first stage of establishing the correct diagnosis is carried out by the clinician to whom the person contacted, based on the predominant symptom. The doctor needs:
- get acquainted with the medical history and life history of the patient - this may indicate some etiological factors;
- conduct a detailed survey of the patient to find out the first time of onset and the degree of intensity of symptom expression. This will enable the clinician to determine the severity of the disease;
- perform a thorough physical examination, which, depending on the situation, may include an ophthalmological examination of the eyes, palpation of the anterior wall of the abdominal cavity, examination of the condition of the skin and nail plates, and listening to the lungs using a phonendoscope.
Instrumental diagnosis of aspergillosis includes:
- chest x-ray;
- biopsies;
- bronchoscopy;
- spirometry;
- CT.
Laboratory tests will also vary depending on the nature of the infection. In most cases, these include:
- study of discharge from the sinuses or external auditory canal;
- microscopic examination of feces;
- general blood test - may indicate the occurrence of an allergic or inflammatory process;
- analysis of sputum produced when coughing - to identify Aspergillus particles;
- blood biochemistry;
- scraping from the skin or nail plates;
- imprint from the surface of the cornea;
- PCR.
Such activities will help not only make the correct diagnosis, but also carry out a differential diagnosis of such a disease.
How to prepare a room for mold disinfection
Mold can affect hard-to-reach areas of the apartment (behind plumbing fixtures, furniture, pipelines). Therefore, prepare for the fact that you will have to move or take out furniture. Also, not all products are safe and tolerated by humans, even if protective measures are used. Therefore, adhere to the following rules.
- Mold often grows in corners where walls are most susceptible to freezing. If necessary, you will have to completely vacate them by removing furniture and unnecessary items.
- All utensils, food, and personal hygiene products must be removed from the premises. Anything that cannot be hidden must be well packed or covered with plastic.
- Be sure to remove animals from the rooms. If you have fish, cover the aquarium and turn off the air supply.
- After treatment with special means, it is better to leave the room for a period of several hours to a day and after the time has elapsed, check it well.
Treatment of aspergillosis
Regardless of the type of aspergillosis in a person, treatment is a very labor-intensive task. Chemotherapy and antibacterial agents do not lead to the expected effect, as indeed do all other methods of combating infectious diseases known to doctors.
For this reason, in recent years, when aspergillosis is diagnosed, treatment is based on the use of surgical methods. Patients undergo a lobectomy with resection of the affected organs. If the operation was performed by a competent specialist in compliance with all established procedures, the intervention is tolerated without complications and gives a good prognosis for the future.
For advanced forms of pulmonary aspergillosis, surgical treatment is used in conjunction with conservative methods. Patients with aspergillosis are prescribed amphotericin B, oxacillin, nystatin, erythromycin, and tetracycline antibiotics. At the same time, the person takes vitamins. Also, for patients with aspergillosis, restorative treatment is recommended.
When using antifungal drugs, the amount of antibodies in the blood increases sharply, but by the end of treatment it returns to normal. If pulmonary aspergillosis leads to lesions of the skin and mucous membranes, patients are recommended to take antifungal and anti-inflammatory drugs.
further reading
- Du C, Lin SK, Koutinas A, Wang R, Dorado P, Webb C (November 2008). "Wheat biological refining strategy based on solid-state fermentation for enzymatic production of succinic acid." Bioresource technologies
.
99
(17):8310–5. doi:10.1016/j.biortech.2008.03.019. PMID 18434138. - Zirbes JM, Milla CE (June 2008). "Steroid-sparing effect of omalizumab in allergic bronchopulmonary aspergillosis and cystic fibrosis." Pediatric Pulmonology
.
43
(6): 607–10. Doi:10.1002/ppul.20804. PMID 18433040. S2CID 25806792. - Asan A. (February 10, 2015) [2004]. "Aspergillus, Penicillium and related species reported in Turkey" (PDF). Mycotaxon
.
89
(1): 155–7. - Soltani J (2016). "Diversity of secondary metabolites of the genus Aspergillus". Recent Advances New and Future Developments in Microbial Biotechnology and Bioengineering: Properties of the Aspergillus System and Its Applications
. pp. 275–292.
Prognosis and prevention
The most favorable course is observed with aspergillosis of the skin and mucous membranes. The mortality rate from pulmonary forms of mycosis is 20-35%, and in people with immunodeficiency - up to 50%. The septic form of aspergillosis has a poor prognosis.
Measures to prevent infection with aspergillosis include measures to improve sanitary and hygienic conditions: combating dust in production, wearing personal protective equipment (respirators) by workers in mills, granaries, vegetable stores, weaving enterprises, improving ventilation of workshops and warehouses, regular mycological examination of persons from risk groups.
Alternaria alternata
The shade of this mold directly depends on its habitat and can be dark gray, greenish, or black. It forms on a damaged part of a plant, an overripe vegetable or fruit, or on a normal soil surface. The spores take root well on food and quickly infect seeds and plants. Fungal particles can be located both outdoors and indoors, focusing on dust. However, the risk of occurrence is greater in closed spaces with high humidity. Wooden houses are more quickly affected by the parasite than concrete or stone ones. The released toxins lead a weakened body to the development of asthma, acute dermatitis and other diseases.